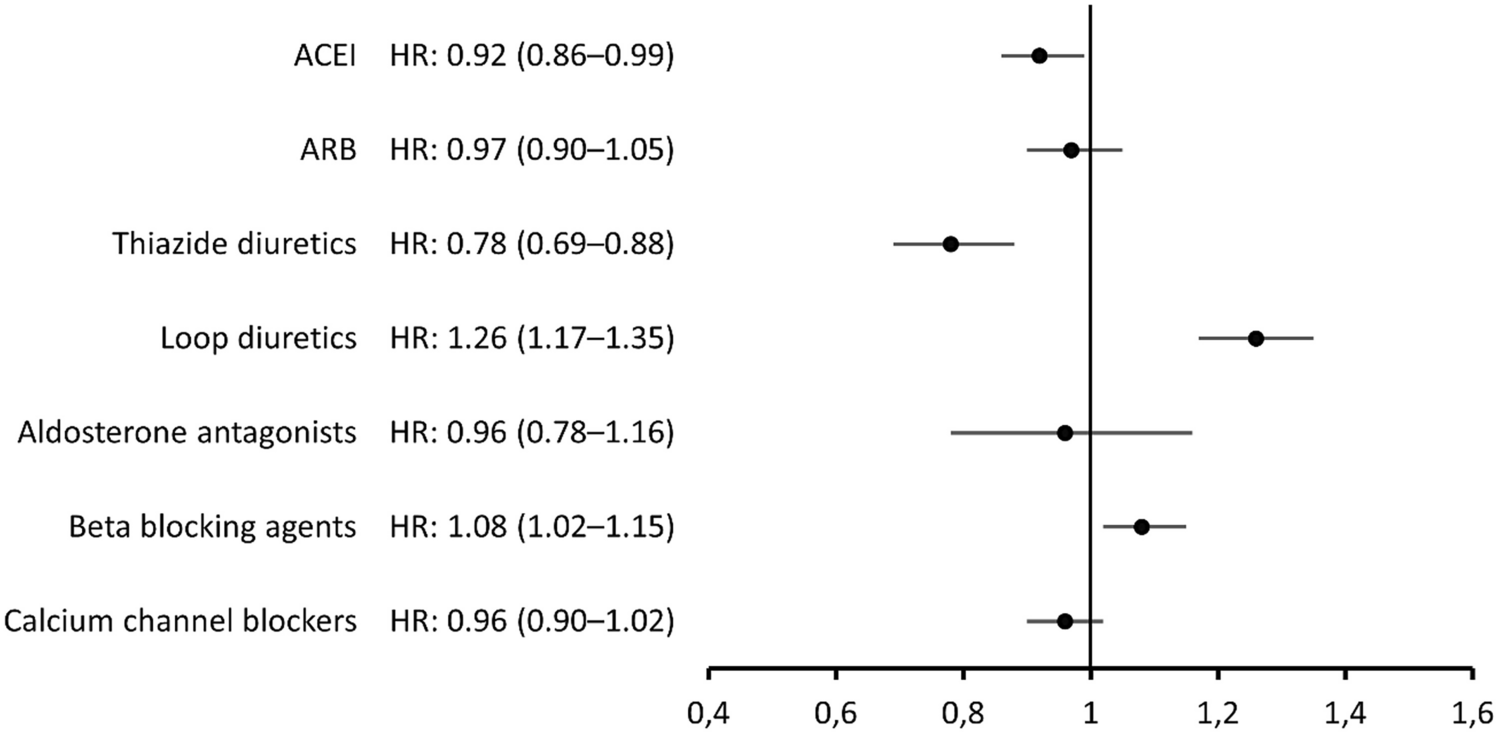
In this study, we have used nationwide record linked register data from nearly four million persons 50 years and older, to assess the association between the use of different types of drugs used to treat hypertension or heart failure, and the risk of death in COVID-19 during the start of the first SARS-CoV-2 wave in Sweden. The main findings were that the use of loop diuretics was associated with a higher risk of death in COVID-19, while the use of thiazide diuretics was associated with a reduced risk. We also observed a slightly lower risk of death with ACEI and a slightly higher risk with beta-blocking agents.
