
記住我





CS is a primary malignant bone tumor with a variable and often unpredictable course that can progress gradually from a slow-growing lesion to an aggressive metastatic sarcoma [3, 5, 25]. Its prognosis depends on anatomical location, lesion size, and histological grade. As it is a hypovascular tissue that secretes a protective chondroid matrix, the response to radiotherapy and chemotherapy is not promising. Based on previous studies [4, 17, 26], we attempted to treat central intramedullary CS with extended curettage assisted by MWA at our Bone Cancer Center. In our retrospective study, no patients developed tumor recurrence, a higher malignancy degree, or distant metastasis during follow-up, which was a surprising result and superior to that of previous studies. The MSTS score of the patients’ postoperative limb function reached 28.8 ± 1.0. Simultaneously, we made some improvements in the preoperative diagnosis of patients, similar to Brown’s [27] study. We diagnose patients in strict accordance with the combination of clinical, imaging and pathological methods, and we fully utilize the power of MDT to ensure that no patient is missed or misdiagnosed. In addition, secondary neurovascular injury or secondary fracture caused by MWA, about which we were concerned, did not occur during the follow-up of this cohort. In this study, the use of extended curettage, assisted by inactivation of intralesional MWA, resulted in satisfactory oncological outcomes, while ensuring functional outcomes for the patients (Fig. 5). We speculate that reasonable preoperative diagnosis of intramedullary CS, correct application of MWA, and fine treatment intraoperatively may have played an important role in our study outcomes.
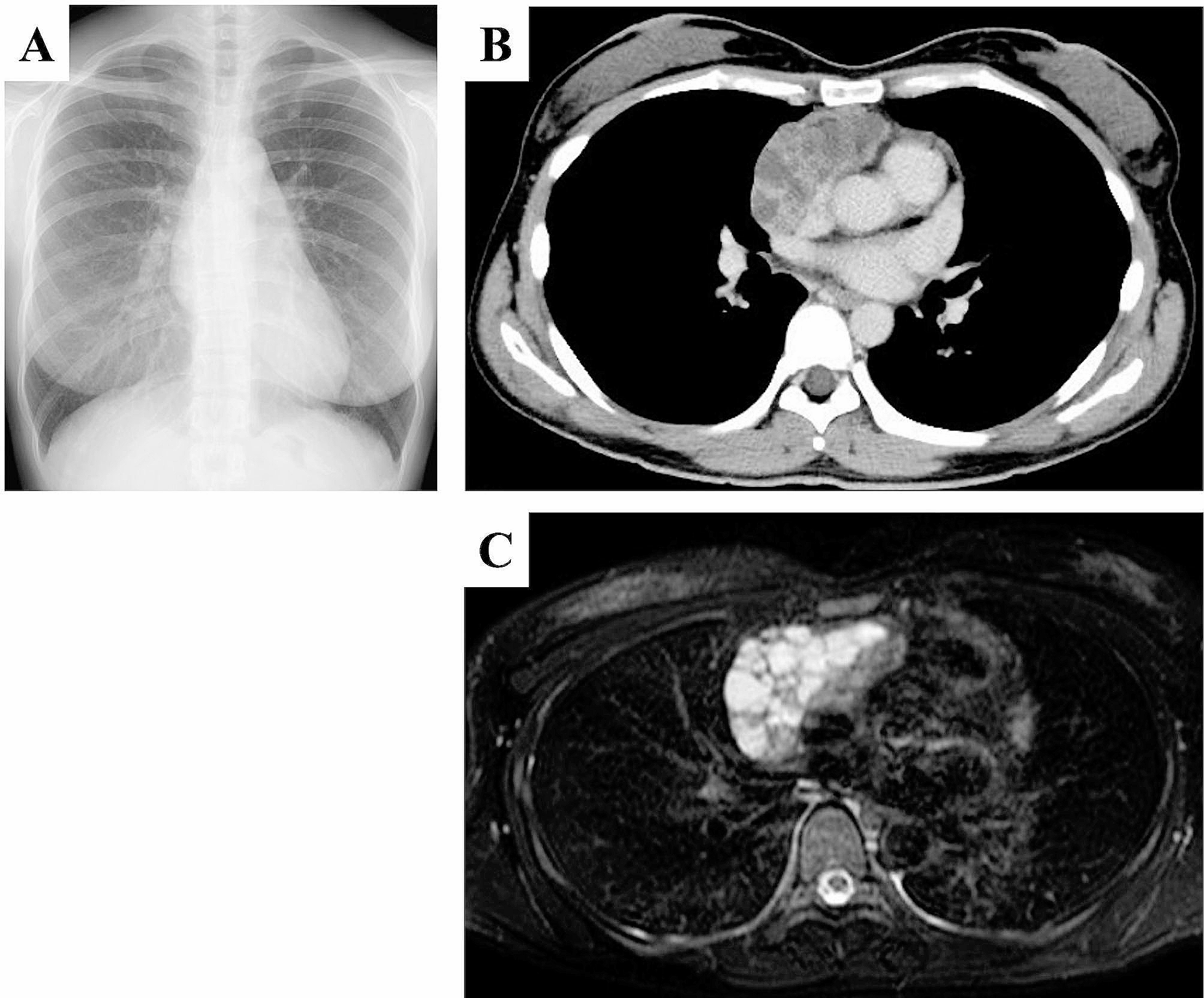
Fig. 5
A typical case of intramedullary chondrosarcoma of proximal humerus. (a) Anteroposterior and lateral X-ray revealed scattered calcification. (b) MRI showed low signal on T1WI and high signal on T2WI, and the lesion involved the internal cortex of medullary cavity. (c) The lesions were inactivated by microwave ablation, followed by extended curettage. (d) Anteroposterior and lateral X-ray after filling tumor cavity with bone cement
Surgical treatment has been the only effective treatment for CS to date [6, 17, 21, 22]. For high-grade CS, extended resection is the preferential treatment [4, 17]. Nevertheless, even when such a radical surgical method is adopted, there is still a high local recurrence rate and distant metastasis rate, and the long-term prognosis of patients is unsatisfactory. Moreover, there has been no consensus regarding the surgical treatment