Trial design
A two-arm, parallel-group cRCT was performed. The study protocol [23] was registered in the University Hospital Medical Information Network (UMIN) Clinical Trials Registry (UMIN-CTR ID, UMIN000038044). First registration date was September 18, 2019. We reported study findings in accordance with the Consolidated Standards of Reporting Trials (CONSORT) for cRCTs [24].
Setting and site selection at the cluster level
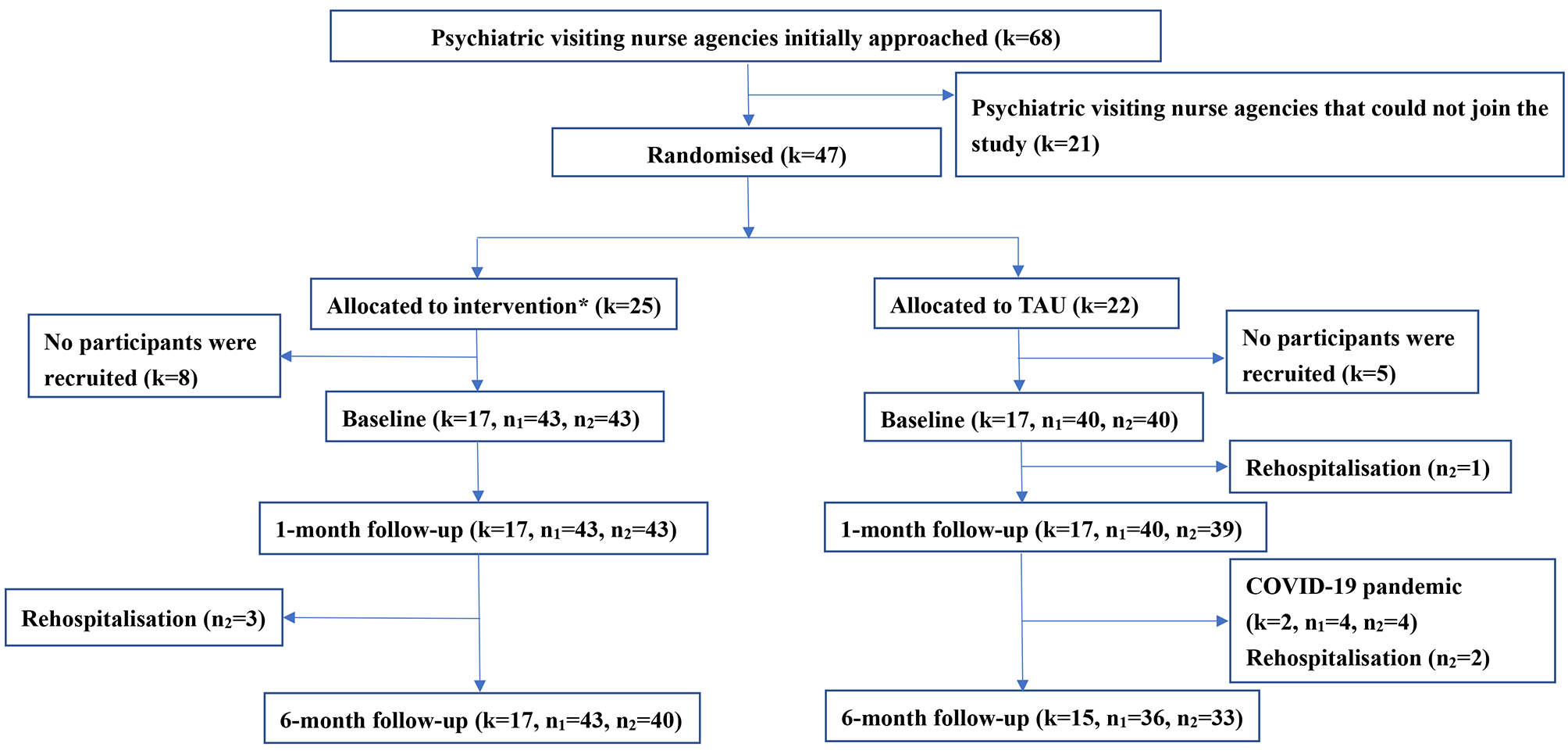
The first author (NY) approached 68 psychiatric visiting nurse agencies in 4 prefectures in Japan (Tokyo, Saitama, Kanagawa, and Chiba) managed by one organisation. Forty-seven visiting nurse agencies agreed to participate in the study.
