Combining digital data obtained from a patient pool comprised of various real-world data sources can predict the efficacy and possible adverse event profile of investigational drugs [7]. Recruiting and enrolling a large patient population for clinical trials is currently wrought with obstacles, and these issues are magnified in the case of rare diseases such as cGvHD. In addition, there is a trend towards redesigning of clinical trials to provide options other than large randomized studies, as exemplified by the opinions expressed in the “2020 treatment of cGvHD report” by the NIH cGvHD Consensus Project on Criteria for Clinical Trials (https://ncifrederick.cancer.gov/events/conferences/sites/default/files/inline-files/NIH_2020_CGvHD_conference_Introduction_PDF.pdf) and a call for alternative trial designs and need for trials without steroid treatment arms. In this study, we demonstrated the feasibility of creating a DT cohort of cGvHD patients in the first-line treatment setting (flGvHD DT cohort) using the Trial Accelerator™ DT platform, which includes a large database of patient data collected from various sources worldwide. This approach has been proven to objectively improve clinical development planning and protocol design optimization [7, 8]. Additionally, we also showed that this digital cohort can be used to construct a control treatment arm—the SOC arm—to validate the efficacy of standard treatment regimens; here we assessed the efficacy of prednisone as first-line treatment. Our findings using this simulation modeling approach are in agreement with and confirm findings from real-world clinical settings. This demonstrates that pre-existing and carefully collated data for a relevant and commonly applied therapy can be used to obtain meaningful results on drug efficacy. Such a digital arm can be used as a comparator arm for testing novel therapies in real-world clinical trials or for designing randomized studies with appropriate power and endpoints.
The baseline profile of the flGvHD DT cohort may be predictive of the patient profile obtained at the first-line treatment setting while applying the specific inclusion/exclusion criteria used here. The DT profile constructed herein suggests that patients present with cGvHD at a median of 7.5 months post transplantation. In agreement with the above, Arora et al. [12], in a prospective cohort study of 911 HCT recipients, reported that the time to onset of cGvHD was 7.4 months post transplantation [10]. Other studies have reported various post-transplantation onset times such as 162 days (5.4 months) [13], 153 days (5.1 months) [14], and 5.9 months (7.3 months for classic cGvHD, and 5.9 months for overlap type cGvHD) [15]. These time frames are well aligned with the 7.5-month timeframe derived from a very large and diversified dataset in the current study.
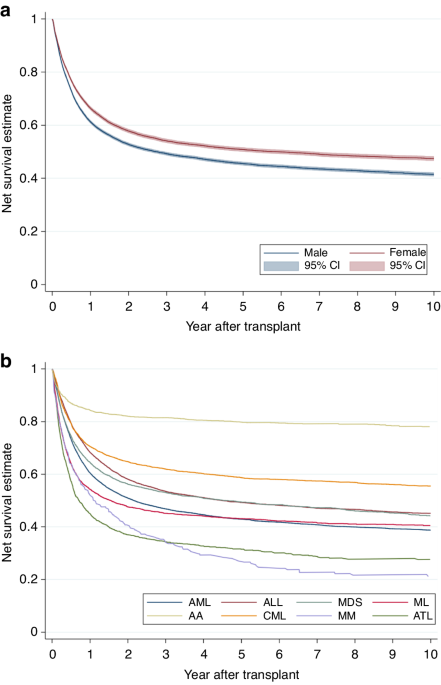
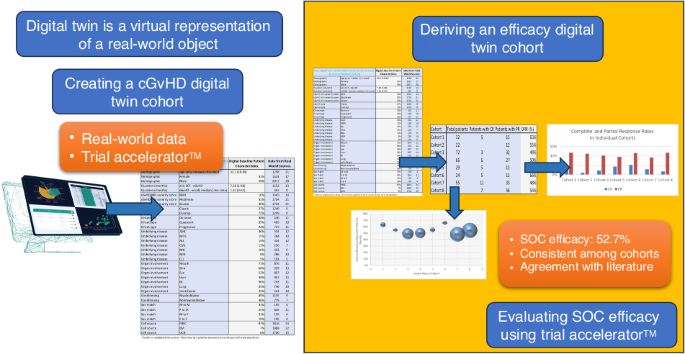
The ORR for first-line glucocorticoid therapy is reported to fall between 40 and 60% [3] and the efficacy analysis result for the flGvHD DT SOC is in agreement with the above, at 52.7% (measured at six months). An examination of the OS data (in cohorts with available source data) showed that the OS was 79% at 24 months after treatment initiation, with no statistically significant difference across cohorts (Supplementary Table S4). The above observations demonstrate that reliable and robust data can be obtained from diverse sources to construct DT arms and support the potential utility of DT SOC arms in real-world clinical trials.