of intramedullary CS. Extended resection for intramedullary CS can achieve excellent oncological prognosis [28, 29], but unavoidably sacrifices some limb functions in the process. With simple intratumoral curettage, although limb function can be preserved, the risk of local recurrence and malignancy upgrading is greatly increased. Therefore, there has been a need to find a way to balance oncological prognosis and functional prognosis in the surgical treatment of intramedullary CS.
The application of expanded curettage and adjuvant treatment (Table 2), such as cryosurgery [22, 29, 30], high-speed grinding and drilling [31], use of bone cement [16, 22], phenol, and absolute ethanol [32, 33], may plausibly balance the oncological and functional prognoses of patients with intramedullary CS. However, with advances in treatment equipment, the application of radiofrequency ablation or MWA in intramedullary CS has also been reported [18, 19, 34]. Although these improvements have greatly improved the prognosis of patients, a small number of patients with recurrence or malignancy upgrades emphasizes the importance of clinical diagnosis and possible need for surgical treatment of intramedullary CS, and highlight the need for further refinement of treatment methods.
Table 2 Summary of extended curettage and adjuvant therapy for intramedullary chondrosarcomaCorrect preoperative diagnosis and grading of intramedullary CS are the basis for selecting the correct surgical method. Inadequate tumor grading may lead to inappropriate surgical treatment, further increasing the risk of local recurrence, metastasis, and subsequent mortality [11, 13, 15, 36]. Overevaluation of tumor grade may lead to the inappropriate use of more invasive surgical treatments, increasing the risk of surgical complications, sacrificing limb function, and resulting in poor cosmetic outcomes. Theoretically, preoperative biopsy is the most important standard for tumor diagnosis and grading [2, 8]. Considering the low pathological discrimination between CS of different grades, it is insufficient to rely solely on pathological diagnosis. Diagnostic biopsies have been shown to be 94% accurate in distinguishing between low-grade and high-grade CS [11]. However, accurate grading of CS lesions by needle biopsy was performed in only 86% of cases. This emphasizes the importance of combining clinical and radiographic diagnoses when devising a surgical treatment plan [7]. Therefore, preoperative radiographic and clinical signs may carry a greater weight in preoperative diagnosis and grading. This is the diagnosis and treatment approach implemented by our institution.