The inclusion criterion for psychiatric visiting nurse agencies was that psychiatric visiting nurses provided services mostly to psychiatric patients rather than elderly people or those with physical diseases. In each agency, psychiatric visiting nurses must care for at least two people with schizophrenia who live with their family. There were no exclusion criteria at the cluster level.
Randomisation at the cluster level
We randomly allocated psychiatric visiting nurse agencies into the BFP programme group (intervention group) or the treatment as usual (TAU) group. Randomization of clusters was performed prior to the collection of baseline data, and the results of the randomization were conveyed to each psychiatric visiting nurse agencies after the completion of participant recruitment. It was also stratified by the median of the average caseload of psychiatric visiting nurses in each agency because the service quality of a psychiatric visiting nurse is affected by caseload [25]. Family support is unlikely to be provided when a psychiatric visiting nurse has a high caseload. A researcher (HT) in the statistics department who was not involved in the study protocol development process created a random sequence table. Another researcher (SY) who was not involved in the intervention or analysis conducted the randomisation and informed each psychiatric visiting nurse agency of the randomisation results after the recruitment procedure at the individual level. The primary investigator (NY) was blinded through the entire randomisation process. Further information about the randomisation process was provided in the study protocol [23].
Participant eligibility criteria and recruitment procedure at the individual level
The inclusion criteria for a family caregiver of a person with schizophrenia were as follows: (1) primary caregiver; (2) age over 20 years; (3) family member of a person with schizophrenia such as a parent, sibling, spouse, or child; and (4) living with the person with schizophrenia. There were no exclusion criteria for caregivers. The inclusion criteria for people with schizophrenia were as follows: (1) diagnosis of schizophrenia based on the International Statistical Classification of Diseases and Related Health Problems, 10th revision and (2) receiving services from psychiatric visiting nurses.
During the recruitment procedure at the individual level, we listed all potential participants (family caregivers of people with schizophrenia and people with schizophrenia) at each agency. Second, we created a randomly ordered list using a random number generator in the Stata statistical software program, version 15, in order to avoid selection bias at the individual level. Third, each psychiatric visiting nurse who attended a lecture on study design and ethical considerations recruited participants according to the randomly ordered list until five participants were recruited. Psychiatric visiting nurses also obtained written informed consent from people with schizophrenia and their caregivers. Only participants who voluntarily agreed to participate in the study were included.
The deadline for participant registration submitted to the ethics committee was October 31, 2020. In Japan, a state of emergency was declared after April 2020, which led to restrictions on the number of visits and duration of psychiatric visiting nurses’ visits from the perspective of infectious disease prevention. Consequently, conducting family psychoeducation, which requires longer visit times than usual, became a burden for both the participating facilities and the patients or their families, making further recruitment challenging.
Intervention programme
This intervention program was a single-family intervention conducted by psychiatric visiting nurses that was based on the Family Intervention and Support in Schizophrenia: A Manual on Family Intervention for the Mental Health Professional [26]. Based on the concept of coproduction and patient and public involvement (PPI), we created this program through discussions and collaborations among members of the Family Association of Schizophrenia, psychiatric visiting nurses, FPE experts, psychiatrists, psychiatric nurses, clinical psychologists, and mental health social workers [27].
