
記住我









This study was a post hoc analysis of the CRHCP trial, which was designed to test the effectiveness of a non-physician community health-care provider-led intensive BP intervention (< 130/80 mmHg) compared with usual care among hypertensive patients. It was approved by the ethics committees of the First Hospital of China Medical University and performed in 326 villages from three provinces (Liaoning, Shanxi and Hubei) in rural China. All participants have signed informed consent at screening visits. All data used in this study were obtained from the CRHCP.
Study Design for CRHCPThe design and main results of CRHCP have been published [15]. In a word, as an open-label, blinded-endpoint, cluster-randomized trial, participants aged 40 years or older, with an untreated SBP ≥ 140 mmHg or a diastolic BP (DBP) ≥ 90 mmHg (≥ 130 mmHg and ≥ 80 mmHg for those with high CVD risk or if currently taking antihypertensive medication) were recruited. 326 villages were assigned to a non-physician community health-care provider-led intervention or usual care randomly. In the intervention group, providers were trained and implied antihypertensive management to achieve a BP goal of < 130/80 mmHg. A total of 33,995 participants were enrolled from May 8 to November 28, 2018 and followed for clinical events over 36 months. More details on the outcomes and procedure could be available in published papers [16].
Randomization and maskingRandomization and masking for this study was mainly located at CRHCP. Randomization was stratified by provinces, counties, and townships. A total of enrolled 163 villages were randomly assigned to intervention and 163 villages to usual care by a biostatistician from the Tulane University Translational Science Institute (Fig. 1). Since it’s a cluster-based implementation program, the participants, providers, and research staff for data collection were unblinded. However, the randomization assignments were concealed before the completion of recruitment and enrollment. Besides, the process of clinical outcome assessment was blinded to randomization.
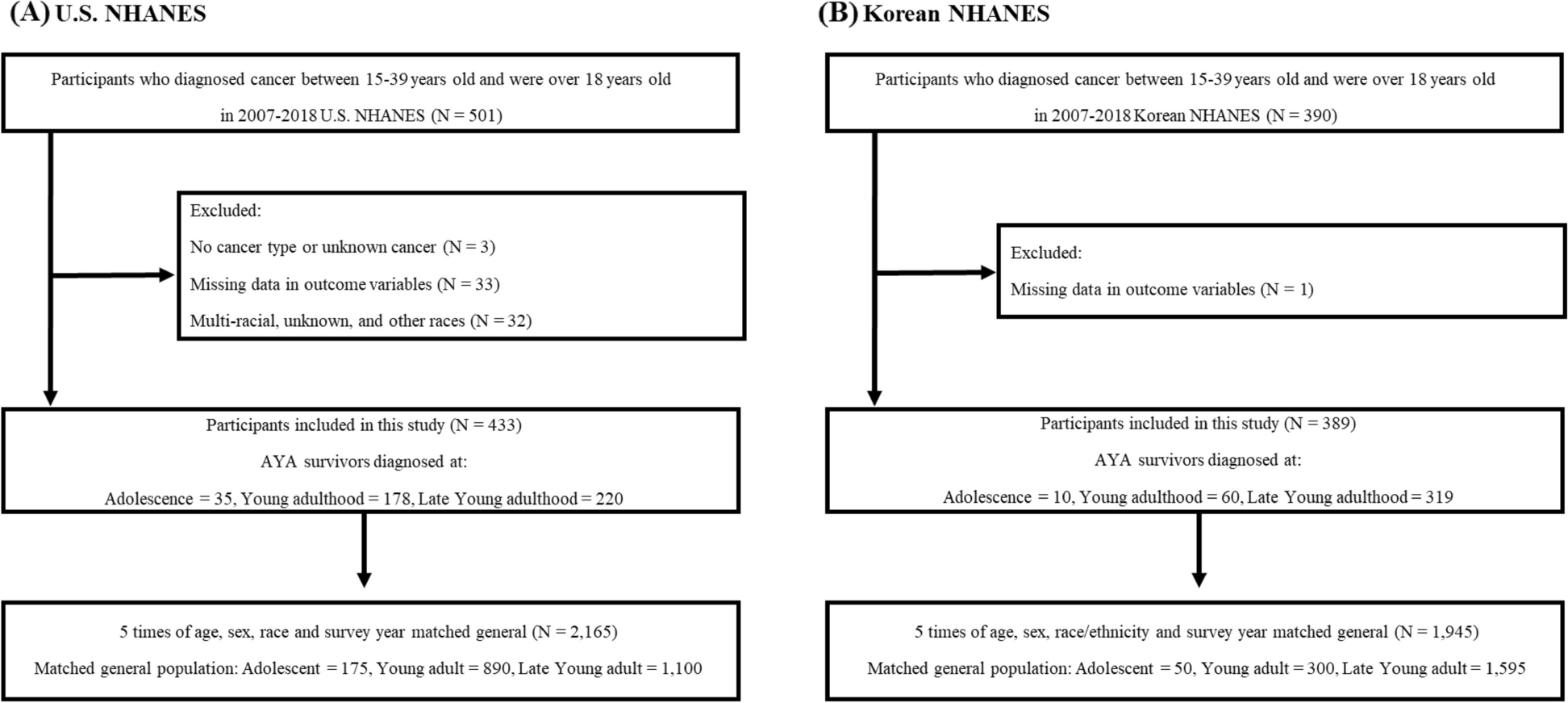
Fig. 1
Flowchart of the study. The randomization, recruitment, enrollment and baseline CVD risk quartile of this study are shown
Participants stratifications and Groups for this studyThis current study screened all eligible participants from CRHCP, among which participants who had a history of CVD, over 80 years old, or missing data were excluded from this analysis since the calculation of ASCVD risk by the American College of Cardiology/American Heart Association Pooled Cohort Equations. We used the same estimation method as outlined in our main article [15] and the Pooled Cohort Risk Equations were accepted and recognized worldwide. During stratification, the distribution of CVD risk was first assessed and it was found that the estimated 10-year risk in the lowest one was less than 5.1% if using quartiles, which matched the low risk category (less than 5%) in risk assessment system. Thus, the whole enrolled subjects were stratified into quartiles by baseline 10-year CVD risk estimation. For each quartile, subjects were assigned to intervention or usual care group according to the original randomization of CRHCP. The flowchart of this study was presented in Fig. 1.
