The prognosis varies significantly among different phases of TNM. A number of studies have confirmed that the 3-year survival rate of stage I lung cancer can reach more than 90%, while the 3-year survival rate of stage II lung cancer can reach about 70%. The survival rate for stage III lung cancer patients is usually less than 50%. In addition, disease recurrence and metastasis occurred mainly within the first two years after surgical intervention. This has led to a significant decline in survival for stage III patients [13,14,15]. Therefore, patients should be closely followed up after surgery, with timely detection of tumor recurrence and metastasis and timely diagnosis and treatment intervention to improve their survival prognosis and quality of life.
The relationship between tumor location and prognosis was related to the distribution of lymph node metastasis. Yang et al. analyzed the association between mediastinal lymph node metastasis distribution and survival in patients with operable NSCLC (≤ 3 cm). The results were as follows: upper right lobe, 4R station (17.7%); right middle lobe, 7th station lymph node (14.9%); right inferior lobe, 7th station lymph node (19.8%); left upper lobe, 7th station lymph node (16.6%); left upper lobe, 5th station lymph node (18.2%) [16]. The Guo et al.‘s study explored the association between the primary site and the mediastinal lymph node station in patients undergoing radical resection of N2 lymph node metastases and showed that the highest rate (100%) was found in lymph node station 2/4, occurring in the right upper lobe. The proportion of lymph nodes at the 7th station in the right middle lobe and lower lobe was higher, accounting for 80% and 88.9%, respectively. The left upper lobe mainly occurred in the 5th station lymph node (84.4%) [17]. Lin et al. evaluated the prognosis of the inferior lobe (basal and superior segments) in patients with operable lung adenocarcinoma. The results showed that N2 lymph node metastasis was more likely to occur in the basal segment than in the upper segment of lung adenocarcinoma excised in the lower lobe [18]. In Liu et al.‘s study, inferior lobe origin was strongly associated with lower overall survival compared to non-right inferior lobe tumors [19].
Since Virchow proposed the hypothesis that cancer occurs at the site of chronic inflammation, extensive research has been conducted on the correlation between inflammation and cancer. The tumor microenvironment plays a crucial role in the occurrence and development of tumors by promoting cell proliferation and migration under the regulation of inflammatory cells [20]. Prior retrospective research has demonstrated a strong correlation between NLR and survival rates in patients with operable NSCLC [8, 21]. The meta-analysis verified that an elevated NLR is an indicator of unfavorable outcomes in patients with lung cancer [5, 22]. The possibility that NLR can effectively assess survival in patients with NSCLC is explained by the fact that neutrophils play an important role in all aspects of cancer progression, including tumor initiation, growth, proliferation, and progression. Neutrophils are involved in tumor-related properties by promoting angiogenesis, motility, migration, and invasion, as well as regulating other immune cells [23]. In addition, some neutrophils have the ability to induce epithelial mesenchymal transformation through the TGF-β/Smad signaling pathway, which is also considered to be a key factor in tumor occurrence and development [24]. This relationship places neutrophils in a central role in tumor inflammation, playing an important role in tumor growth and progression through their direct effects on tumor cells or through their indirect effects on the tumor microenvironment. Studies have shown that high levels of neutrophils are linked to decreased survival in NSCLC [25, 26]. Lymphocytes can hinder tumor cell growth and movement by releasing cytokines, which significantly contribute to tumor defense and immunological monitoring [27]. According to research, a decrease in the percentage of lymphocytes in peripheral blood may result in an elevation in the NLR, which is strongly associated with disease progression [28].
Due to the characteristics of rapid metabolism and proliferation of tumor cells, nutritional status indicators such as BMI and albumin are also important clinical prognostic parameters for evaluating lung cancer treatment. Malnutrition has been observed in previous studies to be associated with poorer overall survival, time to tumor progression, and quality of life in lung cancer patients [29,30,31,32,33]. It is important to note that anti-cancer treatments, including surgery, may exacerbate the severity of malnutrition. In addition, malnutrition is associated with increased susceptibility to perioperative morbidity and death. Incorporating nutritional assessment into pre-treatment regimens for cancer patients is critical, as research has shown that providing nutritional support can effectively mitigate the adverse effects of malnutrition on perioperative outcomes [34, 35].
