In the present study, authors observed that the implementation of proactive perinatal care, beginning from intensive prenatal care for high-risk mothers, continuing proactive neonatal resuscitation starting at the DR, and minimizing handling by reducing unnecessary sampling and tests in NICU, led to improvements in survival rates as well as reductions in neonatal morbidities among PPIs. First, the mortality rate decreased significantly, dropping from 54.4% to 24.3% after the implementation of proactive perinatal care for PPIs. Proactive perinatal care emerged as an independent factor contributing to this reduction in the mortality rate. Second, the incidence of neonatal morbidities or death, especially severe brain injury or death, significantly decreased, which could be considered an indicator of improved long-term neurological outcomes.
The survival of PPIs born at 220/7 to 246/7 wk of gestation increased from 30% (424/1391) to 36% (487/1348) from 2000–2003 to 2008–2011 [14]. However, these outcomes differ depending on the treatment policy. PPIs may receive comfort-focused or survival-focused care following delivery. The goal of comfort care is to provide comprehensive health care services to avoid painful stimuli or maternal-infant separation to mother-infant dyads with life-limiting conditions [15]. Meanwhile, for survival care, health care professionals provide maximal resuscitation to PPIs. These variations in neonatal care have a substantial impact on the survival and morbidities of PPIs. Clearly, more active perinatal care has resulted in higher survival rates among PPIs. In Western Europe, routine provision of proactive treatment is not standard care. The reported survival rates were only 0% in the EPICURE study in England [16] and 2% in the EPIPAGE-2 study in France [17] for infants born at 22 wk of gestation. In contrast, with proactive treatment in highly specialized centers, survival rates above 50% can be routinely achieved [18]. Furthermore, several studies in which proactive treatment was provided to all mother–infant dyads at risk for periviable delivery have provided evidence for these significantly improved statistics [18,19,20,21,22].
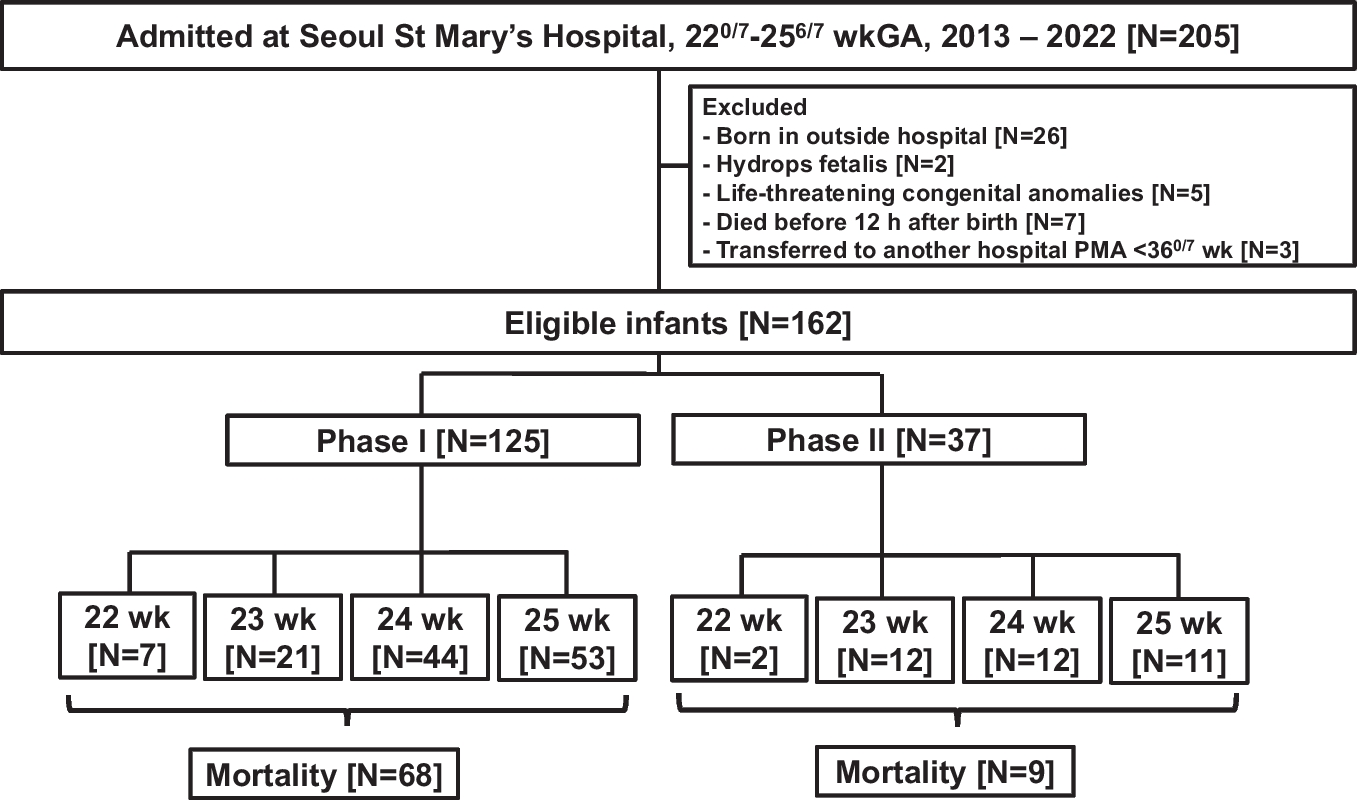
It is worth to note that the survival rate in present study increased dramatically after the provision of proactive treatment—75.7% in phase II—which was even greater than that in the US or Sweden. Logistic regression analyses revealed that initial conditions such as GA at birth, air leak syndrome, and massive pulmonary hemorrhage were independently associated with mortality of PPIs, which is consistent with the findings of previous studies [23, 24]. Each additional week for GA resulted in a 0.9-fold decrease in the risk of mortality. Moreover, neonatal conditions immediately after birth were associated with a greater mortality risk: 4.958 times and 4.944 times greater for patients with air leak syndrome and massive pulmonary hemorrhage, respectively. Furthermore, birth during phase II decreased the risk of mortality by 0.324 times. These findings proved again that proactive perinatal care for PPIs confers survival benefits.
