
記住我

The study was approved by the Institutional Review Board of the Sheba Medical Center- Tel Hashomer (0947-23-SMC) Israel, and conducted according to the Declaration of Helsinki.
First, an interdisciplinary senior staff focus group, comprised of adult and pediatric physicians, psychiatrists, psychologists, social workers, nurses and Public Relations personnel was organized. Selection of focus group members was based on level of clinical experience and diversity, with the intention of incorporating varied areas of clinical expertise and considerable experience with child and adult trauma. The focus group met once or twice weekly to define and facilitate the implementation of protocol guidelines. Discussions were structured around a set of carefully predetermined questions and were moderated by the Director of the Children’s Hospital (I.M.P.).
Second, a rapid review of the literature was conducted in order to assess existing literature on hostage and captivity situations, specifically those involving young children and child-caregiver dyads. The search included electronic databases, such as MEDLINE, EMBASE, and Cochrane Central Register of Controlled Trials. Studies were included if they were published between 1970 and October 2023 and written in English. Quantitative, qualitative, case reports, reviews and mixed-method studies were included to consider different aspects of captivity within the civilian population. Literature review keywords included: abduct*, captivity*, hostage*, kidnap*, child kidnap*, parent abduction*. Next, the search strategy was expanded to include the keywords: “terrorism”, “war”, “terror*”, “terrorist attack”, as well as “armed conflict”, “acute trauma response*” and “post traumatic response. However, due to the unique circumstances surrounding the situation under study, as well as the relatively short timeframe in which the review was conducted, we opted for a non-systematic approach to gather and analyze the available information. This decision was made to ensure timely access to relevant data and insights in a rapidly evolving context. In addition, local expert guidelines (such as the national council for the child, the Ministry of Health, Israel Defense Force: IDF) informed our approach. Further information was also gathered through personal communication with international experts in the field of hostage situations, child and adult trauma and disaster response.
Based on these cumulative findings, the focus group arrived at a consensus document which details key principles and practical guidelines for the initial reception and care of hostages, (from here on referred to as “returnees”), across the age range. Considerable attention was given to the unique needs of pediatric hostages, parent-child dyads, and families. In addition, guidelines encouraged careful consideration of individual characteristics and circumstances of hostages (i.e., preexisting psychosocial risk and protective factors), as well as the variance in the traumatic exposure during the terror-attack and while in captivity (highlights from the document are provided in Table 1). Guidelines were reviewed and reaffirmed by the Israeli Child National Council. Leaders of clinical sectors reviewed these guidelines with all staff members, and strategies, specific to each sector, were further developed.
Table 1 ReSPOND guidelines for the medical center clinical staff provided by the focus groupThese guidelines were further developed into the elaborated ReSPOND protocol as outlined below:
ReadinessA specialized, trauma-focused training was developed for the multidisciplinary team, comprised of (a) lectures on acute stress and posttraumatic stress reactions across the lifespan, emphasizing diverse and compounded traumatic exposures (e.g., physical and sexual assault, parent-child separation, food and stimuli deprivation, traumatic grief and death notification); (b) live simulation-based trainings and video-based debriefing sessions conducted with professional actors and members of the medical and psychosocial teams at MSR. Studies suggest that active engagement in the learning process within a meaningful or relevant context is crucial for fostering adaptive work-related expertise, a goal that can be achieved through live video simulations [32]. In the current hostage situation, training simulation scenarios were developed by senior trauma experts who composed scripts anticipating returnee’s physiological, psychiatric, and emotional conditions, as well as scenarios expected to unfold throughout their hospital stay. Scripts were created for both adult and adolescent returnees, as well as for mother-infant dyads, highlighting the common and divergent factors in caring for returnees across the age range. Scripts incorporated pre-defined tasks, including pre-reunification family support, returnee admission and escort to unit, family reunification, death notification, developmentally-informed interventions, medical exams, and hospital discharge procedures.
Simulation scenarios were developed to raise awareness and develop strategies for effective coping with potential challenges, inform specific language, and holistic, developmentally-informed methods of care. Special attention was given to the unique needs and care of pediatric returnees (e.g., the importance of a familiar and self-regulated caregiver present at all times and strategies for facilitating positive parental involvement), as well as the importance of constantly monitoring and supporting returnee family members. Live simulation sessions were followed by video-based debriefing, focus-group discussions and group supervision by the senior expert team, refining system-level coordination and elucidating key guidelines for privacy protection, media management, chain of command, decision-making, and task prioritization. Identification of various dilemmas presented by professional actors (such as separation anxiety, refusal of medical exam, dissociation and disorientation during simulations) led to protocol refinement and promoted teamwork and skill mastery.