Our results support previous findings that people who use ACEI or ARB are not at higher risk of dying in COVID-19 [4,5,6, 9,10,11, 13]. Instead, our results for ACEI suggest, although the association was weak, that these drugs may have a protective effect against poor outcome in COVID-19, also in agreement with a number of studies [4,5,6, 9, 10].
However, a more pronounced negative association with the risk of death in COVID-19 was observed for thiazide diuretics. This is in line with two previous studies reporting associations between thiazide use and a lower risk for COVID-19 [8] and severe COVID-19 disease [15].
The other main finding of the present study was that people who used loop diuretics were at higher risk of death in COVID-19. In one earlier descriptive study at the NBHW, we found loop diuretics to be one of the drug groups being most over-represented among persons who were either treated in ICU for, or died from, COVID-19, compared to the general population in the same age range [16]. This led us to hypothesise that the use of loop diuretics may increase the risk of COVID-19 with poor outcome. This hypothesis is supported by the present study, where the association with loop diuretics was analysed taking a wide range of possible confounders into account.
Guragai and colleagues investigated the effects of baseline diuretic use on the prognosis in patients admitted to hospital with COVID-19 and found no significant difference between users and non-users, in COVID-19 severity or mortality [18]. However, their study was small and did not differentiate between the different types of diuretics. To our knowledge, only one study has specifically examined the association between the use of loop diuretics and the outcome in COVID-19. This was a population-based case–control study from the Italian Lombardy region, on 6272 patients with confirmed COVID-19 and 30,759 matched controls [12]. They found no significant association with risk for COVID-19 overall, or among patients who had a severe or fatal course of the disease, for ACEI, ARB, beta-blocking agents, calcium channel blockers, thiazides or aldosterone antagonists. By contrast, an increased risk was observed for loop-diuretics (OR 1.46; 95% CI 1.23–1.73). The authors judged, however, that this finding was likely to be explained by the fact that the use of loop diuretics reflects the existence of clinical conditions such as heart failure or advanced renal damage, rather than an effect of the drugs per se.
The present study largely corroborates their findings [12], pointing towards an increased risk of death in COVID-19 in users of loop-diuretics, and this was observed in an analysis adjusted for a broad range of possible confounders, including heart failure and kidney disease/failure.
Moreover, as regards heart failure, we obtained an even stronger result in patients without this diagnosis. One may also argue that, if the presence of heart failure would explain the association with loop diuretics, some of the other drugs that are more closely related to treatment of heart failure, i.e. ACEI, ARB, beta blocking agents and aldosterone antagonists, would have been associated with an increased risk in our analysis. We did observe a positive association with beta-blocking agents, indicating an increased risk, but this was weak and for the other drug groups no such association was seen.
As to advanced renal failure, this diagnosis is reportedly uncommon among users of loop diuretics, compared to heart failure and other cardiovascular diseases [19]. Further, similar to the results for heart failure, we observed a higher HR for loop diuretics in patients without a diagnosis of kidney disease/failure.
Clearly, as the present study is observational, it cannot prove causality and we cannot exclude the possibility of confounding by factors that have not been accounted, or properly adjusted, for in the analysis. However, if our results would reflect a causal relationship between the use of loop diuretics and increased risk of death in COVID-19, there are several plausible mechanisms for this. Saheb Sharif-Askari and colleagues [20] examined the effects of common drugs, including the loop diuretic furosemide, on the expression of SARS-CoV-2 entry receptors in kidney tissue. They did not find that furosemide increased the expression of ACE2, but instead the opposite. However, although this could reduce the entry of the SARS-CoV-2 virus, a downregulation of ACE2 may still worsen the prognosis in COVID-19, as there is evidence that the ACE2 enzyme also has organ protective functions in hypertension, diabetes and cardiovascular disease, as well as against acute respiratory distress syndrome (ARDS) [21]. In fact, the SARS-CoV infection per se can downregulate ACE2 expression, which may contribute to multiple organ injury in COVID-19 [22, 23].
