The present study shows similar perioperative routines in Nordic centers performing NU among the majority of the examined subjects on the treatment of UTUC.
The extent of adherence to EAU guidelines concerning diagnostic practice was high. Five out of 6 examined components recommended by EAU as a part of the diagnostic practice, were adopted by ≥ 72% of the participating centers. This differs from other studies on implementation of guidelines on disease management in European countries [4, 5, 7] and other international studies [8, 9]. An online survey proposed to physicians in the field of bladder cancer from nine European Countries found that up to 45% of high-risk disease did not receive a re-TURB and adjuvant instillation. This despite the fact that 87% of participants declare to follow EAU guidelines [4]. On the other hand, the current findings are similar to a prior survey in the Nordic countries for the general management of radical cystectomy and adherence to enhanced recovery protocols and EAU guidelines [10].
The EAU guidelines recommend that patients identified as being at risk of for Lynch syndrome should undergo DNA sequencing and family counselling, but there is no specified follow-up program for UTUC fore these patients in the guidelines.
Under half of the participating centers follow EAU guidelines concerning DNA sequencing for patients that are highly suspected of having Lynch syndrome. This survey did not address whether participants use the Amsterdam criteria when screening for Lynch syndrome, or what reason participants have for not following guidelines. National guidelines vary on the subject of offering DNA sequencing for Lynch syndrome [5, 11], which might be a part of the explanation for the lack of implementation of this part of the EAU guidelines.
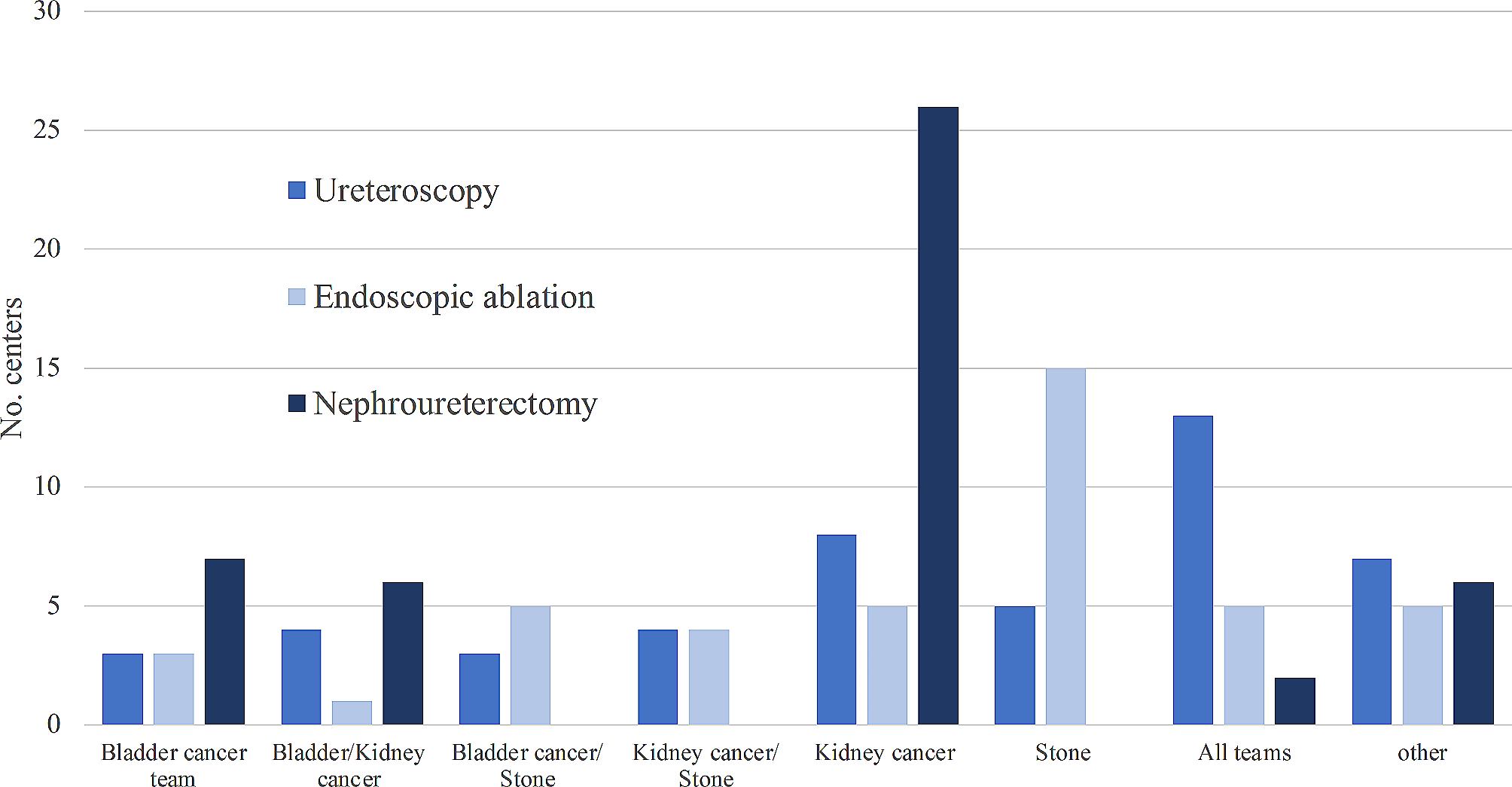
The disease management in the Nordic countries is less uniform compared to the diagnostic practice for UTUC and treatment of bladder cancer [10]. EAU guidelines recommend endoscopic treatment for low-risk tumors and ureteral resection for low-risk tumors not eligible for endoscopic treatment, as well as high-risk tumors limited to distal ureter and other high-risk tumors when preservation of renal function is imperative. However, the majority of participating centers treat ureteral tumors by segmental resection, however most centers do not select eligible patients as recommended by EAU guidelines. This finding could in part be explained by the low incidence of ureteral tumors, combined with the lack of high evidence studies on the subject [12,13,14].