The extreme hostage situation, intertwined with the tragic events of October 7th and its aftermath, clearly challenged healthcare teams as well. The extreme situation necessitated interdisciplinary providers to deliver acute care that addressed multiple trauma layers within an ongoing national security threat. A shared traumatic reality has been identified in previous research as a significant risk factor for healthcare providers’ personal and professional well-being [33]. Thus, the preparedness of professional teams for such an extreme traumatic event highlighted the need for incorporating trauma-informed principles to prevent secondary traumatic stress. This included shared sessions with senior trauma psychiatrists, relaxation techniques, enabling open communication and sharing of distressing emotions, and a designated space with refreshments for rest and team bonding.
Specialized teamsPast hospital responses to mass casualty incidences highlight the importance of prioritizing the organization of human response over physical supplies [34]. Accordingly, considerable efforts were devoted to the formation of well-rounded specialized teams. The teams dedicated to receiving and caring for the returnees consisted of experienced adult- and child-focused multidisciplinary professionals, from the following sectors: medicine, social work, psychology, forensics, gynecology and nursing. As a general standard and principle, the Sheba Medical Center ensures all aspects of diversity are represented as best possible.
Psychologists and social workers functioned at the core, with the former assigned to each released individual or child-parent dyad, and the latter assigned to accompany returnee’s families who awaited the release of their loved ones within the designated hospital facility. Each pair was reinforced by a team supervisor, a senior psychiatrist, psychologist, or social worker, present on site and available for consultations as needed. In addition, forensic specialists were available on site and called upon when a forensic exam was indicated. Nurses and supportive staff were positioned throughout the facility. Director and Deputy Director of the Safra Children’s Hospital oversaw the entire operation and were present at the facility from reception to discharge.
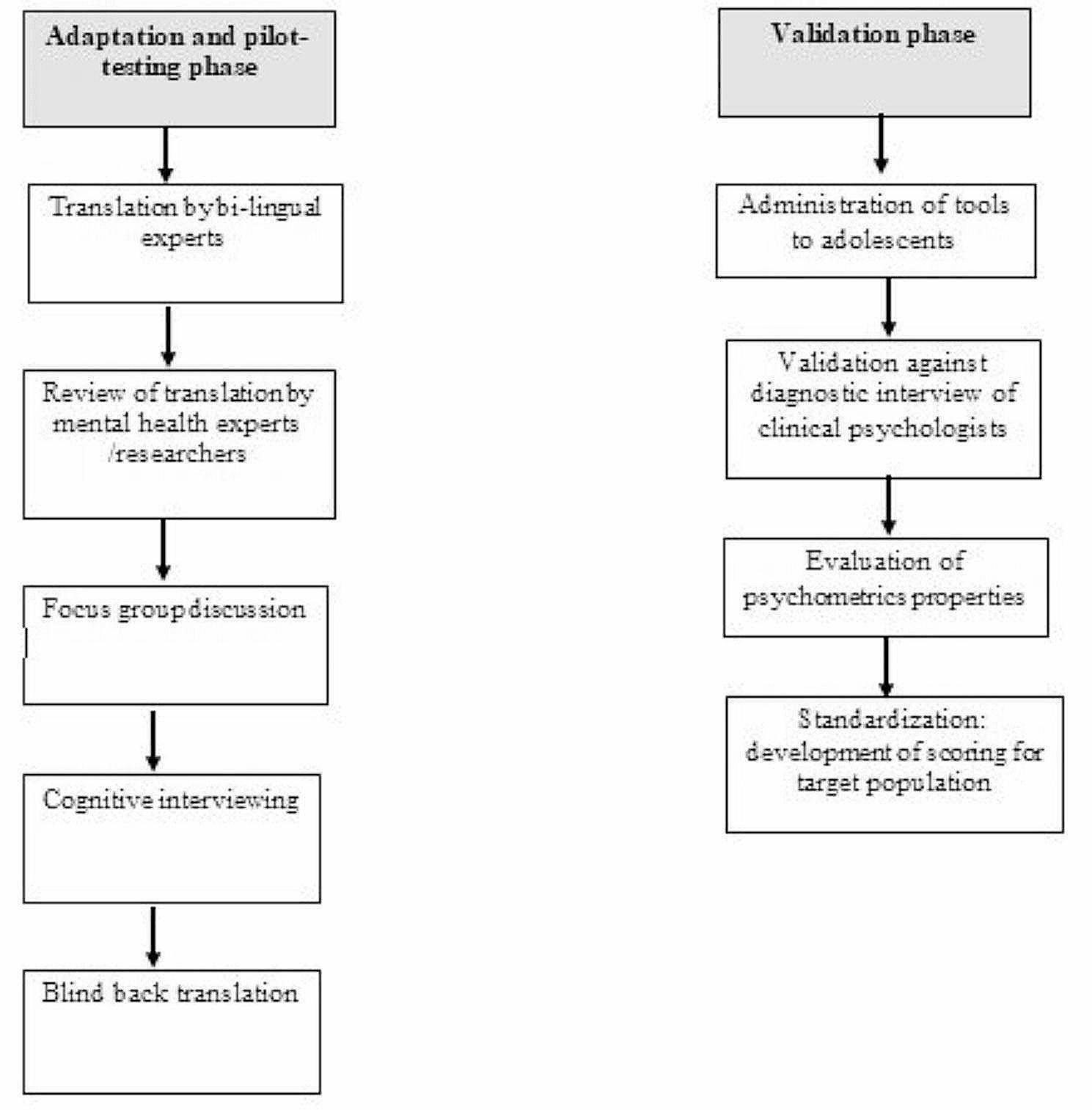
A primary task of the professional teams was optimizing and streamlining the transition process from the Gaza border and throughout returnees’ stay (see Fig. 1).
Fig. 1
Protocol for multi-disciplinary reception and care procedures of hostages admitted to the Safra Children’s Hospital. Dashed lines indicate returnees’ release process outside hospital ward; Straight lines represent hospital arrangements for the reception of returnees; Grey rectangles signify the process within the hospital facility following returnees’ admission. *IDF-Israeli Defense Forces
Upon receiving military notification with names of hostages expected to be released, on-call unit leaders would be contacted and a multidisciplinary team, encompassing psychosocial preparation, properties, logistics, patient experience (e.g., basic necessities, hygiene, food supply, cleaning crew), operations and security (i.e., media control, spatial management, security of premises), and central commander logistics were to be activated.
