In recent years, the incidence of prostate cancer has increased year by year, seriously affecting the health and quality of life of patients, the complications after radical prostate cancer surgery mainly include urinary incontinence and sexual dysfunction, but inguinal hernia is also one of the common complications [16]. Liu L et al. found that open radical resection for prostate cancer technique and advanced patient age, especially those over 80 years old, are associated with a higher incidence of IH. Appropriate prophylaxis during surgery should be evaluated in high-risk patients [17].In some regional studies, low BMI has been identified as a risk factor for IH, and the risk threshold for BMI has not been determined, which is about BMI < 25 kg/m2 [18]. However, a number of studies have found that low BMI does not increase the risk of postoperative IH [19, 20]. At present, there is no uniform conclusion on the risk of IH between open radical resection for prostate cancer and laparoscopic radical prostatectomy. The study of Alder R scholars believed that the incidence of IH after laparoscopic radical prostatectomy was relatively low [21], while Otaki T’s study shows that the incidence of IH after laparoscopic radical prostatectomy is 7.3% and that of open radical resection for prostate cancer is 8.4%, showing no statistical difference between them [20]. There is no consensus on whether pelvic lymph node dissection is a risk factor for inguinal hernia [14, 15]. In short, the specific mechanism of inguinal hernia after radical prostate cancer surgery is unclear.
This study retrospectively analyzed the clinical data of 251 cases treated in our hospital, and found that the overall incidence of inguinal hernia was 14.7% (37/251), which was consistent with most of the current research results. We also found that the average time of occurrence of inguinal hernia after surgery was 8.58 ± 4.12 months, which provided certain guidance for our postoperative follow-up time.
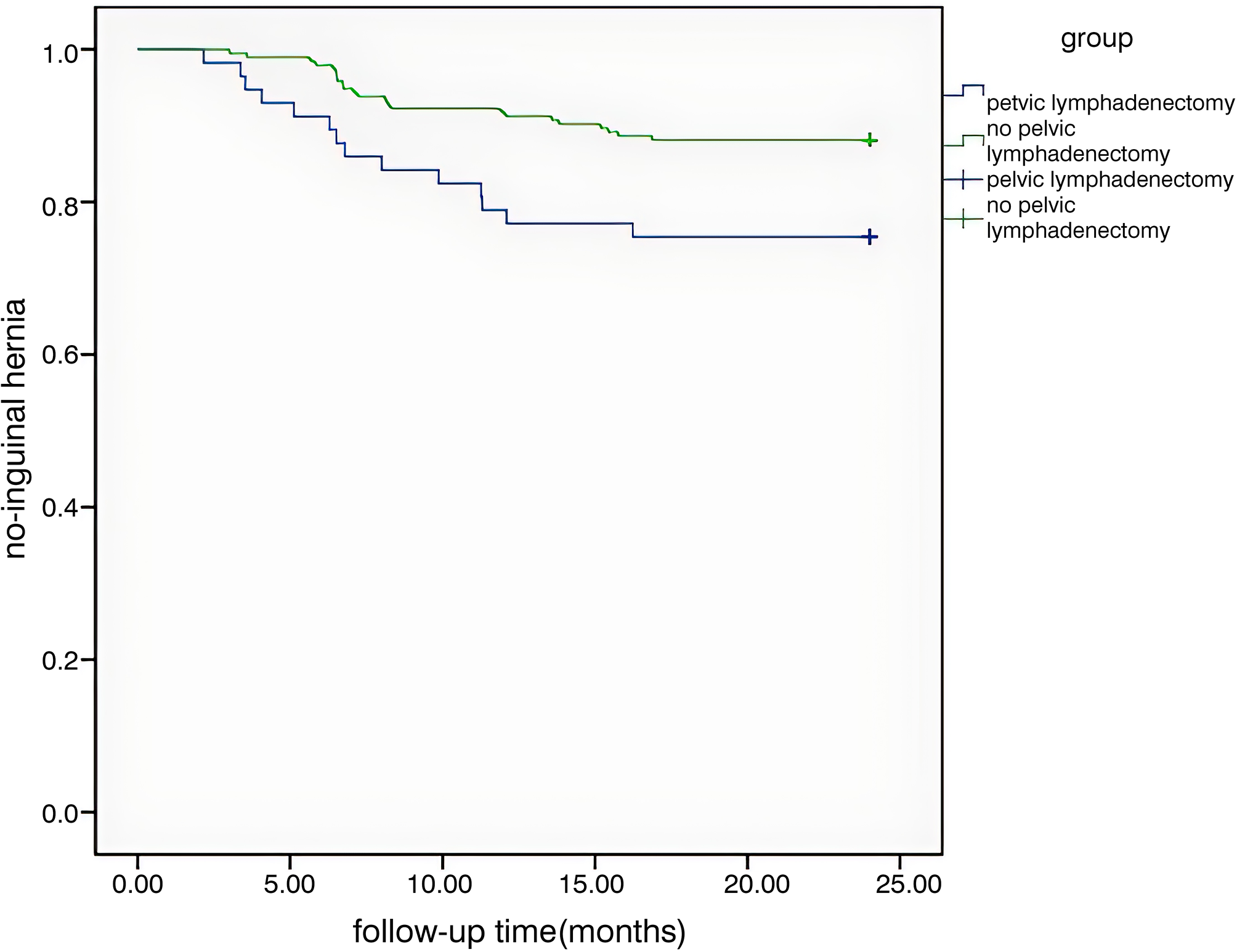
In this study, through Logistic multivariate analysis, it was found that pelvic lymph node dissection was a risk factor for inguinal hernia after prostate cancer surgery (OR = 0.413, 95%Cl: 0.196–0.869, P = 0.02). There was no statistical significance in age, BMI, hypertension, diabetes, PSA value, previous abdominal operations, operation method, operative approach and the occurrence of inguinal hernia after prostate cancer surgery (P > 0.05),but there were statistically significant differences with surgical method and pelvic lymph node dissection (P < 0.05). Therefore, the advantages and disadvantages of pelvic lymph node dissection should be reasonably evaluated for low-medium-risk prostate cancer patients, so as to avoid the occurrence of inguinal hernia. By drawing Kaplan-Meier survival curve, it was found that the rate of inguinal hernia in the group receiving pelvic lymph node dissection was significantly higher than that in the control group. Some studies believe that pelvic lymph node dissection during radical resection of prostate cancer operation will cause postoperative scar contraction in the inguinal region, resulting in an increase in abdominal pressure outward and downward, resulting in an increase in the incidence of inguinal hernia. Lodding P designed a comparative study between the group of radical resection of prostate cancer plus pelvic lymph node dissection, the group of pelvic lymph node dissection and the group without operation. They found that the incidence of inguinal hernia in the three observation groups was 13.6%, 7.6% and 3.1%, respectively, and the difference between the prostatectomy group and the group without operation was statistically significant. There was no significant difference between the group and pelvic lymph node dissection group. This result implies that pelvic lymph node dissection is an important factor in the development of inguinal hernia [22]. Another Sun M study compared the incidence of inguinal hernias after radical prostate cancer surgery and pelvic lymph node dissection alone, and showed that the risk of inguinal hernias increased by 6.8% and 7.8% at 5 and 10 years, respectively, in the radical prostate cancer resection group compared with the pelvic lymph node dissection group [23]. Niitsu H et al. believed that pelvic lymph node dissection during radical resection of prostate cancer might damage the pectineal foramina, while inguinal hernia originated from the defective pectineal foramina [14].
