
記住我



The use of AUS as a treatment for SUI is increasing in both males and females. According to the 2023 AMS 800 consensus statement by Chung et al., female AUS insertion is still considered an uncommon procedure, however, is recommended in female patients with urodynamically proven detrusor underactivity and concomitant ISD. Use of the device is contraindicated in patients with previous pelvic radiation therapy, active urosepsis or cellulitis [8••].
Peyronnet et al. described total use of the device increasing by 8.8% from 2012 to 2017. From 2015 in the female population however there was an increase in the number of implants by 28.9% [7•].
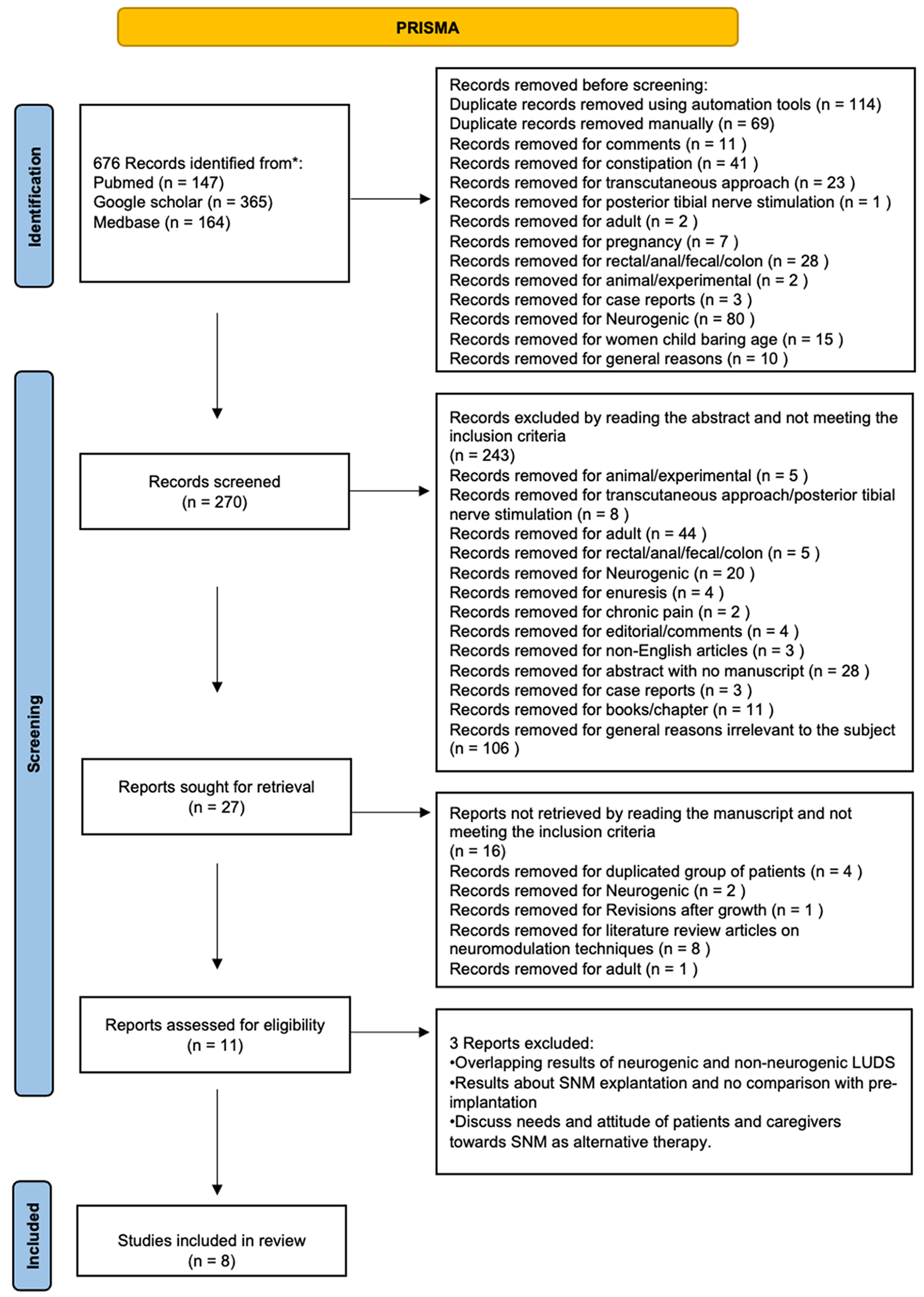
Barakat et al. published a systematic review to assess the results and complications of female AUS and concluded that implantation of AUS in women with SUI is an effective treatment option for patients who have failed first line therapies [9]. A meta-analysis performed by Reus et al. showed a “no pad rate” that ranged between 42 and 86% across all studies included, with a post-surgical adverse event rate reported between 2 and 54%. The wide range of outcome heterogeneity is due to variations in surgical technique, the indiscriminate inclusion of neurogenic and non-neurogenic patients, and a high percentage of AUS patients having one or more previous operation for incontinence [10].