A dedicated and integrated authority was established by the state, tasked with collecting information from various parties (e.g., Israeli Defense Force: IDF, Ministry of Social Services, Ministry of Health, Hostages and Missing Family Forum). This authority created a background file for each returnee and forwarded it to the hospital staff as soon as their return was certain. Psychosocial and medical teams would then receive background information related to returnees’ age, family structure, significant losses, traumatic exposure and any information available pertaining to preexisting medical or psychosocial conditions. Social workers were tasked with receiving pre-designated family members of returnees, providing support to awaiting families and counseling them in preparation for their reunion with returnees, while psychologists attended to the returnees at the hospital entrance and guided them through the initial step of family reunification.
To ensure privacy, the entrance of the Safra Children’s Hospital was blocked off from the media and unverified visitors or personnel. Entrance to the facility was permitted only to identified staff members, which received a specific name tag and hand-band. Family reunification was highly prioritized and therefore, returnees would be immediately accompanied to meet their families in the privacy of their designated rooms. Next, provision of basic needs (e.g., preferred meals, shower, change of clothes, hygiene items), would be attended to, followed by an evaluation of mental state and needs, introduction to medical personnel and invitation to conduct medical exam. If evidence of sexual or physical abuse is detected or disclosed by the returnee, appropriate professionals would be consulted to determine the feasibility of collecting further evidence without exacerbating distress. If needed, forensic exams would be offered as well. Finally, interviews with a designated, pre-trained security intelligence officer would be offered to all returnees above the age of 14, to allow for the gathering of crucial information pertaining to the fate of hostages who were still held in captivity. Next, in agreement with returnees and their families, discharge meetings would be conducted during which a discharge plan would be made.
Personalized-careA vital goal of acute interventions is the early identification of trauma related reactions and the delivery of preventive interventions that could reduce the risk for acute stress disorder and PTSD [35]. To this end, and in line with the acute trauma-informed approach, screening for both acute and post-acute traumatic stress responses was to be performed [36]. Standardized measures that would rely upon returnees’ self-report were deemed inappropriate due to the sensitive, and highly unpredictable, conditions of returnees. Instead, screening relied on clinical observations, both documented in returnees’ medical files and through clinician-rated responses to modified standardized measures as described below:
A clinician- rated child symptom checklist was developed by the authors and sent via a secure electronic link to all clinicians. The checklist was based on the Trauma Symptom Checklist for Young Children (TSCYC) [37], a 90 item scale comprised of eight-factors for young children, and the Trauma Symptom Checklist Short Form (TSCC- SF) [38], a six-factor, 29-item scale for children and adolescents. Both measures pertain to children’s trauma- and abuse-related symptomatology as assessed by caretaker report, and were found to have well established psychometric properties [39].
