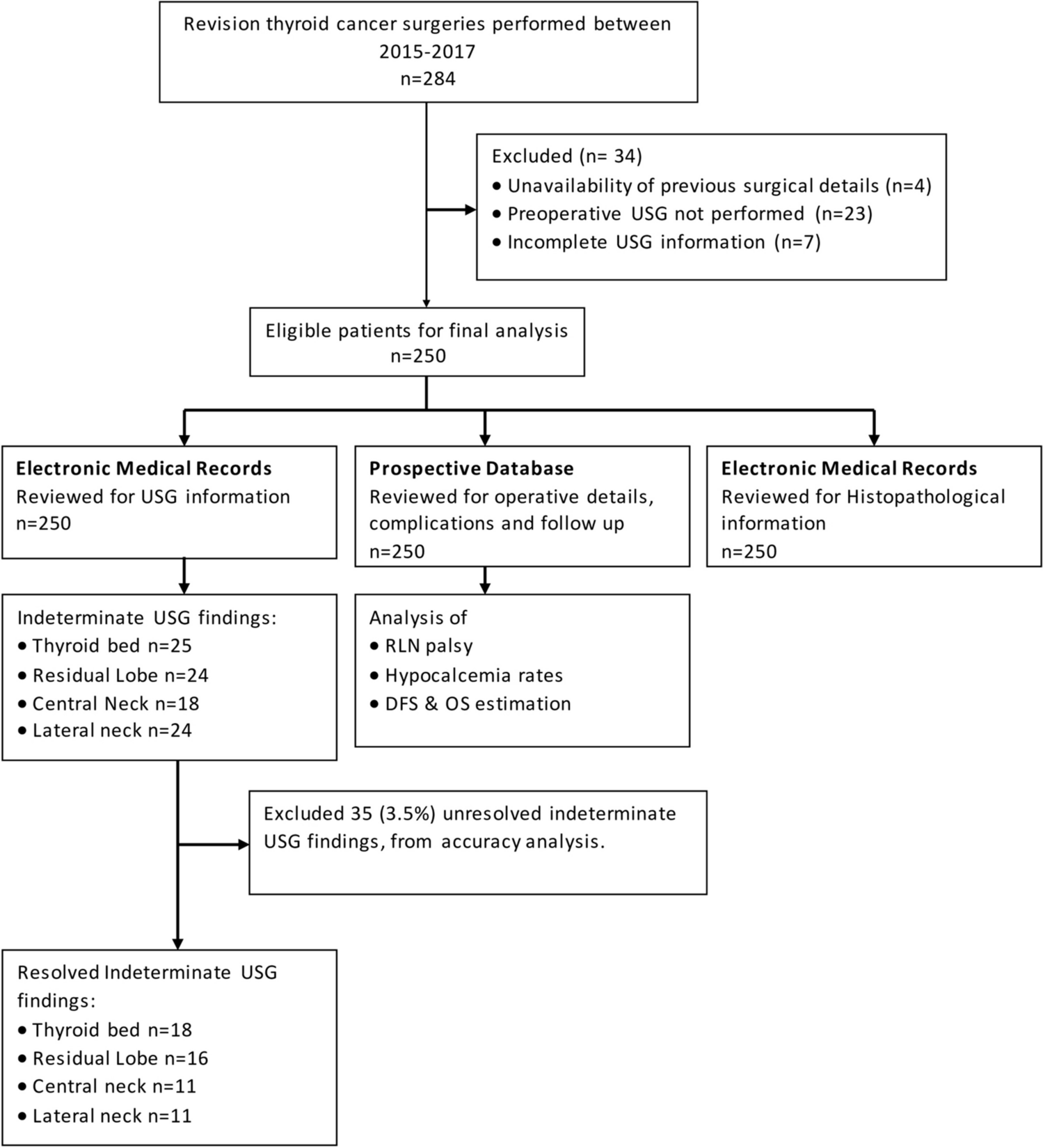
After obtaining Institutional Review Board approval, a retrospective analysis of all thyroid cancer patients undergoing revision surgery from 2015 to 2017 was performed. Cases were identified from a prospectively maintained institutional surgical database. Patients undergoing resurgery for suspected recurrence in the residual thyroid/thyroid bed/central or lateral nodal compartments, patients undergoing completion surgery for previously operated hemithyroidectomies, and incomplete surgeries in high-risk patients were included. Patients who had undergone surgery for benign thyroid diseases, patients with incomplete operative details, nonavailability of preoperative USG, and those with incomplete preoperative USG findings were excluded from the analysis. Previous operative information, findings of neck sonography done before reoperation, operative procedure, and histopathological findings were reviewed from the prospective database and from hospital electronic medical records.
Imaging
USG was performed using high-frequency linear array transducers of 7-13 MHz (GE LOGIQ™ E9). At our institution, USGs are performed and interpreted by speciality trained head and neck radiologists. These reports were evaluated and USGs of patients with indeterminate findings were rereviewed by SA#.
Image Interpretation
USG findings were classified into four subsections: thyroid bed, residual lobe, central compartment nodes, and lateral compartment nodes.
Thyroid bed was defined as an inverted triangular area with hyperechoic fibrofatty tissue with boundaries as follows: lateral boundary by the carotid arteries, medially by the proximal trachea, ventrally by the strap muscles, craniocaudally from the lower half of the thyroid cartilage to the thoracic inlet.
Residual lobe: The remaining thyroid lobe in patients who had undergone prior hemithyroidectomy/isthmectomy.
Lateral compartment nodes: Neck nodes were divided into level II to level V according to the imaging based nodal classification [7].
Central compartment was defined as the area between the medial borders of both common carotid arteries, bounded superiorly by the inferior border of hyoid done and inferiorly by the superior border of the manubrium. Platysma, trachea, and prevertebral space were the anterior, posteromedial, and posterolateral limits.
Lesions in the thyroid bed with sonographic features like hypoechogenicity, marginal irregularity or spiculation, microcalcification, and a taller-than-wide shape were classified as suspicious in nature. Lateral and central compartment nodes which are well-defined, coffee bean-shaped, and homogeneous with preserved echogenic fatty hilum were classified as reactive lymphoid hyperplasia. Lateral and central compartment nodes with sonographic features like round shape, absence of an echogenic hilum, microcalcifications, hyperechogenicity, cystic change, and peripheral flow on color doppler were classified as metastatic nodes.
USG reports for patients included in the study were reviewed, and all findings were classified as suspicious, benign, or indeterminate. In the case of USG reports showing indeterminate findings, the images were reviewed by SA. Individuals with unresolvable USG findings were documented as indeterminate. Indeterminate findings were excluded from the accuracy analysis.
As per the American Association of Clinical Endocrinologists (AACE) guidelines, postoperatively, patients with corrected serum calcium (Ca+2) levels of < 8.6 mg/dl were considered as having temporary hypoparathyroidism [8]. Individuals with low serum Ca+2 levels for a duration > 6 months after surgery or those requiring Ca+2 supplementation to maintain optimal serum Ca+2 levels beyond 6 months were considered as permanently hypoparathyroid.
Follow-up was calculated from the date of reoperation to the last date of follow-up.
Statistical Analysis
Sensitivity, specificity, positive predictive value, and negative predictive value were calculated using histopathology as the gold standard for the four subsections within the neck. Survival analysis was performed using the Kaplan–Meier curves. SPSS (Statistical Package for the Social Sciences) version 23 was used for data collection and analysis.






留言 (0)