A 2023 study conducted in France compared the long-term device survival of the AMS 800 in men and women. 107 women were compared to 316 men, who had all undergone AUS insertion for non-neurogenic SUI in a single centre between 2000 and 2013. During a median follow up of 5.1 years it was seen that 13.9% of men and 11.2% of women required explantation, and 26.9% of men and 26.1% of women required revision surgery. In the first six months of implantation, there were zero women requiring revision surgery, compared to 13 men. As demonstrated by this study, the AUS had better long-term survival in women, recognising that results may have been affected by varied surgical approach [11].
Phe et al. conducted a long-term study on female patients with SUI treated with an AUS between 1984 and 2011. A cohort of 26 patients were reviewed retrospectively. Of the patients, 23 underwent open device insertion and 3 underwent laparoscopic insertion, with 24 pumps inserted in the right labia. 58% of patients had previously undergone surgical intervention for SUI including Burch colposuspension, retropubic tension free vaginal tape and one prior augmentation cystoplasty. A median follow up of 7.5 years saw 57.7% (15/26) of patients still using the original device, with revision surgery occurring in 35.2% (9/26). At the time of final follow up 71.4% of patients were continent, requiring no pads. This study may be adversely affected by the length of his treatment period as modern advancements and surgical techniques may result in better outcomes in newer studies [12].
A systematic review and meta-analysis were performed in 2022, looking at 308 articles with an aim to determine the complication rate of AUS, exclusively in female patients with SUI, which resulted from ISD. The most common complications included atrophy, necrosis, erosion, infection, mechanical failure, reconstructive surgery and leak. These complications were subdivided per the surgical implantation method of open and minimally invasive. The study determined that the minimally invasive approach significantly decreased the incidence of mechanical failure (0.53% vs 8.22%) and the need for reconstructive surgery (3.72% vs 14.2%), however significantly increased the risk of infection (6.38% vs 3.2%). All revisions were due to the mechanical failure of the pump, the balloon, the cuff or the connections [13].
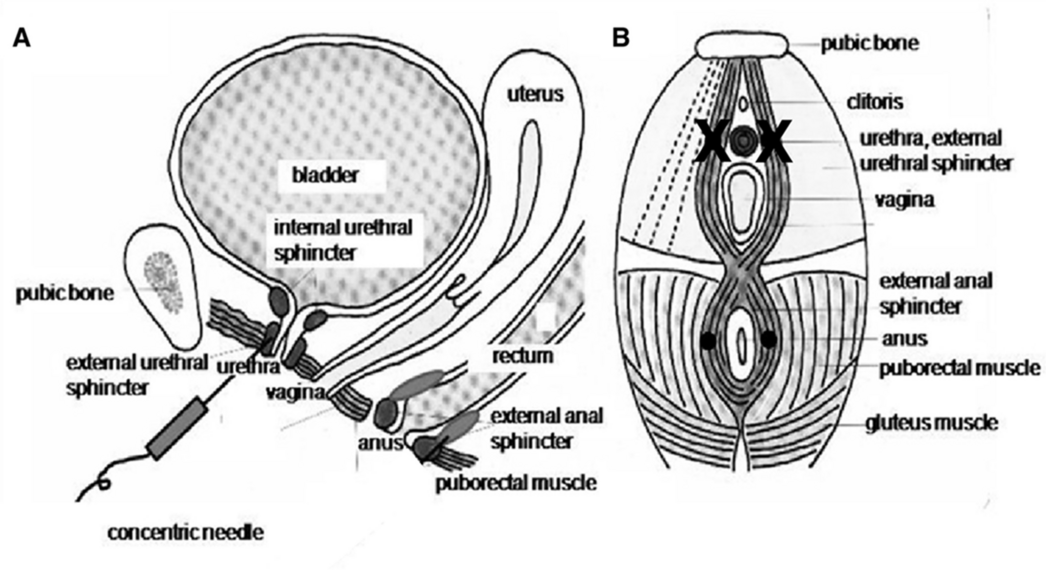
Surgical TechniquesIn terms of surgical approach, the implantation can be performed open, transvaginally, laparoscopic, and robot-assisted, placing the cuff around the bladder neck, pressure regulated balloon (PRB) in the lower abdomen, and pump in the labia majora. The 2023 consensus by Chung et al. recommend a retropubic approach to allow adequate AUS cuff placement at the bladder neck with a 14fr or 16fr foley catheter to facilitate urethra palpation, particularly in patients with a history of pelvic trauma, diabetes or previous urethral surgery. Intraoperative cystoscopy is also encouraged to be a routine part of the procedure to ensure no urethral injury, however a peri-catheter leak test may be used as an alternative if necessary [8••]. The main steps of the robotic approach are illustrated in Figs. 1, 2, 3 and 4 (Figures courtesy of Dr. Vincent Tse).