Caregiver symptoms were assessed using the Adult National Stressful Events Survey Acute Stress Disorder Short Scale [NSESSS] [40, 41], a 7-item measure evaluating the severity of acute stress disorder symptoms in individuals age 18 and older following an extremely stressful event or experience. The scores for both child and adult scaled items were dichotomized to ‘present’ or ‘absent’. Findings pertaining to returnee physical symptoms were collected from medical files.
Optimal safetyA core principle in providing psychological first-aid response to acute trauma survivors consists of regaining a sense of control and safety [42]. This is usually attained by providing survivors with information and space to express their concerns while ensuring that their needs and voices are heard [43]. To this end, the Optimal safety component focuses on well-recognized reciprocal elements comprising Psychological First Aid [44], with particular attention given to developmentally-informed needs. These elements consist of (1) physical safety, (2) calming, (3) promoting connectedness, (4) attending to returnees’ basic needs, (5) promoting self-efficacy, and (6) instilling hope, gradually implemented and individually tailored to ensure optimal safety, as delineated in Fig. 2.
(1) Physical SafetyPhysical Safety refers to the importance of providing food, protection, and connectedness [44, 45]. All returnees would be primarily received by the Red Cross and transferred to the IDF special reception teams (see Fig. 1 for Release Process). IDF medical personnel would assess whether urgent medical care is indicated, in which case returnees would be transported to the nearest medical center. If urgent medical care is ruled out, returnees would be provided with basic elementary needs, including: change of clothes, water and snacks. When possible, IDF personnel would engage children and parents through play and provide orienting information, including a verbal account of their intended next steps (i.e., transportation via helicopter or vehicle to the Safra Children’s Hospital, where their families await).
(2) CalmingGiven prevalent neurophysiological dysregulation following traumatic exposure [46, 47], staff were trained to maintain a calm, compassionate presence, limiting demands placed on returnees and providing accurate information [48]. Particular attention would be devoted to supporting caregivers as studies demonstrate the vital co-regulatory role of caregivers for young children [49], as well as the crucial impact of parent–adolescent interactions in the aftermath of highly stressful events [50]. Therefore, all caregivers would be provided with professional support aimed at self-stabilization and parental guidance.
Considerable attention was also devoted to returnees’ hospital environment. After careful consideration, a dedicated facility within the Safra Children’s Hospital was chosen. This unit was tailored to meet the needs of children, adolescents, and families. It features child-friendly décor, private rooms, and communal areas to provide flexibility in privacy and social interaction, shielding returnees from unwanted exposure to visitors or experiences shared by fellow returnees. Dim lighting would be maintained within the facility to counter potential effects of light deprivation during captivity. Staff were trained to speak softly and to minimize their presence, to allow for returnees’ privacy and comfort. Steps were taken to protect returnees from visitors, media, and unwanted external stimuli. Furthermore, the enrolment of female staff members was preferred to mitigate power dynamics and establish a sense of safety, especially as traumatic experiences were primarily inflicted upon hostages by male perpetrators and some evidence exists indicating preferences for female providers, particularly pertinent to disclosure of sexual abuse [51].
(3) ConnectionHuman connection enhances a sense of continuity in face of disruption and trauma, provides models of resiliency which could bolster survivors’ own sense of competence, and increases their access to tangible and non-tangible resources [52]. Accordingly, family reunification has repeatedly been cited as a priority in disaster and mass trauma response, especially for children and adolescents for whom the stress resulting from delayed family reunification has been associated with significant and prolonged negative effects [53, 54]. Appropriately the World Health Organization (WHO) advocates for family reunification as an essential component of promoting mental health in post-disaster response [55]. Connection would therefore be facilitated in several ways. For instance, core teams would meet returnees at the entrance of the Children’s Hospital to establish a personal connection, and immediately escort them to their closest family members, where they would reunite in a private setting before gradually connecting with additional family members.