Moreover, the study by Saheb Sharif-Askari et al. [20] showed that furosemide was one of the drugs that increased the expression of the transmembrane protease serine 2 (TMPRSS2), as well as being the top upregulating drug for the transmembrane glycoprotein CD147. TMPRSS2 acts by priming the virus spike protein, necessary for the virus-host cell membrane fusion and cell entry [24] and CD147 has been shown to play a functional role in facilitating invasion of host cells by SARS-CoV [25, 26].
Another possible mechanism for an increased risk of death in COVID-19 in loop diuretic users is QTc-prolongation and the subsequent risk of ventricular arrhythmias. Studies have demonstrated that QTc-prolongation is more frequent in COVID-19 patients and may be important for the outcome of the disease. A single-centre cohort study of patients hospitalised with COVID-19 [27] found that 9.8% had a prolonged QTc-interval on admission, which was independently associated with a higher mortality, even after adjustment for treatment with hydroxychloroquine and azithromycin. Another single-centre cohort study, of patients admitted to the hospital for COVID-19, showed that the QTc-intervals on presentation with COVID-19 were longer than in ECGs taken before the disease. This was seen in both those who survived and died with COVID-19, but the prolongation was more marked in the deceased patients [28].
The use of loop diuretics may be of importance for this QTc-prolongation. In a systematic review of 10 observational studies, Vandael et al. [29] found that the use of diuretics was — together with hypokalaemia, antiarrhythmic drugs and specific QTc-prolonging drugs — a factor