Fig. 1
Dissection of the plane between the vagina and bladder neck, during a robotic approach from an anterior aspect (all images courtesy of Dr. V. Tse)
Fig. 2
Sizer used to determine the bladder neck cuff size, which often ranges between 6.5–7.5cm
Fig. 3
Cuff secured and pressure regulating balloon placed and covered with intraperitoneal fat that have been secured
Fig. 4
Extraperitonealisation of the device at the end of the robotic procedure
Peyronnet et al. performed the first multicentre retrospective review in 2019 of 49 female patients who underwent robotic AUS implantation between 2012 and 2017. The outcomes of this study revealed a 16.3% complication rate but only 4.1% were Clavien-Dindo grade 3 or higher. There was a 2.1% erosion rate, with 6.1% of patients needing revision. 81.6% of patients were fully continent, 12.2% had improved continence and 6.1% had unchanged continence. The same study compared the robotic approach and outcomes in male and female patients; 149 patients were included, 91 male and 58 female. There was a significantly shorter operating time for male patients (137.4 min vs 179.4 min) with comparable complication rates (20.8% vs 27.6%), however the female group was found to have remarkably higher rates of complete continence at 3 months, with zero pads used in 76.4% of females and 42.3% of males [14•].
Gondrand-Tellier et al. used a posterior approach to minimise blind dissection and thus the risk of bladder or vaginal injury. The single surgeon study included 8 patients who underwent robot assisted AUS insertion between 2017 and 2018. Of the cohort, 62.5% had previously undergone pelvic surgery for SUI or vaginal prolapse. The approach resulted in no bladder or vaginal injuries. This study is limited by a small cohort, which may not provide an accurate cross section of patients who may undergo this procedure [15]. To compare a larger cohort, Orchoa Vargas et al. utilised this technique on 40 patients from 2017 to 2022, noting the challenge of ensuring adequate vesicovaginal dissection low enough to place the cuff. 87.5% of patients were able to be completed using this technique, with 2 patients needing conversion to open, and 3 patients needing modifications to surgical approach. 97.5% of patients had previous SUI surgery. There were bladder injuries sustained in 23% of cases, vaginal injury in 14% of cases and bladder neck injury in 3.5% of cases. 5.7% of the devices were removed and 5.7% of patients needed revision surgery. There was a continence rate of 94% [16].
Haudebert et al. presented a case report at EAU 2023 about a robotic extraperitoneal approach in a female patient with spina bifida and a surgical history of a supra-trigonal cystectomy and augmentation cystoplasty in 1996. She had additionally had a history of an enteric fistula secondary to an oophorectomy and had previously had a pubovaginal sling inserted to treat her SUI which had no longer remained effective to maintain continence. This approach was successful and the patient was fully continent at the 6 month follow up [17]. While this is evidence of a successful implantation technique in a single complicated patient, there has only been a relatively short follow up period within which failure and longer term complications can occur.
Other surgical techniques utilised include a laparoscopic approach with a posterior dissection used in 49 female patients, the majority of which had spinal cord injuries. There was a bladder injury rate of 18.4%, a 10.8% explantation rate and a 84% rate of improved or complete continence which is comparable to robotic methods [18].
ContraindicationsThe AUS is contraindicated in patients with recurrent UTI’s, anatomical abnormalities such as urethral diverticulae or recurrent stricture disease, poor bladder compliance, acontractile detrusor or patients with reduced manual dexterity or cognitive dysfunction. Recurrent renal or bladder stone disease and vesicouretric reflux are relative contraindications to the device, and prior radiation therapy has been associated with high rates of intraoperative on post-operative complications in some studies [19].
With respect to women of child-bearing age, it is important to note that they are at greater risk of cuff erosion during vaginal delivery. Deactivation during labor and delivery is necessary, along with recommendations against future pregnancy, opting for elective caesarean section, and deactivation of the device during the final trimester in order to minimize the risk of erosion [20].
留言 (0)