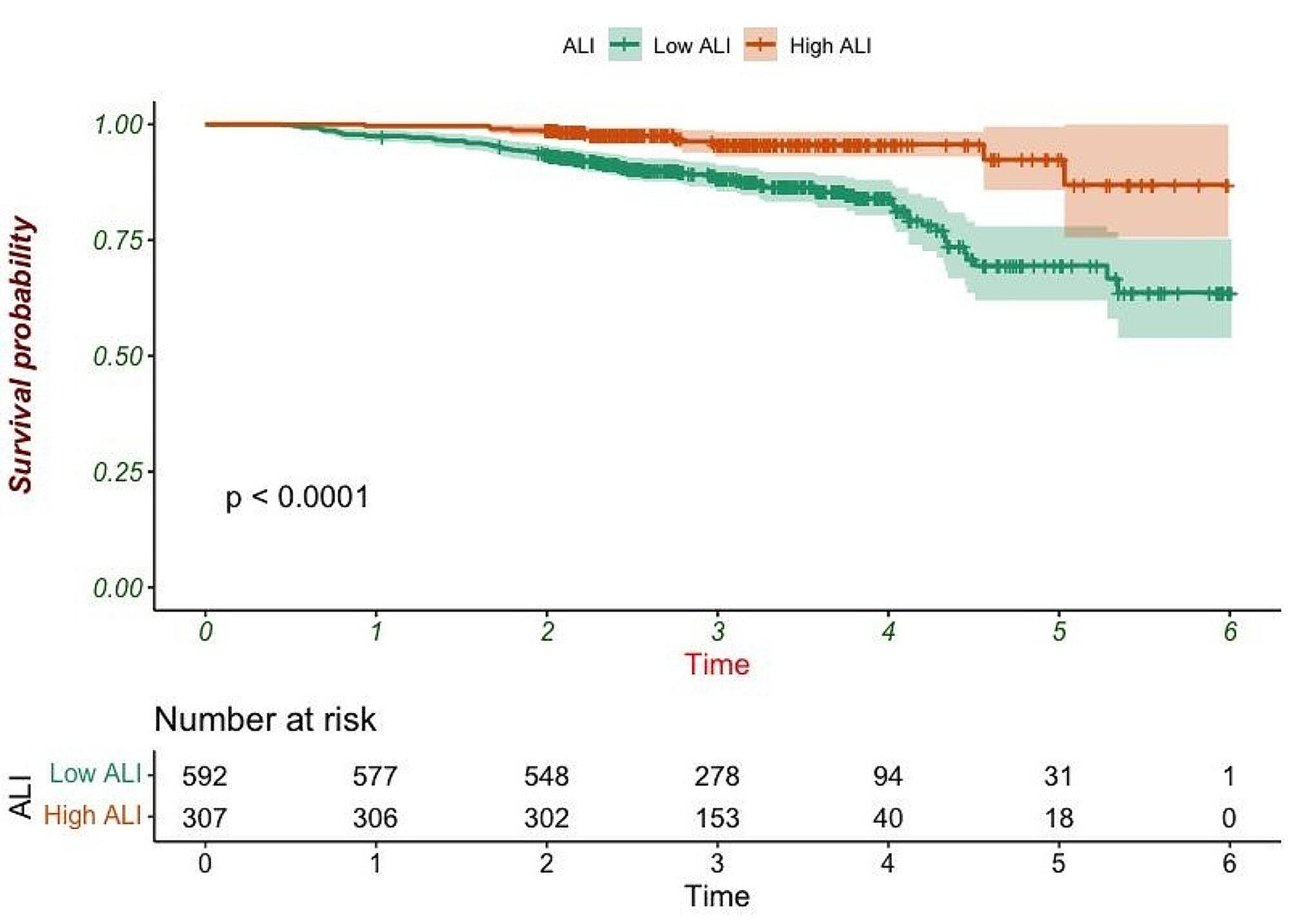
Compared with NLR, PLR, and other single indicators, ALI is a complex indicator composed of inflammation and nutrition indicators, which can more comprehensively assess the level of inflammation, immune function, and nutritional status of patients. This approach has been shown to be beneficial for a more effective assessment of patient outcomes. Song et al. [36] and colleagues assessed the prognosis value of 16 inflammatory and nutritional markers for OS in patients with lung cancer. They discovered that the prognostic ability of ALI was superior to other inflammation and nutrition indicators. Mandaliya et al. [37] assessed the prognostic significance of NLR, ALI, PLR, and lymphocyte-to-monocyte ratio (LMR) in predicting OS in patients with advanced NSCLC. The study revealed a strong correlation between NLR and ALI with OS. Mountzios et al. [38] also verified that ALI serves as a robust indicator for forecasting survival outcomes in patients with advanced NSCLC who are undergoing treatment with immune checkpoint drugs. Additionally, this study demonstrates that ALI possesses a robust capacity to forecast outcomes in patients with NSCLC who are undergoing surgical procedures. Therefore, Assessment of ALI levels before treatment, stratification of patients who may have low levels of ALI, and adjustment of individualized treatment regimens (for example, low BMI and ALB indicate poor nutrition and can be given appropriate nutritional support) can help to prolong patient survival and improve quality of life. Second, ALI offers several advantages, including simple measurement, routine availability, and a high degree of standardization. Therefore, we suggest that ALI may serve as a reliable and cost-effective prognostic indicator of postoperative survival in patients with NSCLC.