(4) Basic needsAddressing children's and families’ basic needs is crucial for restoring stability and promoting a sense of control following traumatic exposure [42]. Once physical safety is ensured and returnees reunite with their families, food, shower facilities, and clothing would be offered, with specific attention given to providing well-fitting and age-appropriate clothing, as oversized or ill fitted clothing could serve as trauma reminders [56]. Potential developmental regression was taken into account with regards to all returnees, therefore, different needs would be prioritized based upon age, ongoing clinical observation, and communication with returnees and their family members. For example, earlier access to their peer group would be facilitated for adolescents, while younger children would be given toys and other comforting items. Adults and care givers would be prioritized with regards to access to information.
(5) Self-efficacyAdult returnees would be encouraged to make personal choices regarding their hospital stay duration, environment, media exposure, and medical/psychological care. Parents would be encouraged to facilitate these decisions for their children, in a developmentally appropriate manner, with the aim of empowering and re-establishing parental roles. In addition, services such as dental care, haircuts, and cosmetic care would be offered upon request, as these are linked to personal identity and self-efficacy [57]. Retrieving personal items and allowing personal choices, including hairstyles, are important aspects of survivors’ identity reclamation process [58].
To further enhance self-efficacy, self-regulation and independence, evidence-based trauma-informed interventions were included in the protocol. Soon after their arrival to the hospital, all families and returnees would be informed of the expected course of events to establish predictability. Psychoeducation on expected psychological, physiological, emotional, and behavioral reactions, along with immediate and long-term response recommendations, would also be provided. The team would prioritize validating and supporting family members’ reactions, concerns, and needs. They would provide training in basic relaxation and cognitive coping skills to allow regulation of arousal, enhance resilience and manage various stress responses. Returnees with children would be offered parent guidance, including psychoeducation on developmentally informed traumatic stress reactions in children and the crucial role of primary caregivers in identifying these reactions and intervening early by re-establishing predictability, safety and open developmentally-informed communication. This information would be shared privately with parents or, when feasible, in dyad sessions, facilitating deeper understanding of anticipated stress and trauma-related responses and recommended trauma-informed practices.
As family members were expected to provide devastating news regarding their community, other family members or friends that were either murdered or are still held in captivity, notification protocols were to be followed, including SPIKES (Setting, Perception, Invitation, Knowledge and Empathy), often used by medical professionals [59]. Special care would be taken when delivering bad news to children and adolescents. Teams would then offer guidance to caregivers and, when requested, deliver bad news alongside family members. Whenever possible, psychoeducation on traumatic grief responses would be provided to adults, parents, and children, with specific developmental needs in mind.
(6) HopeA central objective of terrorism is fostering hopelessness [60]. One aspect of hopelessness is a sense of a foreshortened future, which is well-recognized as a prominent posttraumatic symptom [61]. Following disaster, adolescents have conveyed a decrease in hopeful thinking [62]. Therefore, a vital component of Psychological First Aid is facilitating hope. Survivors, who often perceive challenges stemming from mass trauma as one unsolvable problem, could greatly benefit from enhancing problem-solving strategies. Not only does this help prioritize the overwhelming bombardment of practical tasks that they face, but it could also enhance their sense of control and instill hope [63]. This would be achieved by the provision of developmentally informed psychoeducation, connection to psychosocial, communal and medical resources, and delineation of a detailed discharge plan. For parents, these interventions could reinstate their sense of control and authority, subsequently reassuring their children and instilling hope in them as well. For adolescents, who rely heavily on their parents and peers, special attention was placed on gradually re-connecting them to their social resources by reassuring them that their network has been eagerly awaiting their safe return.
Fig. 2
Basic components of Optimal Safety, including, specification of primary action items depicted in boxes
Navigating dischargeRecognizing potential future deterioration, we followed post disaster recommendations and intended to coordinate care continuity through careful planning of pragmatic manageable steps [64, 65]. Upon hospital discharge, family members and parents were to be provided with brochures and handouts including important information regarding developmentally informed expected reactions, review of principles for coping with such reactions, and information necessary in case they wish to reach out to Sheba staff members in the future. In addition, connection to community-based resources was a major priority led primarily by the psychosocial teams. Follow up was to be conducted a week and two weeks after discharge, by telephone and in some cases in person, as directed by the Ministry of Health. This was to ensure that needs and wants were met once the returnees were in the community.
Assessment of the ReSPOND protocol implementation and feasibility was obtained via multi-level supervision conducted by highly experienced adult- and child-trauma as well as medicine experts. This team oversaw protocol development and implementation beginning with training; supervisors participated in live simulations, observed trainees undergo live and video-based simulations, and offered immediate on-site feedback, modeling and guidance. Therefore, feasibility would be assessed based upon supervisors’ feedback pertaining to the ReSPOND protocol implementation.
留言 (0)