Higher survival rates were achieved in the phase II than that of recent results based on nationwide South Korea’s registry [25], and the survival rate in present study reached as high as that of US and Sweden [19, 20]. The special characteristic of the present proactive perinatal care protocol is that three aspects of effort were made together: intensive prenatal care for high-risk mothers, proactive resuscitation for PPIs immediately after birth, and minimal handling with maximal observation after admission to the NICU. Prenatally, the administration of ACS significantly increased during phase II. In a study from the NICHD, Neonatal Research Network, high mortality was reported for PPIs without maternal ACS administration [6]. Since the experienced attending neonatologist efficiently led the neonatal resuscitation before the baby's condition deteriorated, the initial body temperature at admission also significantly increased in phase II, and the proportion of neonates who needed epinephrine during resuscitation significantly decreased with the new protocols. These findings supported that authors’ center’s multidisciplinary approach unquestionably contributed to the improved survival of PPIs and a reduction in overall morbidities.
A recent study reported that infants who received active perinatal care had no or mild long-term neurodevelopmental impairment [14, 18, 26]. Minimal handling, which is implemented for neuroprotective purposes, reduces stress and can enhance the potential for neuroplasticity in PPIs, thereby promoting healthier brain development. Although the authors did not analyze long-term outcomes, morbidities other than BPD decreased in phase II. In particular, severe brain injury or death significantly decreased from 83.2% to 51.4% with time, which could be considered an indicator of improved long-term neurological outcomes.
The main strength of the current study is uniqueness of the protocol, as it considered intensive obstetric care, proactive perinatal care and minimal handling together. However, this study had several limitations. First, this was a retrospective study design, which might be unable to fully confirm the examined relationships. Second, the study group had a relatively small sample size. Third, there was a consistent decreasing trend in the number of births in authors’ center, especially after the onset of Coronavirus disease 2019 pandemic, when the total number of births decreased in South Korea.


留言 (0)