Lymphatic vascular invasion (LVI) has long been associated with poorer survival and highly aggressive tumors [39]. In the study of Dicken BJ et al., LVI is considered to be an effective factor that can independently predict survival and is correlated with T stage [40]. LVI has been observed as a significant predictor of OS in retrospective studies of gastric cancer and NSCLC [41,42,43]. However, no correlation was found between LVI and OS in this study, which may be because LVI mostly appeared in middle- and advanced-stage patients, while this study mainly focused on patients with stages T1–T2, and the risk of LVI was relatively low. In addition, perineural invasion (PNI) is also a strong predictor of postoperative NSCLC. In the study of Demir A et al., PNI was observed to be a decisive factor for poor prognosis. According to their report, the presence of PNI was found to have a significant negative impact on 3-year and 5-year survival (3-year survival decreased from 54 to 32% and 5-year survival decreased from 15–0%) [44]. Kilicgun A et al.‘s report observed that patients with stage IA with perineural infiltration had a worse survival rate than patients without PNI but with stage IIIA disease [45]. Another retrospective study also confirmed that the appearance of PNI significantly shortened the patient’s prognosis. The 3-year survival rates of stage I NSCLC patients with and without PNI were 23.3% and 63.2%, respectively [46]. Our results showed that the occurrence of PNI could increase the risk of death by 2.24 times, and PNI still had good predictive value after excluding multiple confounding factors.
The traditional TNM staging system ignores the biological differences between tumors and normal tissues. Compared with the TNM stage prognostic evaluation system, the nomogram can synthesize various prognostic indexes and has a better prognostic evaluation value [47]. Each independent variable receives a score based on the specific patient situation, and the nomogram’s high accuracy and practicability allow for the calculation of the probability of patients’ occurrence of outcome events based on the relationship between the total score and the probability of outcome occurrence. Secondly, compared with simple models and scoring systems that contain only a few variables, the nomogram model can more comprehensively analyze the risk factors and interaction effects related to survival prognosis, which is of great significance to provide guidance for the clinical management of patients. Based on the above factors, the nomogram has an important clinical reference value in predicting the prognosis of NSCLC patients.
In this study, the prognosis of patients with operable NSCLC was evaluated by constructing a nomogram model. The model was evaluated by the C-index and correction curve, and the results showed that the model had high prediction accuracy and clinical practicability and could provide an important clinical reference value for the prognosis assessment of NSCLC. However, there are still some limitations: First of all, this is a retrospective analysis with a single-center design and limited sample size, which inevitably leads to selection bias in the selection of study subjects and clinical data collection. Secondly, there is no clear consensus on the optimal cut-off value of ALI. The effect of dynamic changes in ALI values on the long-term prognosis remains to be evaluated. Moreover, any underlying factors that affect changes in blood indicators (such as previous nutritional support in other hospitals) can lead to fluctuations in ALI results. Third, this study lacks external data to verify the model. The essence of the above reasons lies in the fact that in the retrospective study, the pre-treatment status of patients (including whether they had received nutritional support in other hospitals and whether there were infection factors that had been treated in other hospitals before treatment) can only be judged by the hospitalization log recorded in the electronic case system, which inevitably causes selection bias. Therefore, prospective studies need to strictly include and exclude patients to avoid deviations from ALI results. Secondly, studies conducted by individual institutions are more limited, and the results may only be representative of the region, with regional differences (such as the relatively poor nutritional status of patients in some economically disadvantaged areas). Therefore, we need multi-center studies to control the limitation of regional populations. Based on the above reasons, it is necessary to conduct multi-center and prospective studies in the future to improve the model so that the built columns can predict the prognosis of patients more accurately and gain benefits for both doctors and patients.






留言 (0)