The program consisted of four sessions lasting 60 min each, which was completed over 1 month. Attendance of at least one session was required. In Session I, general knowledge about schizophrenia was covered, including its definition, causes, symptoms, and prognosis. The definition and causes were emphasized using the stress-vulnerability model and dopamine hypothesis, highlighting that schizophrenia is a brain disease that can affect anyone. It was important to explain biological causes, as some families believe that familial relationships are the cause of schizophrenia. Regarding symptoms, the session emphasized the challenges that individuals face in maintaining their typical way of life due to psychiatric symptoms. The course of the illness, including the prodromal, acute, and recovery phases, was explained, detailing the characteristics and management strategies for each phase. The prognosis discussed how schizophrenia is not necessarily a condition with a poor outcome. Medication therapy was addressed, acknowledging the difficulties of daily medication adherence, and discussing the necessity and safety of pharmacological treatment. The side effects of antipsychotic medications were explained using illustrations. The session concluded with an explanation of psychosocial treatments such as psychoeducation and daycare, and a knowledge check quiz was conducted. In Session II, various family concerns and problem-solving techniques were addressed. The session covered responses to hallucinations and delusions, signs of relapse, creating a crisis plan, managing worsening conditions, dealing with a family member staying indoors, reluctance to take medication, potential and occurring violence, and suspected self-harm or suicidal behaviors. Finally, problem-solving techniques were taught, and families practiced solving everyday caregiving issues using these methods. Session III dealt with engagement and communication training with the affected individual. It focused on understanding the patient’s feelings, Expressed Emotion (EE) theory, basic communication knowledge and skills, and methods to enhance resilience. The importance of showing understanding for the individual’s pessimistic views about their future and their difficulties was emphasized. EE theory also highlighted that it is understandable for families to exhibit high EE levels, and explained how changing the way families interact could potentially alter the individual’s symptoms and condition. Additionally, the session included practicing conversation using hypothetical case scenarios to think about better communication methods. Session IV focused on family recovery. It addressed the importance of family recovery, the significance of families living their own lives, considerations for physical and mental health, strategies for managing stress without exhaustion, experiences, and messages from members of a schizophrenia family association, and available community resources. This session emphasized the importance of both the individual and family having their own lifestyles and goals, encouraged families not to devote themselves solely to caregiving but to utilize various social resources to pursue their own lives. It also aimed to improve family members’ physical and mental health through knowledge of self-care and stress management. Experiences from three family association members were shared to help families understand that they are not alone in their struggles, aiming to alleviate their sadness and despair. Lastly, the session discussed community resources available and the importance of connecting with multiple supporters. We also described the development and contents in greater detail in the study protocol [23].
Training and program adherence
The intervention team of psychiatric visiting nurses was provided with a 1-day group lecture before the intervention, which consisted of three parts. First, family caregivers of people with schizophrenia talked about their life problems and what they wanted psychiatric visiting nurses to do. Second, basic communication training was performed through role-playing. Third, the primary investigator (NY) equipped psychiatric visiting nurses with basic knowledge about FPE and explained the contents of this intervention tool and the points that the primary investigator wanted to emphasise.
With regard to program adherence, we created a checklist to confirm the date the programme was implemented and how many sessions psychiatric visiting nurses were actually able to conduct with participants. The checklist was self-reported by psychiatric visiting nurses at the end of each session.
Treatment as usual (TAU) group
Family caregivers of people with schizophrenia in the control group received usual care from psychiatric visiting nurses. They did not receive any type of psychoeducation or supportive therapy.
Outcomes
The following outcome measures were assessed at baseline prior to the intervention (T1), immediately after the completion of the intervention (1-month follow-up, T2), and 6 months after the baseline assessment (6-month follow-up, T3).
Primary outcome for caregiversZarit burden interview (ZBI-22)
ZBI-22 was used for measuring caregiver burden. It consists of 22 items scored on a 5-point Likert scale from 0 (never) to 4 (nearly always) [28]. The total score ranges from 0 to 88, with higher scores indicating higher burden. Cut-off points are as following: 0–21, little or no burden; 21–40, mild to moderate burden; 41–60, moderate to severe burden; and 61–88, severe burden. The Japanese version of ZBI-22 has high test–retest reproducibility and internal consistency [29]. Construct validity has also been confirmed [30].
Secondary outcome for caregiversKessler psychological distress scale (K6)
K6 was used to measure sub-clinical depression and anxiety disorders as part of a self-administered questionnaire, which consists of six items answered on a five-point Likert scale. Scores range from 0 to 24, with higher scores representing higher degrees of sub-clinical depression and anxiety disorder. The Japanese version has essentially equivalent screening performance as the original English version [30].
General self-efficacy scale (GSES)
GSES is a measure of self-efficacy in daily living, which includes 16 items with dichotomous questions [31]. In general, higher scores indicate better self-efficacy [31]. GSES has high test–retest reproducibility and internal consistency [31]. Construct validity has also been confirmed [31].
WHO-five well-being index (WHO-5)
WHO-5 was used to measure subjective well-being or quality of life based on positive mood (good spirits and relaxation), vitality (being active and waking up fresh and rested), and general interest (being interested in things). The scale consists of five items rated on a six-point Likert scale. Higher scores mean higher well-being. The Japanese version of WHO-5 has adequate internal consistency [32]. External concurrent validity and external discriminatory validity have also been confirmed in a previous study [32].