with ‘very strong evidence’ for being a risk factor for QTc-prolongation. Moreover, in an earlier study of 900 consecutive patients admitted to cardiac care units, loop diuretics were found to be one of the independent predictors of QTc prolongation [30].
It is interesting to note that the two types of diuretic drugs — thiazides and loop diuretics — were found to have opposite associations with death in COVID-19 in our analysis. Our present results, suggesting a potential protective effect of thiazides, are in line with previous findings. Hippisley-Cox et al. [15] observed a decreased risk with thiazides for severe COVID-19 disease, while Rezel-Potts and colleagues [8] reported lower odds of COVID-19 diagnosis, but not mortality, in COVID-19, when using thiazides.
Our findings are further supported by a recent Spanish retrospective cohort study of 15,968 patients hospitalized with COVID-19. In the study, which aimed to find effective treatments among drugs used for other indications, 21 drugs out of a total of 864 treatments were found to be associated with improved patient survival, among them hydrochlorothiazide. In contrast, only one drug — the loop-diuretic furosemide — was associated with an increase in patient mortality [31].
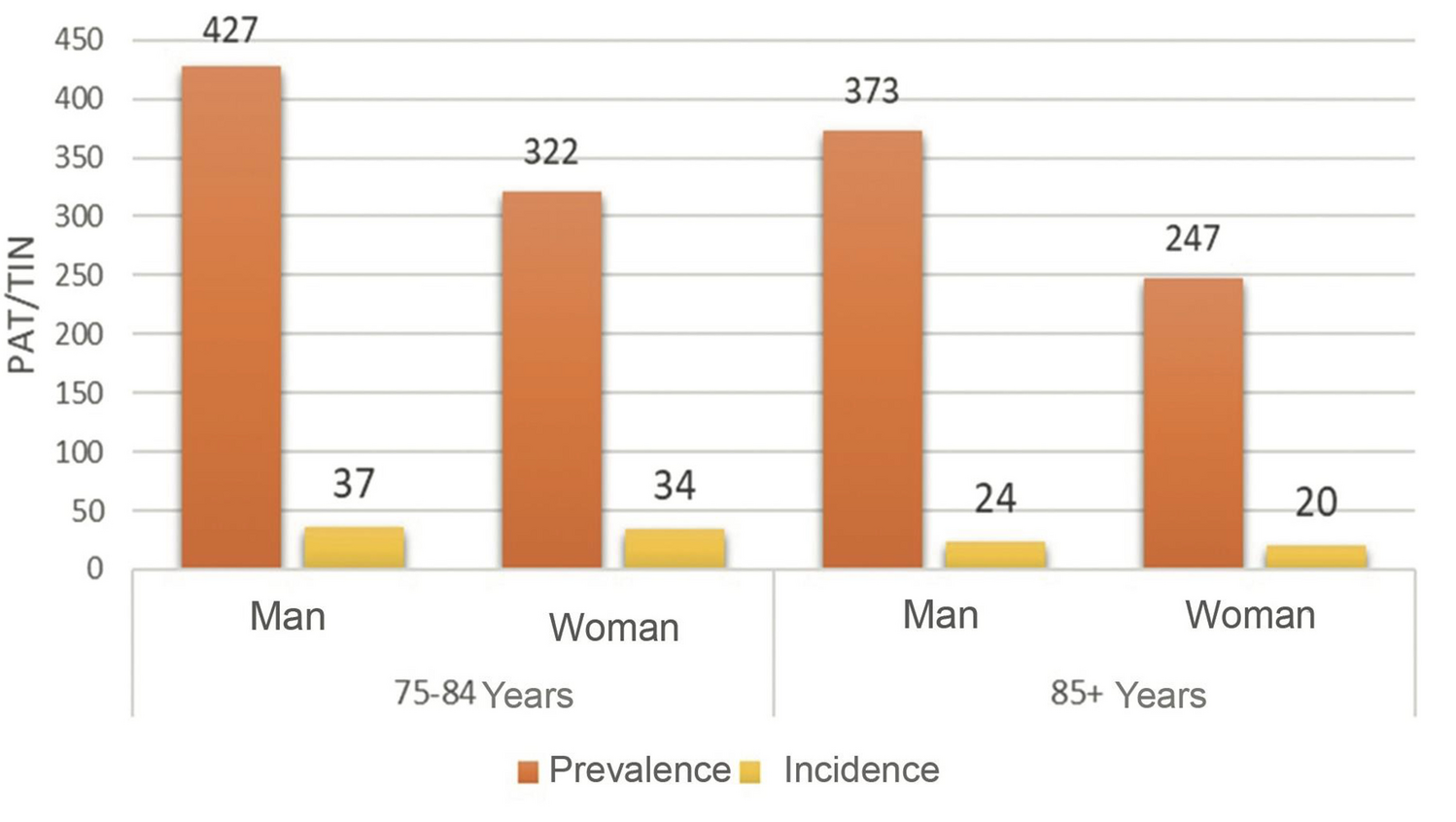
The present results, suggesting that the use of loop diuretics may contribute to the risk of poor outcome in COVID-19, should be considered in light of the fact that these drugs are common in the elderly, who are also the age group most affected by severe COVID-19; and that a considerable proportion of these drugs are prescribed without a proper indication, in elderly patients [19].