Shimbo M et al. found that due to prostatectomy and vesicourethral anastomosis, preoperative and postoperative sagittal MRI images showed that the rectovesical excavation (RE) was moved downward by about 2 to 3 cm [24]. Accordingly, they speculated that due to the displacement of RE, the peritoneum and vas deferens after urethrovesical anastomosis were pulled, which further pulled the opening of the inner ring and caused it to shift medially, which led to the occurrence of postoperative IH. Based on this theory, many scholars have prevented the occurrence of hernia after operation by reducing the tension of peritoneum and vas deferens at the inner ring and ligation and rupture of sheathing process. Several other articles have reported the role of preserving the retropubic space (RS) in preventing IH after radical resection of prostate cancer. Chang KD et al. found that robot-assisted laparoscopic radical prostatectomywith retained Retzius space significantly reduced the incidence of postoperative IH compared with standard robot-assisted laparoscopic radical prostatectomy [25]. In addition, the study of Matsubara et al. also showed that compared with standard open radical resection for prostate cancer, the incidence of IH after transperineal radical resection of prostate cancer with retained anatomical structures such as the Retzius space was lower [26]. Therefore, urological surgeons can take some effective measures in the operation to prevent the recurrence of inguinal hernia.
In this study, we identified risk factors for inguinal hernia after pelvic lymphadenectomy for prostate cancer. Other risk factors such as age, BMI, hypertension, diabetes mellitus, PSA value, history of abdominal surgery, operative method, operative approach were not significant in multivariate analysis, which was inconsistent with the results of Iwamoto H et al [27]. They found that dilatation of the right internal inguinal ring and different manipulation of the medial peritoneal incision of the ventral femoral ring were independent risk factors for IH after laparoscopic radical prostatectomy. The reason why postoperative IH occurs more often on the right side is not known. Alder R et al. found that the incidence of IH after open radical prostate cancer treatment was significantly higher than laparoscopic radical prostate cancer treatment [21], but our study did not show a difference between the two groups, possibly due to the small number of cases included in open radical prostate surgery.
In summary, the incidence of inguinal hernia after radical prostate cancer surgery is relatively high, and the specific cause is still unclear. Our study shows that pelvic lymph node dissection is a risk factor for inguinal hernia.
Limitations
The sample size of this study is small, and it belongs to a single-center study, so the representativeness of the research conclusions may not be strong. This time, we followed up the samples for 2 years, which was not long enough and may have overlooked the real incidence of inguinal hernia. In addition, this study is a retrospective study, and the clinical parameters observed are not very comprehensive, which may ignore the influence of other factors on the IH. Because our data is derived from clinical data, some data cannot be detected. These problems need further study by more scholars.






留言 (0)