
記住我








A 38-year-old male patient visited the emergency department of an acute-care hospital because of acute exacerbation of abdominal pain that had persisted for a month. He was previously diagnosed with Wolff–Parkinson–White syndrome and was under observation due to no history of arrhythmia. Although his general condition was stable, he presented with strong spontaneous pain and tenderness at the upper abdomen. Consequently, he was admitted to the hospital and was followed-up. He underwent abdominal contrast-enhanced computed tomography (CT) scan on the next day. Results revealed an extensive thrombus from the intrahepatic portal vein to the supra-mesenteric vein without findings of thrombus in other regions or embolization in the arterial system. The patient was diagnosed with port-superior MVT and was transferred to a tertiary hospital.
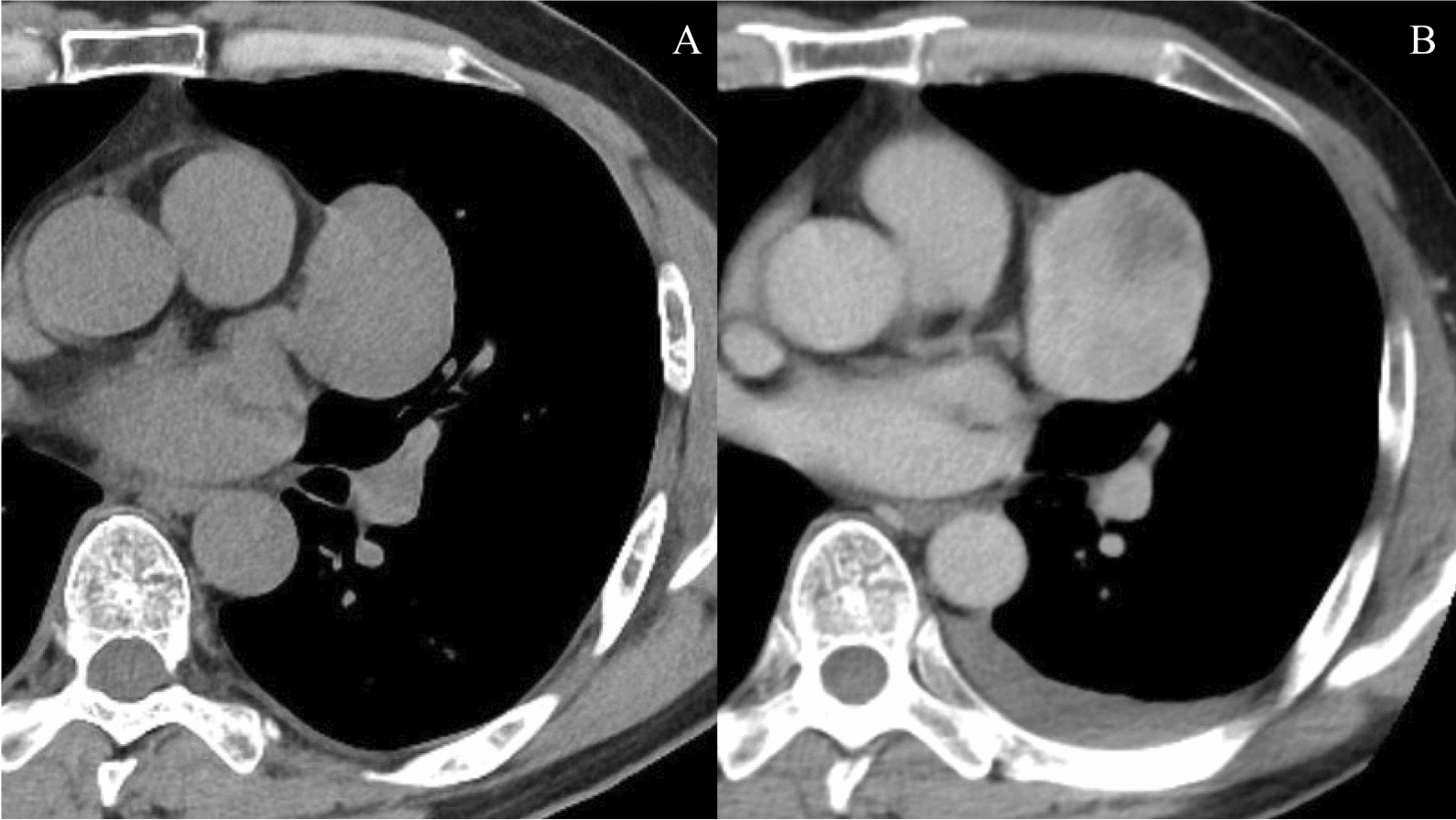
Upon hospital arrival, he was alert, and his vital signs were stable (respiratory rate: 12 cycles/min, heart rate: 69 beats/min with sinus rhythm, and blood pressure: 135/74 mmHg). He complained of diffuse abdominal pain with localized mild upper abdominal tenderness. Laboratory test results were almost normal except for the following: white blood cell count, 15,700/μL; C-reactive protein level 3.2 mg/dL, prothrombin time international normalized ratio, 1.46; and D-dimmer level 21.9 μg/mL. CT scan performed in a previous hospital revealed the development of collateral blood vessels around the portal vein, and there was no reduction in the contrast effect on the bowel wall (Fig. 1). Hence, the symptoms could have been caused by chronic MVT. The patient was managed with conservative therapy particularly anticoagulation therapy using heparin in the intensive care unit. However, he complained of abdominal pain exacerbation 6 h after admission. He underwent repeat abdominal CT scan. Results revealed increased peritoneal ascites and reduced contrast effect on the small intestine wall in the right upper quadrant (Fig. 2). Small bowel infarction was strongly suspected, emergent laparotomy was performed.