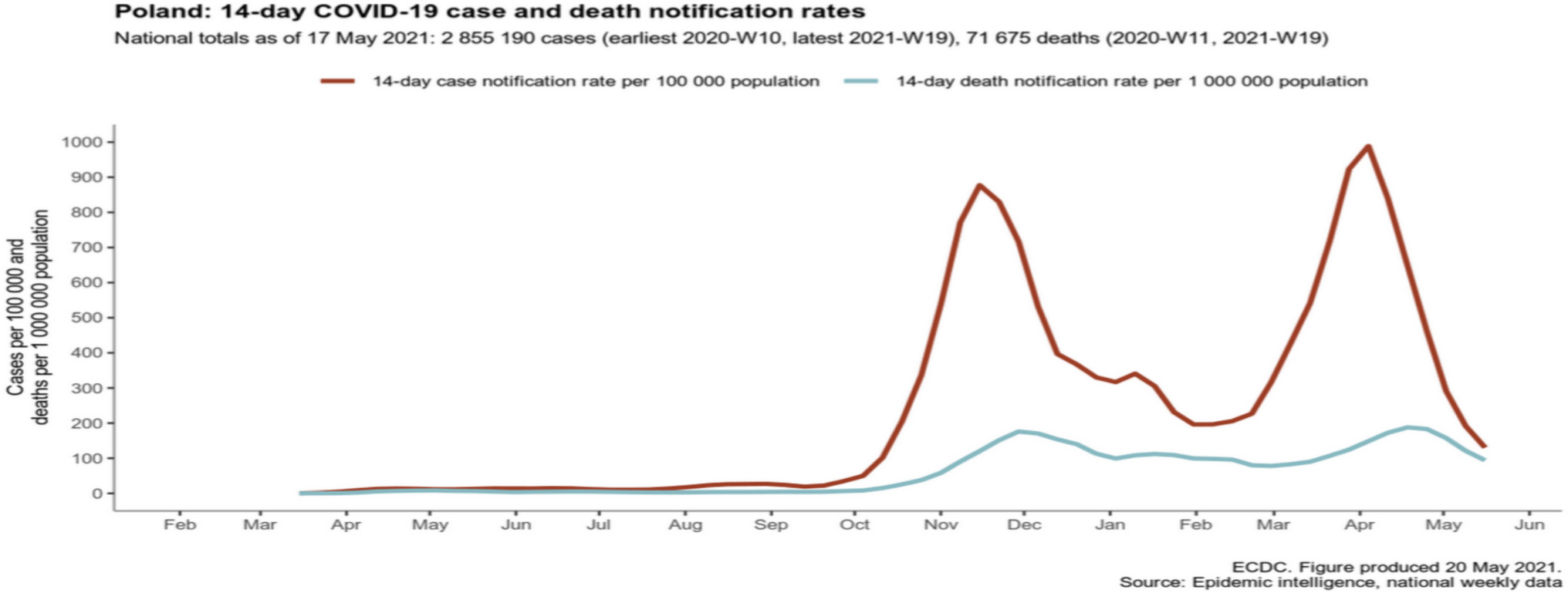
The present study covers the first SARS-CoV-2 infection wave in Sweden, when no vaccine was available and the knowledge about how to treat patients with COVID-19 was limited. Since then, better treatments — such as corticosteroid, anticoagulant and more recently antiviral therapy — are provided and since December 2020 a high proportion of Swedish citizens have been vaccinated. Moreover, numerous new mutations of the virus have emerged. All this may have changed the possible impact of medications on the risk of serious outcomes of COVID-19, something that should be explored in further studies.
Strengths and limitations
The strength of this study lies in the large, nationwide cohort-based data from multiple, record linked national registers. This favours the generalisability of the results. However, there are also some limitations. One is the lack of information on persons with COVID-19 who did not die from the disease. For several reasons, only few of them could have been diagnosed during the study period. First, most likely a considerable number of COVID-19 cases were asymptomatic or showed symptoms or signs that did not lead to suspicion of COVID-19. Second, at this early stage of the pandemic, testing for COVID-19 in the Swedish population was very limited and restricted in essence to severe cases.
Other limitations are related to the register-based design of the study. First, as the study is based on register data, we lack more detailed clinical data on the studied persons, such as physiological and laboratory parameters. Second, the registers used have some shortcomings. The SPDR only records prescription drugs dispensed at pharmacies. Over-the-counter drugs and drugs administered in hospitals or from drug storerooms in nursing homes are not recorded in the register, potentially leading to an underestimation of the actual drug exposure. However, between 80 and 90% of DDDs of drugs dispensed to the Swedish population annually are prescription drugs delivered through pharmacies and are therefore covered by the SPDR. The patient register, providing the data on diagnoses, only covers inpatient and specialised outpatient care but not primary care. Therefore, some of the diagnoses processed as confounders in our analyses, particularly those often treated in primary care, such as diabetes, hypertension, dementia and obesity, may not have been fully covered.


留言 (0)