The survey also addressed if participating centers performed LND, although we did not ask to distinguish between low- and high-risk tumors, therefore wording of this question is not specific enough to determine adherence of guidelines on this subject. On the other hand, we asked participants if they carry out template-based LND concomitant to NU in all cases or only when lymph node metastasis was suspected clinically (cN+).
The EAU guidelines recommend LND offered to all patients who are scheduled for NU for high-risk non-metastatic UTUC, but the authors draw attention to the current lack of evidence of benefit in case of < T2 UTUC [8, 15, 16]. In proposed flowchart for disease management, high-risk UTUC is recommended treated by NU “+/- LND”, and not “+ LND”. To our knowledge, no randomized studies exists and prior studies have produced conflicting results [8, 15,16,17,18,19,20,21].
Internationally there is no consensus on indication for LND, which leave room for individual interpretation.
The lack of adherence to LND in approximately two-third Nordic centers is comparable to findings by others [16,17,18], and may be attributable to the absence of clear indications for LND. On the other hand, an ongoing prospective LND-trial in seven Nordic hospitals might have contributed to that some centers reported use of LND concomitant to NU. Instead, we investigate if participants use cN+, as a preoperative surrogate for tumor stage > pT1 as criteria for doing LND, as this practice seems to be supported by node positive disease as a trigger for adjuvant systemic therapies for UTUC [22]. Studies on usage of topical agents in the upper urinary tract for treatment of CIS and small low-grade tumors is mentioned in the EAU guidelines. The guideline members state that further research is needed and from existing evidence, treatment is with questionable efficacy. The same is true for neoadjuvant chemotherapy, but use adjuvant chemotherapy is strongly recommend to for high-risk non-metastatic UTUC [2]. Our study shows low adherence to this latter recommendation as the majority administer adjuvant chemotherapy only in selected cases. However, one might suspect that at least centers who use adjuvant chemotherapy “in selected cases” routinely do consider giving adjuvant chemotherapy but refrain due to postoperative carboplatin-ineligibility related to renal insufficiency. Alternatively, it is possible that some participants by “selected cases” mean high-risk UTUC as recommended by guidelines. Due to non-specific wording of the question, this cannot be further examined from current data.
Among surveyed Nordic centers 43% (17/47) performs > 10 NU/year. This might imply a higher degree of centralization of complex surgical procedures in the Nordic countries compared to in the US, as Sui et al. found that hospitals that performed > 6 NU/year represented only 9% of all included hospitals, while majority (71%) performed less than 3 NU/year and with an overall range of surgical volume, extending from 0.8 to 30.1 NU/year [23].
It is well established that hospital volume represents an important outcome determinant for several surgical treatments including urological [23,24,25,26,27,28,29]. Other studies claim that observed benefit on outcome is largely mediated by surgeon volume [26] and high procedure-specific volume [23, 30].
Sui et al. and Tinay et al. have shown that patients treated at centers performing > 6 NU/year who had a shorter length of stay (LOS) [31] and were more likely to receive intravesical chemotherapy perioperative [23]. However, the observed difference between the two groups was small.
As seen in Fig. 4b, low volume centers were less likely to administer intravesical chemotherapy in our survey, but the association was tested and found independent. Likewise, our data shows no association between surgical volume and estimated LOS in the survey. The different finding from our study compared to a US population-based study [31] could be explained by an inadequate number of participants in the current survey or the fact that LOS is estimated in this survey.
Only 64% based their answers on registries or local data collection.
Limitations
As for all survey studies, there is a risk of inconsistencies between the responses and the actual practice patterns, recall/-reporting bias due to the wording of questions and the questions used in the survey were not validated. The selection of invited participants was made solely based on the knowledge by the representatives of NUCG. Additionally, it is not possible to conclude from which time period responses referred to or that the validity of the responses can be questioned, as one third of responding participants state that they do not register operative data on UTUC. As inclusion criteria centers were believed to perform NU, data might be missing on organ sparing procedures if some Nordic centers perform these treatments but not NU. For parameters like surgical volume and LOS, shorter numerical intervals would have made the data more comparable to other studies and might have enlightened a hospital-volume-outcome relationship.
As no power and sample size estimations was done, the interpretations of statistical analyses should be done with caution. Despite these limitations, we believe this study adds information and basis for further studies on treatment of UTUC in the Nordic countries.






留言 (0)