
記住我
Out of the 81 adolescents who participated in the Phase-I qualitative study, the majority were between the ages of 12 and 15 (58%), currently in grades 6 to 8 (38.3%), and belonged to the Brahmin/Chhetri (45.7%) or Janajati (34.6%) caste/ethnic groups.
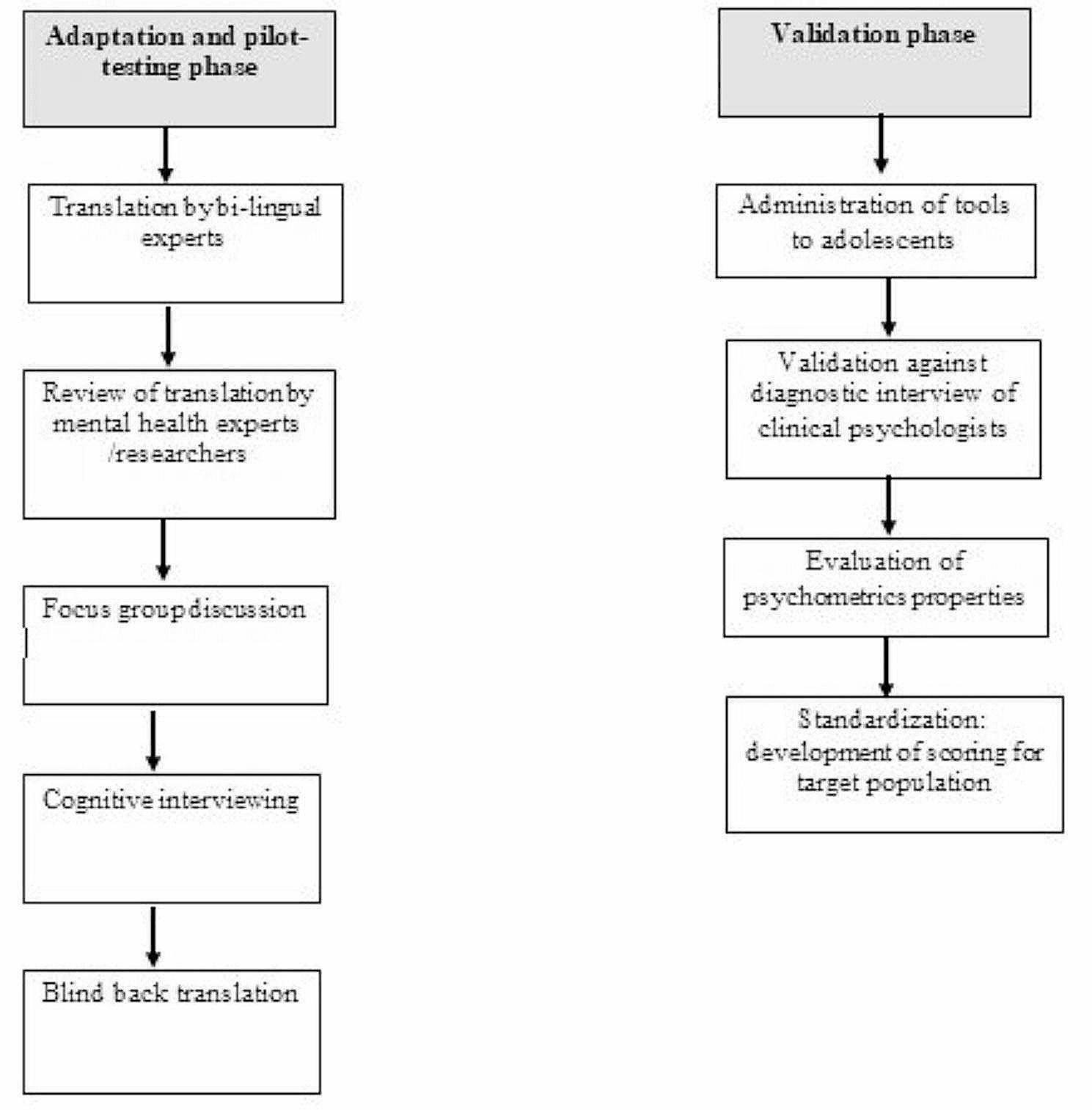
Translation and cultural adaptation of PHQ-A and GAD-7The translation and cultural adaptation of the PHQ-A and GAD-7 were conducted following UNICEF’s MMAPP protocol (Carvajal-Velez et al. [4]). The PHQ-A was translated by two mental health experts, including a clinical psychologist and a psychiatrist with a research background, who were experienced in translating mental health tools. The GAD-7 was translated by three mental health experts, including two clinical psychologists and one psychiatrist. The translators followed the guidelines recommended for cross-cultural research (van Ommeren et al. [38]).