Fig. 1
Abdominal contrast-enhanced computed tomography scan performed in the previous hospital. The thrombus extended from the intrahepatic portal vein to the superior mesenteric vein (arrows). The small intestine in the right upper quadrant was swollen but contrasted
Fig. 2
Computed tomography scan after abdominal pain exacerbation. Ascites appeared (arrows), and the contrast in the small intestine reduced (arrowheads)
During emergent laparotomy, we found approximately 500 mL of light-brown ascites in the peritoneal cavity and a 90-cm-long ileum, which was 210 cm away from the Treitz ligament to the anal side, discolored with dark brown color and sclerotic. The ileum that was evidently necrosed was partially resected. Moreover, temporary abdominal closure with the Barker method for the purpose of a second-look surgery was introduced. On postoperative day (POD) 1, a part (50-cm-long) of the small intestine was additionally resected, and anastomosis was created via hand sewing using the end-to-end Albert–Lembert suture. Abdominal compartment syndrome had been a cause of concern because the whole bowel was edematous. Open abdomen was continued for several days. Open thrombectomy was not performed due to the absence of progression in intestinal necrosis after the initial surgery. The abdomen was closed on POD 3 after bowel edema improvement.
Paralytic ileus developed after surgery and lasted long. Although anticoagulation therapy with heparin was administered during the perioperative period, oral warfarin was initiated after paralytic ileus improvement. The patient was tested for various coagulation abnormalities during hospitalization and the protein C and S activities was reduced by 20% and 46.7%, respectively. In addition, protein C antigen was reduced by 23%. However, the patient did not have a family history of thrombosis. He was evaluated by an in-house hematologist. The patient was discharged on foot on POD 60.
He was followed-up at the outpatient clinic every 3 months. Anticoagulation therapy with warfarin was continued. During follow-up, he was referred to the department of hematology of a university by our in-house hematologist. Protein C and S deficiency was diagnosed. Although the genetic diagnosis including family members was proposed, the patient declined the offer, and no further test was conducted. The patient was initiated on lifetime anticoagulant therapy. For follow-up evaluation of portal hypertension, esophago-gastroduodenal endoscopies and contrast-enhanced CT scans were performed on postoperative years 3, 5, and 10. Endoscopies showed neither gastrointestinal ulcer nor gastroesophageal varices. CT scans revealed gradual recanalization, and the port-superior mesenteric vein was eventually recanalized with improvement of the collateral vessels around the portal vein on postoperative year 10 (Figs. 3 and 4). During the 10-year period, the patient did not experience any event suggesting thrombosis or embolus at other sites.
Fig. 3
Axial view of computed tomography scans showing changes in port-superior mesenteric venous thrombus and collateral vessels over time. Thrombus in the portal vein (arrows) disappeared three years later, and the diameter of the portal vein increased over time. Collateral vessels around the portal vein improved over time. Stenosis of superior mesenteric vein (dotted arrows) gradually improved compared with the superior mesenteric artery (arrowheads)
Fig. 4
Coronal view of computed tomography scans showing changes in port-superior mesenteric venous thrombus and collateral vessels. Note the gradual improvement of collateral vessels in parallel with the gradual increase in port-superior mesenteric vein diameter
留言 (0)