
記住我

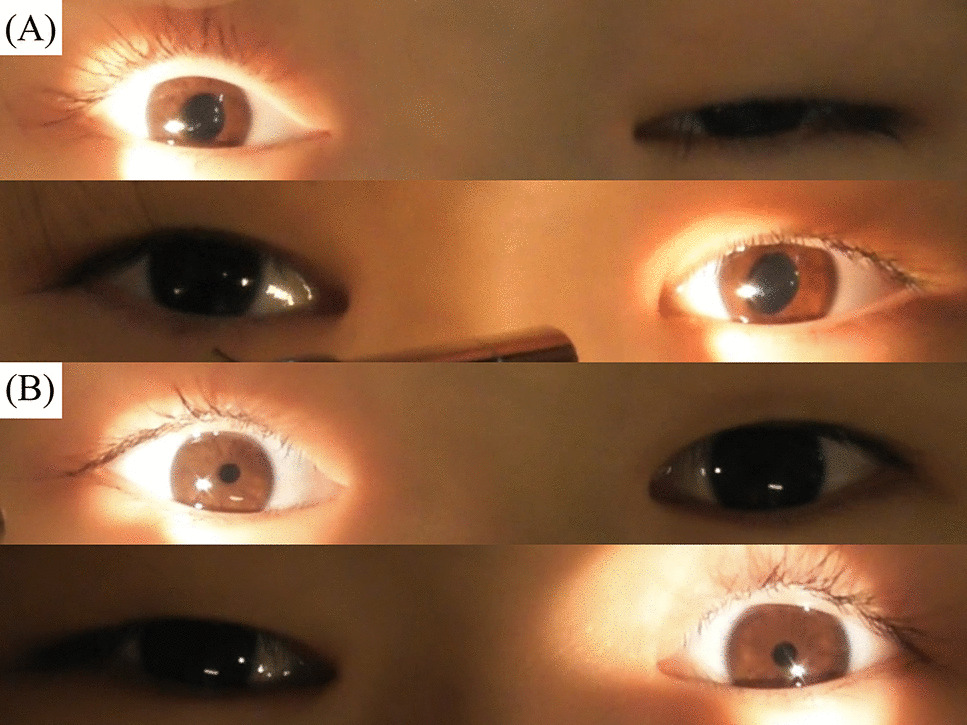
A previously healthy 6-y-old boy suddenly developed paralytic ileus, then gradually presented with photophobia, paresthesia, and irritability over the next two months. No infection or immunization preceded the onset. Physical examination revealed areflexia in the lower legs and various autonomic symptoms, such as pupillary dysfunction (Fig. 1A), tachycardia, hypertension, orthostatic syncope, constipation, and hypohidrosis. He had severe paroxysmal coughing that often led to vomiting. The anti-ganglionic acetylcholine receptor, paraneoplastic and anti-nuclear antibodies were negative. The brain and spine magnetic resonance imaging were normal. Cerebrospinal fluid analysis showed mildly elevated protein concentration. Nerve conduction studies revealed slightly reduced sensory nerve action potential amplitudes. 0.125% dilute pilocarpine test showed markedly prolonged pupil constriction (Fig. 1B). Finally, he was diagnosed with acute autonomic and sensory neuropathy (AASN). He required gastrostomy for feeding intolerance. Methylprednisolone pulse therapy was partially effective for paroxysmal cough and vomiting, whereas intravenous immunoglobulin therapy was not. His symptoms gradually improved over several months, with complete recovery twenty months after onset.
Fig. 1
A Oval pupils, bilateral mydriasis and loss of light reflex. B Hypersensitivity to 0.125% dilute pilocarpine
AASN is characterized by an acute development of autonomic and sensory neuropathy without motor impairment [1]. Pupillary disorders and hypersensitivity to pilocarpine in AASN patients have been reported as representative symptoms [2], which might be explained by functional parasympathetic denervation due to a synaptic transmission blockade in the ciliary ganglia [3]. AASN is rarely identified in children, challenging its diagnosis. These characteristic pupillary abnormalities help diagnose autonomic disorders, including AASN.
留言 (0)