First, a particular item of the PHQ-A and GAD-7 was translated from English to Nepali, back translated into English, and evaluated based on comprehensibility, acceptability, relevance, and completeness (Kohrt et al. [18]). Second, the translations were reviewed by two mental health researchers and one psychiatrist, who made several adaptations to ensure the translations were acceptable and easily understandable by different groups of adolescents. Third, feedback and inputs from adolescents were obtained through focus group discussions (FGDs) and cognitive interviews (CIs). In the FGDs, participants were asked if the translations were understandable, acceptable, and relevant to adolescents from different caste/ethnic groups, ages, and education levels. If a word or terminology was not acceptable or understandable, participants were asked to provide an alternative translation or terminology. Fourth, after incorporating feedback and suggestions from the FGDs, cognitive interviews were conducted individually with adolescents who were not involved in the FGDs. The results from the FGDs and CIs are summarized separately for the PHQ-A and GAD-7 in Tables 1 and 2, respectively.
Table 1 PHQ-A original item, back-translation of Nepali items, and comments from adolescentsTable 2 GAD-7 original item, back-translation of Nepali items, and comments from adolescentsThe major adaptation made in both PHQ-A and GAD-7 included changing statements into questions, using a visual scale (glass scale) to maintain uniformity in responses and keeping a time frame (i.e. in the past two weeks) in the beginning of each item. We included a water glass response pictorial scale to maintain uniformity in assessing the severity of each symptom. This scale was developed through a transcultural translation process with children in Nepal (Kohrt et al. [18]). Adolescents in the adaptation phase found that using the water glass response scale helped them differentiate between different response options.
Other adaptations suggested by the adolescents included providing examples to clarify specific questions, dividing certain items into multiple questions, and ensuring that items are relevant to the local context by explaining the meaning of specific terminology or idioms. For example, adolescents mentioned that “watching TV” is one of their most enjoyable activities, so it was recommended to remove “watching TV” from PHQ-A item-7.
Sometimes it is hard to concentrate due to tension or sadness. However, adolescents are able to maintain their concentration on TV at any time, even when they are feeling tense, because watching TV is an interesting activity for them.Cognitive interview-8.
Moreover, during the FGDs and CIs, most of the adolescents recommended splitting PHQ-A items 3, 5, 6, and 8 into multiple questions. They observed that these items encompassed multiple themes or ideas within a single question. For instance, during a cognitive interview, one adolescent mentioned experiencing sleep problems for several days. However, he pointed out that he couldn’t provide the same response to all three issues, such as having difficulty falling asleep, waking up during sleep, or feeling sleepier than before.
Similarly, during the FGDs and CIs, many adolescents suggested breaking down PHQ-A items 3, 5, 6, and 8 into multiple questions. They noticed that these items covered multiple themes or ideas within a single question. For example, during a cognitive interview, one adolescent mentioned having sleep problems for several days. However, he noted that he couldn’t give the same response to all three issues, such as difficulty falling asleep, waking up during sleep, or feeling sleepier than before.
This question (PHQ-9 item3) contains three ideas/concepts, therefore, it makes hard to understand once at a time. Therefore, I suggest asking the first two ideas in a separate question, and last idea in another question–Cognitive interview-9.
Participants reported that there is no idiom or appropriate terminology for “feeling on edge” (GAD-7 item-1) in Nepali. Therefore, they suggested excluding this term from the Nepali translation. Additionally, an example of “writing, playing games, hanging out, using mobile” has been suggested to added clarifying the term “things” for GAD-7 item-3. Most participants associated “trouble relaxing” (GAD-7 item-4) with physical aspects, so this has been further clarified by adding “because of (feeling) fidgety in your mind”. Furthermore, the term “easily annoyed or irritable” in GAD-7 item-6 has been changed to “annoyed or irritable in small things”. An example has also been added in GAD-7 item-7 to clarify the term “awful” (Table 2).
Phase-2 validation study resultsTable 3 displays the socio-demographic characteristics of the participants in the validation study (Phase II). The majority of the participants were girls (55%). Their ages ranged from 12 to 19 years, with most falling between 15 and 19 years old (62%). The most common castes were Brahmin/Chhetri (53.1%) or Janajati (36.1%), and the majority practiced Hinduism (79.7%) and spoke Nepali at home (81.4%).
Table 3 Social demographic characteristics of the participants involved in the validation studyPsychometric properties for PHQ-AWe presented the area under the curves (AUCs) for both PHQ-A and GAD-7 separately for girls, boys, younger, and older adolescents. The AUC of PHQ-A for boys was 0.81 (95% CI, 0.68–0.93), while it was 0.88 (95% CI, 0.82–0.93) for girls. Similarly, the AUC for younger adolescents was 0.92 (95% CI, 0.85–0.98), while it was 0.85 (95% CI, 0.79–0.92) for older adolescents.
