
記住我








The present study is a longitudinal cohort study and the database was from NHANES. NHANES serves as a comprehensive survey designed to amass data on the health status of the United States population. Employing a stratified multistage random sampling methodology, NHANES ensures the representation of a national sample [20]. NHANES was granted approval from the ethical review board of The National Center for Health Statistic, with each participant providing informed consent via signed agreements [21]. The datasets, replete with thorough documentation and protocols, are publicly available on the NHANES website, aligning with the laboratory technologists and anthropometry procedures of our previous studies [22, 23].
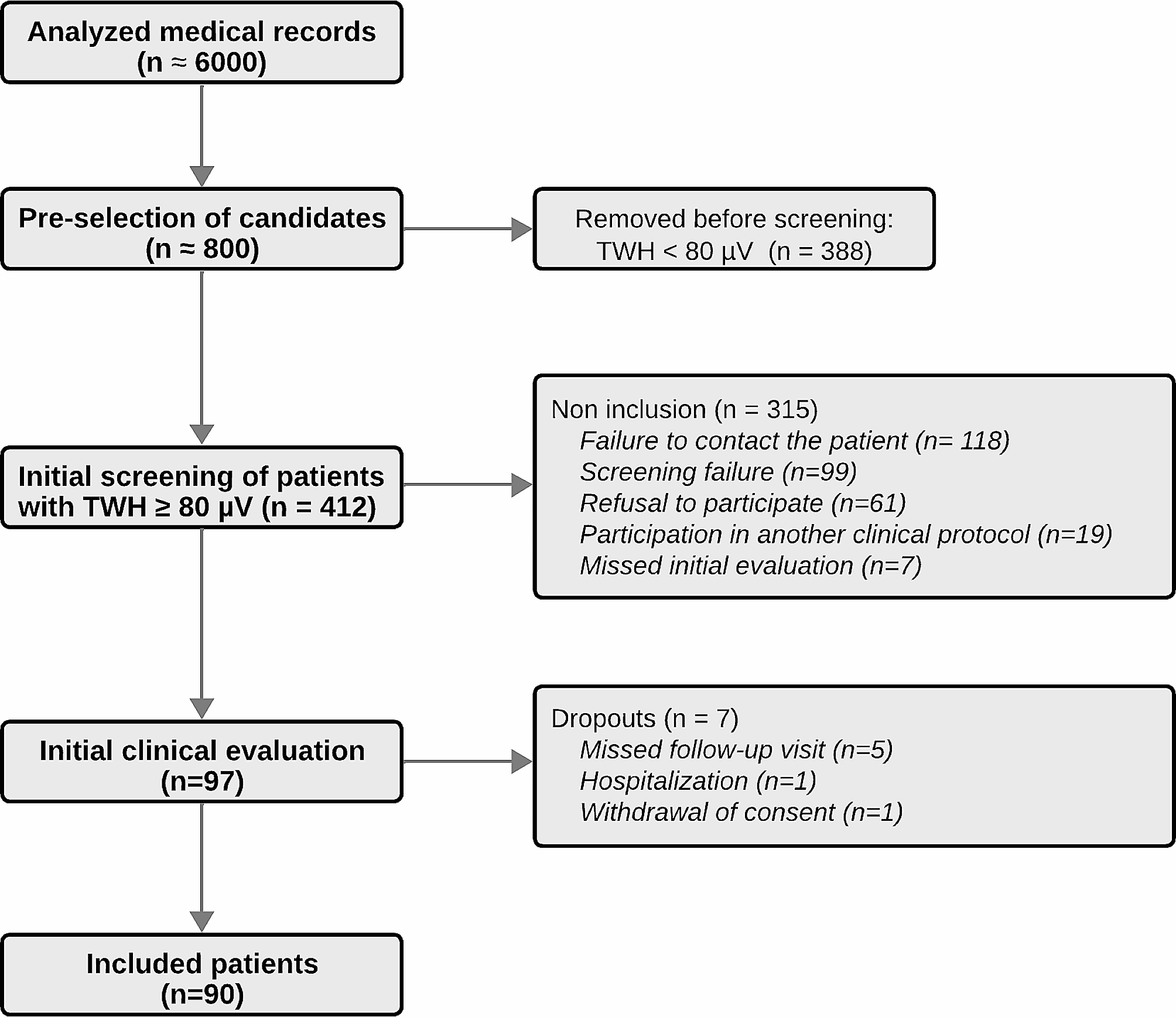
For the present prospective cohort study, we screened and analyzed data spanning 6 two-year cycles from 2005 to 2016. To uphold the integrity and reliability of results, the specific exclusion criteria were applied including (1) individuals<65 years of age (N=52734); (2) individuals without complete mortality data (N=13); (3) individuals without CMI value (N=4907); (4) individuals without records of necessary covariates including weight (N=6), leukocyte (N=15), drinking status (N=157), smoking status (N=4), eGFR (N=14), the history of hypertension (N=5), DM (N=8), coronary heart disease (CHD) (N=27), angina (N=9), heart attack (N=6) and stroke (N=2). A total of 3029 participants were enrolled from the years 2005 to 2016 in our study (Fig. 1).