The surgical treatment of intramedullary CS prefers local curettage supplemented by adjuvant treatment, which can achieve satisfactory oncological control [6, 16, 21, 37], rather than aggressive strategies, such as extended resection or radical resection, which can obtain a more satisfactory oncological prognosis, but involves greater sacrifice of limb function. With the innovation of treatment equipment, surgical strategies are constantly improving, and the application of thermal ablation technology in the field of bone tumors and the release of related guideline documents have also led to new treatment strategies for the surgical treatment of bone tumors [38,39,40,41,42]. The application of radiofrequency ablation or MWA in osteoid osteoma and bone metastases has been widely reported [43,44,45], and its therapeutic effect is worthy of recognition. However, the possible consequences of thermal ablation need to be considered, such as secondary fractures, recurrence, and soft tissue necrosis [44, 45]. Therefore, we propose the innovative use of MWA as an adjuvant measure for local curettage of intramedullary CS to achieve an optimal tumor control rate. Our strategy has proven feasible: no tumor recurrence was found during the follow-up of patients in this cohort, and most patients retained satisfactory limb function.
The principle underlying MWA is that the microwave electromagnetic field acts on water molecules, protein molecules, and other polar molecules in tumor tissue, to generate extremely high-speed vibrations, resulting in mutual collision and friction between the molecules, generating a high temperature of up to 150 °C within a short time period, thus leading to cell coagulation necrosis. Owing to high frequency, short wavelength, and shallow penetration depth, medical microwave is generally about 3 cm. CS tissue has a high water content; therefore, the temperature can rapidly rise to achieve the effect of in situ tumor inactivation [38, 46]. As hard tissue, bone is mainly composed of collagen and inorganic calcium salt; thus, it can withstand high temperatures while maintaining its original biomechanical strength [43, 44]. Intramedullary CS is an intramedullary lesion. MWA can ensure the complete inactivation of intramedullary tumors. By strictly controlling the inactivation time and providing extramedullary cooling treatment with cold saline, extraskeletal soft tissues can be properly protected from thermal burns. As hard tissue, the main components (collagen and inorganic salt) of the bone tissue can withstand elevated temperatures, and the maintenance of the biomechanical strength is enhanced. In situ MWA can preserve the natural continuity of bone tissue to the maximum extent, which is conducive to long-term reconstruction and remodeling of bone tissue and avoids osteotomy and bone healing problems that need to be considered in cases of extended resection of tumors and inactivated replantation. Microwave ablation has many advantages over other ablation techniques, particularly radiofrequency ablation, such as higher intratumoral temperature, larger tumor ablation volume, faster ablation time, local hemostasis, the possibility to apply multiple ablation needles simultaneously, and less surgical pain. MWA is similarly beneficial for other benign or invasive intramedullary tumors.
MWA can effectively inactivate tumors, but it is also necessary to remove coagulative necrotic material. Subsequent local extended curettage, followed by bone grafting or bone cement filling in the tumor cavity, can completely restore the structural integrity of the bone and preserve the function of adjacent joints. Prophylactic internal fixation is recommended for patients with lesions located in the lower limb bone or those with cortical fenestration greater than 4 cm in the upper limb bone, regardless of the filling method used (Fig. 5).
Innovation in adjuvant therapy has yielded satisfactory results, which exceeded expectations. We found that preoperative diagnosis based on radiographic and clinical manifestations may be more suitable for patients with CS than relying solely on biopsy pathology. Rational operation of MWA is the most important step in achieving tumor inactivation and avoiding soft tissue burns. Proper protection of soft tissue and strict control of single-hole ablation time are particularly important. Restoration of bone structural integrity is also an important prerequisite for ensuring postoperative limb function.
This study had some limitations. Due to the rarity of CS, the small sample size of this study and the relatively short follow-up time make it impossible to draw definitive conclusions about oncological prognosis. Considering the slow biological progress of CS, long-term follow-up with large samples and controlled studies based on different adjuvant treatments are necessary.
In conclusion, we demonstrated that extended curettage assisted by MWA can achieve an excellent oncological prognosis for intramedullary CS while ensuring normal postoperative limb function. Standardized operation of MWA and accurate preoperative diagnosis, guided by radiographic and clinical manifestations, are important factors for achieving successful degradation treatment of intramedullary CS.
留言 (0)