Table 4 presents the psychometric properties of the adapted PHQ-A compared with the K-SADS depression module. A cut-off score for the overall sample of > = 11, yields sensitivity of 0.90 and specificity of 0.71. The positive predictive value for the cut-off score of > = 11 was 0.31 and 0.98. The results suggested different cut-off scores for younger and older adolescents. A cutoff score for younger adolescents (12 to 14 years) is > = 13, with a sensitivity of 0.93 and specificity of 0.80. The PPV and NPV for > = 13 for younger adolescents were 0.33 and 0.99. On the other hand, a cut-off score for older adolescents was > = 11, with a sensitivity of 0.89 and specificity of 0.70, and PPV of 0.32 and NPV of 0.97 (Table 2). Similarly, the results also suggested different cut-off scores for boys and girls. A cut-off score of > = 11 with a sensitivity of 0.73 and specificity of 0.78 has been suggested for boys. The PPV and NPV for the > = 11 cut-off for boys were 0.17 and 0.97. Similarly, a cut-off score for girls of > = 13 has a sensitivity of 0.85 and specificity of 0.73. The cut-off score of > = 13 has a PPV of 0.40 and NPV of 0.96 (supplementary table-1).
Table 4 Validation psychometrics of the PHQ-A comparison with the K-SADSPsychometric properties for GAD-7The AUC of GAD-7 was 0.80 (95% CI, 0.73–0.87) for younger adolescents and 0.76 (95% CI, 0.70–0.82) for older adolescents. For boys, the AUC was 0.77 (95% CI, 0.69–0.85) and slightly lower for girls at 0.74 (95% CI, 0.68–0.81).
Table 5 presents the psychometric properties of GAD-7 for the overall sample, boys, girls, and younger and older adolescents separately. A cut-off score for the overall sample of > = 7 yields a sensitivity of 0.83 and specificity of 0.61. The PPV and NPV for the cut-off score of > = 7 were 0.41 and 0.92. Acut-off score for both younger and older adolescents was 8, with the same sensitivity (0.70 for both groups) but slightly different specificities (0.67 for younger and 0.71 for older adolescents), PPVs (0.39 for younger and 0.50 for older adolescents), and NPVs (0.89 for younger and 0.85 for older adolescents). The results suggested different cut-off scores for boys and girls. A cut-off score of > = 7 with a sensitivity of 0.75 and specificity of 0.71 has been suggested for boys. The PPV and NPV for the > = 7 cut-off for boys were 0.31 and 0.94. Similarly, a cut-off score for girls of > = 8 yields a sensitivity of 0.76 and specificity of 0.61. The cut-off score of > = 8 has a PPV of 0.51 and NPV of 0.83 (supplementary table-1).
Table 5 Validation psychometrics of the GAD-7 from comparison with the K-SADSAdjustments for population prevalenceFigure 2 shows the adjusted prevalence rates for adolescent depression and anxiety at the population level. These rates were calculated using the psychometric properties obtained in this study. We adjusted the false positive (FP) and false negative (FN) rates in the current sample to calculate the true prevalence in the population. For instance, if a prevalence rate of 40% is found for depression on the PHQ-A, the estimated true prevalence rate in younger populations is closer to 25% and for older adolescents it would be below 20%.
Fig. 2
Application of the validation results: adjustments for population level prevalence
Item level analysisThe internal consistency reliability of the PHQ-A (Cronbach’s alpha) was 0.914. Table 6 shows the mean scores of each PHQ-A item for adolescents diagnosed with depression and those without a diagnosis. The results indicate that the PHQ-A items have excellent discriminant ability between depressed and non-depressed adolescents. The mean scores of all PHQ-A items were significantly higher (P < .001) among adolescents with depression compared to those without a diagnosis. Similarly, the mean scores of all PHQ-A items were significantly higher among younger and older adolescents with depression compared to their counterparts without a diagnosis.
Table 6 Discriminant ability of PHQ-A items for adolescents with and without diagnosis on K-SADSSupplemental Table 4 showed that there was no significant difference in the mean score of PHQ-9 item-9 (thoughts of being better off dead/hurting yourself) between boys with and without depression. However, the mean scores of all PHQ-9 items were significantly higher among girls with anxiety (supplemental Table 4).
The internal consistency reliability for GAD-7 (Cronbach’s alpha) was 0.907. Table 7 shows that the mean scores of all GAD-7 items were significantly higher among adolescents diagnosed with generalized anxiety disorder than those without any diagnosis. Similarly, the mean scores of all GAD-7 items were also significantly higher among younger and older adolescents with GAD compared to their counterparts without any diagnosis (Table 7).
Table 7 Discriminant ability of GAD-7 items for adolescents with and without diagnosis on the K-SADSSupplemental Table 5 shows that there was no significant difference in the mean score of GAD-7 item 7 (feeling afraid as if something awful might happen) between boys with and without depression. However, the mean scores of all GAD-7 items were significantly higher among girls with anxiety (Supplemental Table 5).
留言 (0)