While the analysis of individual patient data (IPD) associated with clinical trials has benefits, the resources, efforts, and inter-investigator cooperation required for such research will continue to limit the usage of IPD in many crucial areas of clinical research. In this regard, DTs can be used to obtain meaningful knowledge in a cost-effective manner. In addition, the regulatory approval of new drugs is based on aggregate patient data, rather than on IPD. Therefore, data from similar or identical studies employing the same agent can be combined with real-world patient data to accurately mimic placebo/comparator outcomes and create DT trial arms, which can then be utilized to detect early warning signs of trial results, safeguard patient safety, promote regulatory interaction, and improve submissions [7, 16]. As already mentioned, the FDA has been explicit about the value of such technologies and has issued the “Artificial Intelligence/Machine Learning (AI/ML)-Based Software as a Medical Device (SaMD) Action Plan”, which indicates that historical virtual control arms may be allowed in submission packages in the future. The method described here provides a reliable, consistent, and cost-effective option to construct historic control arms.
Despite its benefits, DT technology is associated with several challenges. First, as the strength of the technology lies in the size of the dataset used to construct the DT, the acquisition of large volumes of data is crucial; in this regard, data acquisition presents the most serious challenge [17]. In this study, the large size of the Trial Accelerator™ database allowed us to obtain an adequately large sample population for constructing the DTs. Second, as the data are sourced from numerous clinical studies conducted at diverse sites worldwide, data heterogeneity is a significant obstacle. In this study, only eight of the 32 cohorts could be included in the efficacy arm due to heterogeneity in the studies (outcome measures, treatment duration, and definition used for establishing ORR). Differences in the definition of the outcome measure (ORR) and treatment duration necessitated the exclusion of several cohorts during the construction of the efficacy DT. Additionally, data on failure-free survival (FFS), an increasingly important outcome measure in cGVHD studies, were not available for all the cohorts, and FFS was thus not used as an efficacy metric for the DT. It is important for clinical trial investigators to standardize the choice and reporting format of key parameters that can be used as modal values in AI-driven technologies. This will improve the accuracy and ease of development of DTs in the future. Third, as our study objective was to construct a DT of cGvHD patients at first-line treatment, we did not address the issue of “progressive onset” of cGvHD, even though the outcome in patients with progressive onset cGvHD is known to be significantly poor at first-line treatment. Fourth, the generalizability of the DT constructed here is limited to the population that falls strictly within the inclusion/exclusion criteria. It is thus important to validate this technology in various disease scenarios in GvHD. In addition, a small proportion of studies (4 of 18 in the baseline DT and 1 of 8 in the SOC cohort) are >10 years old. In our experience data shifts happen when quantifiable events occur, such as the introduction of a new treatment. As such events have not occurred, we did not feel the need to exclude these older studies. A statistical analysis of ORR data with and without Cohort 2 (older than 10 years) showed no statistical impact on the ORR results (data not shown).
In summary, AI-driven DT technology has the potential to significantly improve clinical trial design and implementation. In this study, we demonstrated the construction and application of a DT cohort in cGvHD for describing certain baseline clinical characteristics and showed that existing data can be used to validate that the SOC efficacy (as determined by the 6-month ORR) barrier that needs to be overcome by a new drug (to show superior efficacy compared to the SOC) is 52.7% in this population. The power of converting data into knowledge can be exemplified by the ease with which investigators can modify the inclusion/exclusion criteria in different scenarios to evaluate the effect of such changes on the baseline cohort profile and efficacy of the drug. The DT control arm could potentially function as an External Control Arm in a prospectively planned and implemented single-arm clinical trial, and solve certain ethical dilemmas surrounding placebo arms. It is hoped that this technology will gain regulatory approval in the future and find its place in the design and implementation of clinical trials.


留言 (0)