Our general approach was based on the principle used in the recent US Food and Drug Administration (FDA) guidance for in silico dose development of programmed cell death (ligand) receptor-1 (PD [L]-1) blocking antibodies for treatment of patients with cancer [11]. This guidance allows the adoption of alternative doses of monoclonal antibodies in the label of approved drugs without the necessity of a clinical study, when it can be shown by using pharmacokinetic modeling that equivalent exposure can be achieved with an alternative dose compared to the approved dose. Since there is a general rationale for such a strategy for all monoclonal antibodies based on pharmacokinetic and pharmacodynamic behavior, the principle of this guideline can be used as guidance for monoclonal bodies targeting other receptors as well [9].
2.1 Pharmacokinetic Model Simulation
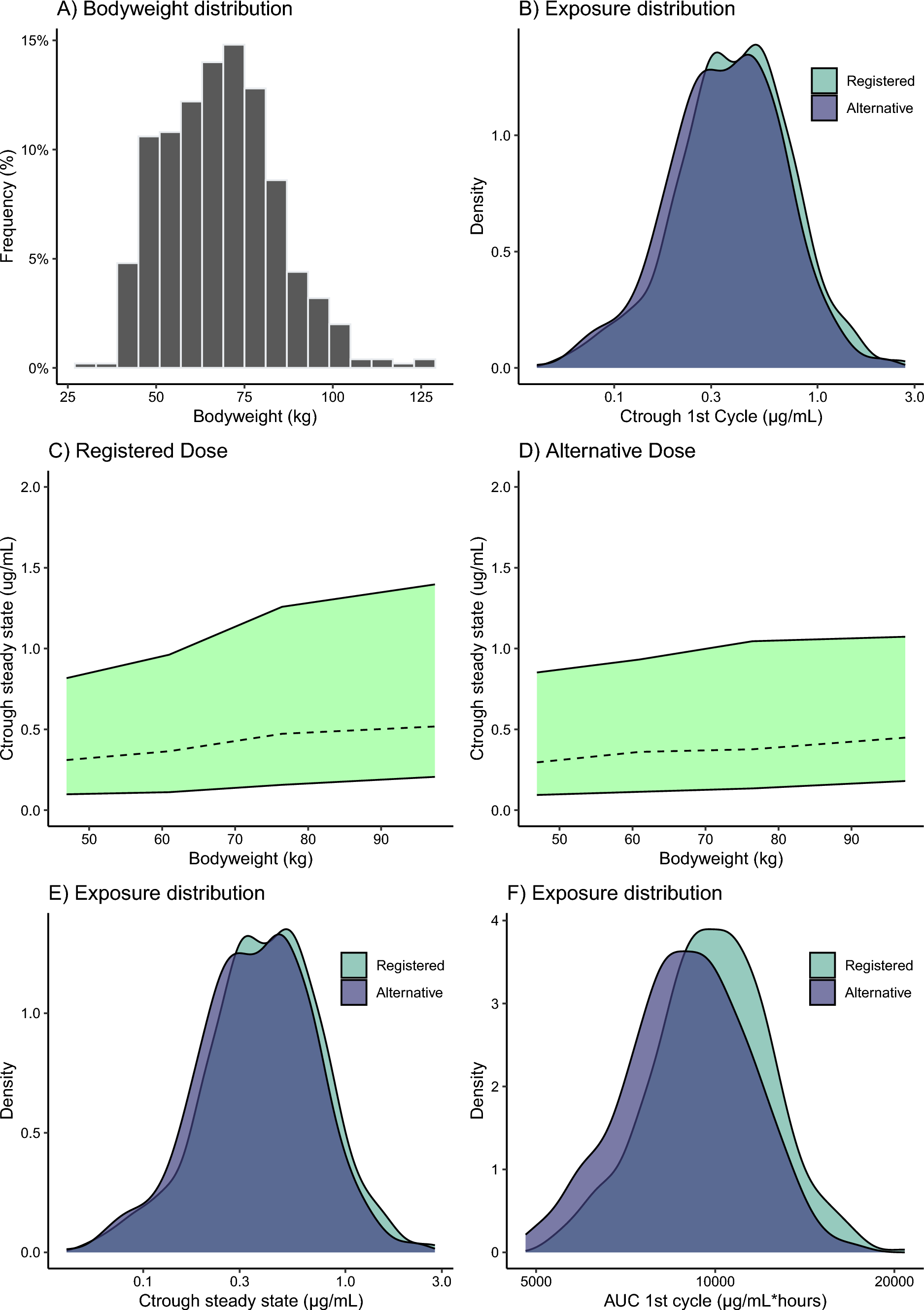
In short, in this guideline, equivalent exposure is defined as follows: the geometric means of the area under the concentration–time curve (AUC) over the least common time interval and trough concentration (Ctrough) following the alternative dosing regimen at steady state and/or in the first least common time interval are no more than 20% lower. For our in silico evaluation of alternative dosing regimens, we used the population pharmacokinetic model for sacituzumab govitecan, as published in the European Medicines Agency (EMA) public assessment report [10]. This linear two-compartment model described the pharmacokinetics of the intact antibody–drug conjugate. Using this model, a Monte Carlo simulation was performed using the non-linear mixed effects modeling software package NONMEM V7.5 (Icon, Dublin, Ireland). The NONMEM model code is supplied in the supplemental material of this manuscript.
2.2 Acceptance Criteria
Furthermore, according to this guideline the geometric mean of steady-state maximum concentration (Cmax) should not increase more than 25%. These criteria are well-aligned with bioequivalence boundaries for the geometric mean ratios for the AUC and Cmax of 0.8–1.25 for drugs without a narrow therapeutic window [12]. Since we consider antibody–drug conjugate drugs to have a narrow therapeutic index, we used the more conservative equivalence criteria of 0.9–1.11 [13] for the predicted geometric mean ratios, as previously proposed for these kinds of drugs for the current analysis.
2.3 Virtual Patient Population
We investigated alternative dosing regimens for the EU and US setting, as the vial sizes (200 mg in EU and 180 mg in the USA) and weight-banded dose recommendation will be different. For this purpose, we created two virtual populations of 500 participants: an EU population, with demographic data from the International Cancer Research Partnership, and a US population from the National Health and Nutrition Examination Survey (NHANES) database, both obtained from the PopGen virtual human population generator [14]. Since serum albumin was a covariate for the peripheral distribution compartment of sacituzumab govitecan, we assumed a serum albumin of 40 g/L [15], with an inter-individual geometric coefficient of variation of 5% during all our simulations.
2.4 General Approach
First, we predicted the pharmacokinetics of sacituzumab govitecan associated with the approved dose for both populations. For these simulations, we assumed exact dosing based on the body weight, without rounding. Thereafter, we explored alternative dosing regimens using the whole vials for the US and EU population separately. As the pharmacokinetics of the cytotoxic payload of sacituzumab govitecan (SN-38) are directly proportional to the pharmacokinetics of the total antibody–drug conjugate, the obtained predicted pharmacokinetics of the intact antibody–drug conjugate were used for our analysis of pharmacokinetic equivalence.
The simulated reference dosing regimen was 10 mg/kg on day 1 and 8 of a 21-day cycle, in line with the drug label. The alternative dosing regimen was based on the same administration days and 21-day cycle, with individual doses based on weight bands with the use of complete vials, while accounting for the established allometric (non-linear) relationship between body size and pharmacokinetics. For all dosing regimens, the average quantity of drug used per dose was calculated, under the assumption of complete wastage of a partially used vial.


留言 (0)