Fig. 1
Flowchart of study participants
Assessment of CMIThe CMI was calculated using the formula:
CMI = triglyceride (TG, mmol/L) / high-density lipoprotein cholesterol (HDL-C, mmol/L) waist circumference (WC, cm)/ height (cm) [15].
CMI was treated as a continuous exposure variable in our study and all enrolled participants were stratified into tertiles based on CMI values for subsequent analyses.
Assessment of all-cause and cardiovascular mortalityIn the present study, the primary outcomes included all-cause and cardiovascular mortality. To determine the mortality status, the NHANES public-use linked mortality file as of December 31, 2019, was utilized in conjunction with the National Death Index (NDI) by the National Center for Health Statistics (NCHS) through the implementation of a probability matching algorithm. Additionally, the International Statistical Classification of Diseases, 10th Revision (ICD-10) was utilized to underly the cause of death. Cardiovascular mortality was described as death as a consequence of diseases of the heart (I00-I09, I11, I13, I20-I51) and cerebrovascular diseases (I60-I69) [24].
CovariatesIn the present study, following covariates were collected including gender, age, race, education level, family poverty-to-income ratio (PIR), body mass index (BMI), WC, waist-to-height ratio (WHtR), smoking, drinking, leukocyte, neutrophil, lymphocyte, systemic immune-inflammation index (SII), neutrophil to lymphocyte ratio (NLR), hemoglobin, platelet, albumin, total cholesterol (TC), TG, low-density lipoprotein cholesterol (LDL-C), HDL-C, creatinine, blood urea nitrogen (BUN), estimated glomerular filtration rate (eGFR), urinary albumin-creatinine ratio (UACR), hemoglobin A1c (HBA1c), hypertension, DM, cardiac disease history and stroke history.
BMI was the ratio of weight (kg) to height (m) squared. Smoking status was categorized into never, former and now according to the questionnaire "Smoked at least 100 cigarettes in life?" (SMQ020) and "Do you now smoke cigarettes" (SMQ040). Based on the questionnaire "Had at least 12 alcohol drinks/1yr" (ALQ101), drinking status was categorized into two groups based on whether participants had at least 12 drinks per year, and 1 unit of drink is equivalent to 12 ounces of beer, 5 ounces of wine, or 1.5 ounces of liquor. The chronic kidney disease epidemiology collaboration (CKD-EPI) formula was utilized to calculate the eGFR [25]. The self-reported questionnaires were used for the diagnoses of hypertension (BPD035), DM (DIQ010), heart failure (MCQ160b), CHD(MCQ160c), angina (MCQ160d), heart attack (MCQ160e) and stroke (MCQ160f).
The formulas for calculating the relevant indexes are as follows:
WHtR = WC (cm)/ height (cm),
NLR = neutrophil (/L)/lymphocyte (/L),
SII = platelet (/L) *neutrophil (/L)/lymphocyte (/L).
Statistical analysisAll statistical analyses were performed with R software (version 4.2.2), EmpowerStats (version 2.0) along with the use of rms package and MSTATA. Categorical variables are expressed as frequencies and percentages, while continuous variables are expressed as medians and interquartile ranges. The Chi-squared test or Kruskal-Wallis H test was used to analyze various CMI tertile categories. A statistically significant result was determined as a two-sided p-value<0.05.
Multivariate Cox proportional hazard models were estimated for the associations of CMI with all-cause and cardiovascular mortality. The findings were displayed in the form of hazard ratios (HRs) and 95% confidence intervals (CI). Model 1 was unadjusted. Model 2 was modified to account for gender, age, and race. Based on Model 2, Model 3 additionally adjusted for smoking, drinking, leukocyte, hemoglobin, platelet, weight, TC, eGFR, the history of hypertension, DM, CHD, angina, heart attack and stroke. Kaplan-Meier curves were conducted to estimate survival over time progression, with the log-rank test used to assess the disparity among the various survival curves. Additionally, the multivariate logistics and Cox regression were performed in the associations between inflammatory indicators with CMI, all-cause mortality and cardiovascular mortality respectively. The inflammatory-related indicators included leukocyte, neutrophil, lymphocyte, NLR and SII. The identical statistical techniques mentioned above were also utilized in the subgroup analyses to investigate potential differences among specific populations including gender, race, education level, family PIR, hypertension, DM, smoking and drinking subgroups.
"mediation" package in R 4.2.2. was utilized to perform Mediation analysis assessing the mediating effects of inflammatory indicators (leukocyte, neutrophil, lymphocyte, NLR, and SII) on the associations of CMI with mortality, adjusted by gender, age, race, smoking, drinking, hemoglobin, platelet, weight, TC, eGFR, the history of hypertension, DM, CHD, angina, heart attack and stroke. The presence of a mediating effect was defined as satisfying all of the following conditions having a significant indirect effect, a significant total effect, and a positive proportion of the mediator effect.
留言 (0)