Knowledge of illness and drug inventory (KIDI)
KIDI was used to assess the knowledge regarding mental illness and the effects of medications on mental illness [33]. There were 2 sub-scales: 10 items assessing knowledge of mental illness and the remaining items assessing knowledge of the effects of antipsychotic drugs. This inventory consists of a self-reported inventory where respondents were asked to select the correct answer from three choices, with higher scores representing greater knowledge.
Secondary outcomes in people with schizophreniaBehaviour and symptom identification scale (BASIS-32)
BASIS-32 has been used to measure mental health. It includes 32 items on a 5-point Likert scale, where 0 indicates no difficulties and 4 indicates severe difficulties. The scale measured five factors: (1) relation to self and others (seven items); (2) depression/anxiety (six items); (3) everyday life and role functioning (nine items); (4) impulsive and addictive behaviour (six items); and (5) psychosis (four items). Internal consistency and construct validity of the Japanese version of BASIS-32 have been demonstrated [34]. For overall symptom severity, we used the average score of the 32 items.
WHO-five well-being index (WHO-5)
WHO-5 was used to measure subjective quality of life based on positive mood (good spirits and relaxation), vitality (being active and waking up fresh and rested), and general interest (being interested in things). It consisted of five items rated on a six-point Likert scale. Higher scores mean higher well-being. The Japanese version of WHO-5 [32] had adequate internal consistency. It had been confirmed to have external concurrent validity and external discriminatory validity.
Hospitalisation by 6-month follow-up
We created a self-reported measure for hospitalisation that included a dichotomous variable about whether a person with schizophrenia had been hospitalised during the past 6 months. The participating family caregiver reported this measure at the 6-month follow-up. If the person with schizophrenia had been hospitalised, the caregiver reported the date of admission.
Sample size calculation
We calculated sample size according to the CONSORT guidelines for cRCTs [24], taking into account intra-class correlations (ICCs). The effect size of the BFP programme for individual caregiver burden was estimated based on a previous pre–post test [35]. The pre–post-test concluded that the standardised mean difference (d) of the BFP programme on caregiver burden was 0.46. Sample size was estimated as 76 in each arm based on an alpha error probability of 0.05 and power (1 − β) of 0.80, using G*Power version 3.1.9.2 [36, 37]. For cRCTs, this value should be multiplied by the design effect (1+[m − 1]ρ), where m is the average cluster size and ρ is the ICC [38]. The estimated ICC for the primary outcome in this study was set to 0.05 and the average number of caregivers per cluster was set at 5. Assuming an attrition rate of 20%, the required sample size is 110 caregivers in each arm. Thus, at least 44 visiting nurse agencies should be recruited.
Statistical analyses
All analyses were conducted in accordance with intention to treat (ITT) model. The effect of the intervention on primary and secondary outcomes was estimated using linear mixed models, which allowed for missing data to be taken into account within the statistical model. In this study, a three-level model was used, with repeated measures nested in participants and participants nested in clusters. Time (baseline, 1-month follow-up, 6-month follow-up) was considered level 1, individual caregivers were considered level 2, and clusters (psychiatric visiting nurse agencies) were considered level 3. For fixed effects, condition (BFP programme versus TAU), time, and the two-way interaction effect of condition by time were included. Models were adjusted for baseline differences in caregiver socio-demographics such as age, gender, education, household income, family relationship to the person with schizophrenia, length of caregiving, and length of psychiatric visiting nurse system use. Subgroup analyses were conducted separately among respondents who had mild or higher caregiver burden (ZBI-22 score of 21 or higher) at baseline. A p-value of less than 0.05 was considered statistically significant. SPSS (Windows version 27) was used for statistical analysis.
Changes to the protocol
Two changes for statistical analyses were made to the registered protocol [24]. One was analysis for rehospitalisation. We had intended to conduct Cox proportional hazards regression models with multiple levels for the dichotomous question of hospitalisation by 6-month follow-up. However, we were unable to perform the analysis because the date of admission was not available for one participant. Therefore, the number of hospitalisations by 6-month follow-up was just described and the chi-square test was conducted. The other change was a subgroup analysis to clarify the effect of the BFP programme based on the existence of caregiver burden (ZBI-22 score of 21 or higher). We determined that study participants had relatively a low level of caregiver burden compared with participants of previous studies [17,18,19] and the effect of the BFP programme may have been weakened by the floor effect.


留言 (0)