Intervention and MeasurementsDemographic data was collected at baseline, while laboratory indexes were measured at both baseline and 36 months. Biological sex was self-reported by participants. BP measurements were taken three times every six months, with participants resting in a seated position for five minutes each time. The collected measurements were promptly submitted to the study data center, where they were pooled and analyzed to identify trends in BP control.
To ensure a comprehensive overview of health outcomes, cardiovascular incidents, and other potential adverse events were systematically monitored by the CRHCP study group every six months. Detailed information about cardiovascular conditions and mortality rates was amassed through a standardized questionnaire, which included an extensive array of variables such as medical history, CVD risk factors, and specific symptoms. The study also rigorously tracked a range of conditions including injurious falls, all forms of hypotension, and syncope, while electrolyte levels and renal function, indicated by estimated glomerular filtration rate (eGFR), were documented as integral components of the adverse outcomes assessment.
Participants in the intervention group were given the same management across all estimated CVD risk stratification. An integrated, multi-faceted treatment strategy was executed by trained non-physician community health-care providers, aiming to achieve a BP target of < 130/80 mmHg. In contrast, participants in the control group were subject to standard care practices. The community health-care providers in the intervention group, under the supervision of hypertension specialists and primary care physicians, were rigorously trained in a comprehensive, protocol-based antihypertensive regimen. This regimen included in-depth instruction on treatment algorithms, pharmacological selection, contraindications, and titration strategies. Furthermore, these providers received extensive training in patient health education, covering essential aspects such as home BP monitoring, adherence to medication, and lifestyle modifications. The role of these community health providers was multifaceted, encompassing the initiation and adjustment of antihypertensive medications, direct medication delivery to patients, health coaching, instruction in home BP monitoring practices, and the organization of social support groups. They received a portion of their salaries and performance-based incentives from research grants for study-related activities. To promote engagement and adherence, patients in the intervention group were provided with monthly supplies of antihypertensive medications at discounted rates or free of charge, accompanied by complimentary home BP monitoring devices. Additionally, they received consistent health coaching sessions facilitated by a dedicated team of non-physician community healthcare providers, ensuring a comprehensive, supportive, and well-monitored treatment environment.
Study outcomesWe examined the primary outcomes in this implementation study which was defined as the first occurrence of major CVD events composing of myocardial infarction, stroke, heart failure requiring hospitalization or CVD deaths during the 36-month follow-up. We also examined adverse events to reflect intervention safety. Serious adverse events included deaths and hospitalizations in this analysis. Besides, injurious falls, hypotension, symptomatic hypotension, syncope, electrolyte abnormalities, and renal outcomes were compared and presented. Details of events adjudication had been published in the previous article by our study team [15, 16]. All study outcomes were adjudicated by the Endpoint Adjudication Committee.
Statistical analysisThe predicted ASCVD risk was calculated based on the American College of Cardiology/American Heart Association Pooled Cohort Equations [17]. The eGFR was calculated based on the 2021 Chronic Kidney Disease Epidemiology Collaboration Creatinine Equation [18]. Baseline demographics, risk factors, and end point BP of intervention and usual care treatment stratified by estimated CVD risk were calculated as mean ± standard deviation for continuous variables and number (percentage) for categorical variables. They were compared with the use of the Chi-square test, Wilcoxon rank-sum test, and the Student’s t-test, as appropriate. Tests for trend across quartiles of estimated CVD risk were conducted by modeling the quartiles as a continuous variable in linear regression models for continuous variables and the Cochran-Armitage test for trend for categorical variables. The Kaplan–Meier curves were drawn and log-rank test was used to detect the difference of event incidences between groups. Mixed-effect Cox proportional-hazards models were used to estimate the hazard ratios (HRs) and 95% confidence intervals (CIs) of primary outcomes, all-cause mortality and CVD mortality associated with the intervention in each quartile, setting the village as a random effect. Baseline covariates including age, sex, cigarette smoking, use of antihypertensive medication, and baseline SBP, low-density lipoprotein cholesterol, and fasting plasma glucose were also adjusted. To test the interaction effect, a multiplicative interaction term between intervention and estimated CVD risk quartiles was additionally introduced to the regression model. We also calculated the absolute risk reduction (ARR) and number of person-years needed to treat (NNT). In our study, we employed the “iri” statement within the Stata software to compute ARR. ARR is defined as the absolute disparity in risk between two groups, specifically the usual care group and the intervention group. The ARR was calculated using the formula: ARR = Risk in the usual care group—Risk in the intervention group. It's important to note that the risks were expressed as rates per person-year. Benjamini–Hochberg method was applied to control the false discovery rate (FDR) in the subgroup analysis for the comparison of primary outcome events, all-cause death, and CVD death. Two-tailed P values < 0.05 were considered statistically significant for all analyses. Statistical analysis was conducted with the use of Stata MP 17.0 and R software 4.2.0.
留言 (0)