Study population
This study is embedded in the Generation R Study, a multiethnic population-based prospective cohort from fetal life onwards. The study is designed to identify early environmental and genetic determinants of growth, development, and health. The cohort has previously been described in detail [14, 15]. Briefly, all pregnant women who resided in Rotterdam at the time of childbirth and with a due date between April 2002 and January 2006 were invited to participate. Enrollment was aimed in early pregnancy (gestational age < 18 weeks), but was possible until birth of the child. In total, 9778 (response rate 61%) women were enrolled in Generation R, of whom 9621 were included in the analyses, see paragraph below. The study has been approved by the Medical Ethics Committee of Erasmus MC in Rotterdam, the Netherlands, and is conducted in accordance with the Declaration of Helsinki of the World Medical Association. Written informed consent was obtained from all parents and children (if older than 12). This project was pre-registered at Open Science Framework (https://doi.org/10.17605/OSF.IO/G86SF).
MeasurementsUnintended pregnancy
Pregnancy intention was measured using a self-report questionnaire at inclusion of the study. Women reported whether their pregnancy was planned or not. This variable was compared with pre-pregnancy folic acid use and contraceptive use at conception. We excluded those who reported both an unplanned pregnancy and pre-pregnancy folic acid intake (n = 104) and those who reported a planned pregnancy and contraceptive use at conception (n = 173), leaving n = 9621 participants for analyses (n = 1765 participants with missing data on pregnancy intention were imputed). In case of an unplanned pregnancy, women reported how they felt about the pregnancy using the following four answering categories: “pleased from the start”; “initially mixed feelings”; “still mixed feelings”; or “mostly unhappy about the pregnancy”. Few women reported having “still mixed feelings” or “mostly unhappy”, which we combined into prolonged ambivalent feelings. Pregnancy intention was categorized into “planned”, “unplanned and wanted from the start”, “unplanned and initially ambivalent feelings”, and “unplanned and prolonged ambivalent feelings”.
Child internalizing and externalizing problem behavior
The validated Child Behavior Checklist (CBCL/1½–5 and CBCL/6–18) was completed by the main caregiver of the child at ages of 1.5, 3, 6, 9 and 13 years [16, 17]. The CBCL consists of 99 items (CBCL/1½–5) or 118 items (CBCL/6–18) and assesses behavioral and emotional problems in the preceding 2 (CBCL/1½–5) or 6 (CBCL/6–18) months. Items of the CBCL/1½–5 and CBCL/6–18 were comparable and scored on a 3-point Likert scale (0 = not true, 1 = somewhat or sometimes true, and 2 = very true or often true). Mean scale scores for internalizing (anxious/depressed, withdrawn/depressed and somatic complaints) and externalizing (rule-breaking behavior, and aggressive behavior) behavior were computed and converted to standardized T-scores per wave. Cronbach’s alpha at the different time points were calculated and are shown in supplemental Table 1. Sensitivity analyses were performed with similar scores, but based on self-report by the children. At age 9 years, children were asked to complete the Brief Problem Monitor which is a validated, 19-item abbreviated version of the Youth Self Report (YSR) [18]. At age 13 years, children completed the full YSR containing 110 items [19]. For post-hoc analyses, internalizing and externalizing problem behavior, as measured using the CBCL, were dichotomized based on borderline clinical cutoffs as indicated by a T score of 60 or higher (equivalent to the 84th percentile) as recommended by Achenbach et al. (2000 and 2001) [16, 17]. At ages 1.5, 3 and 6 years, borderline clinical cases were defined as sumscores > 12 for internalizing and > 18 for externalizing behavior. At age 9, borderline clinical cases were defined as sumscores > 8 for internalizling behavior in boys and > 10 in girls, and > 11 for externalizing behavior in boys and girls. At age 13, borderline clinical cases were defined as sumscores > 10 for internalizing behavior in boys, and > 11 in girls, and > 13 for externalzing behavior in boys, and > 11 in girls.
Postpartum psychiatric symptoms
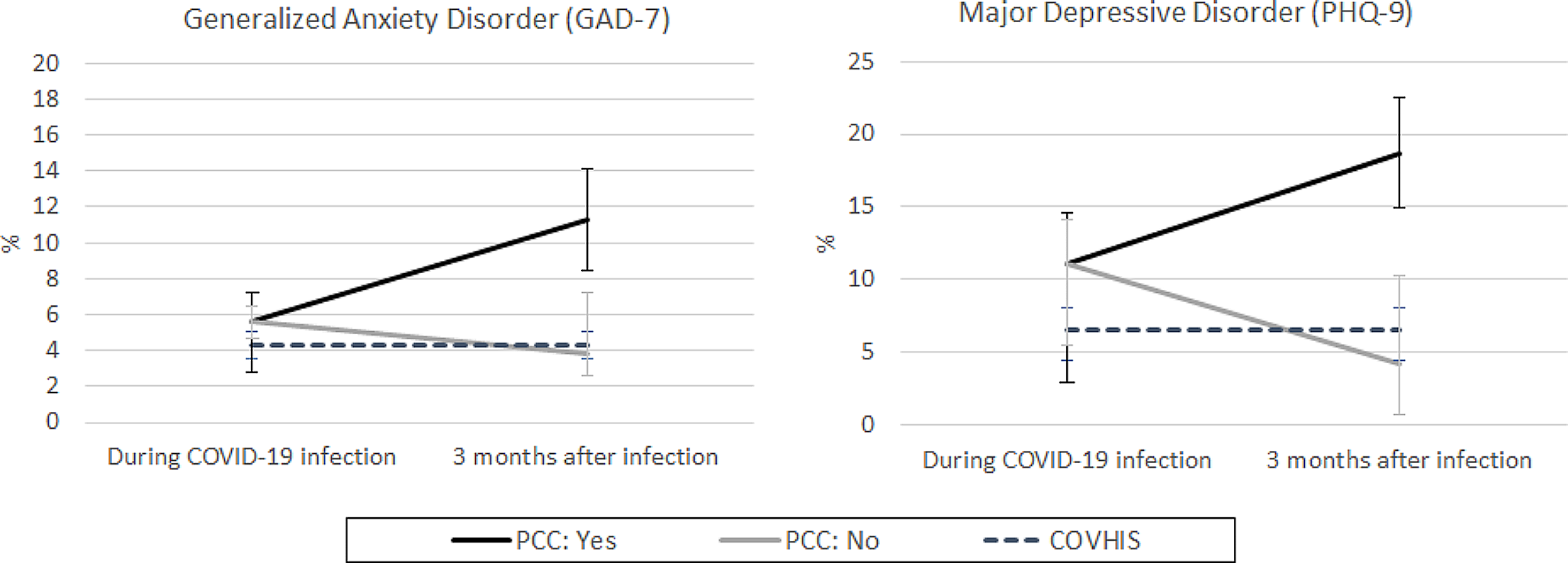
Postpartum psychiatric symptoms were measured 2 months after childbirth with the Edinburgh Postnatal Depression Scale (EPDS). This validated self-report questionnaire includes 10 items assessing symptoms of postpartum depression in the previous week, rated on a 4-point scale from 0 (no, not at all) to 3 (yes, quite often) [20, 21]. A sum score ranging from 0 to 30 was calculated with higher scores indicating more depressive symptoms. Women with a score of more than 12 were classified as having postpartum depression. This cut-off score had a sensitivity of over 80% and specificity of 95% in diagnosing postnatal depression in a clinical population [22, 23].
Social support
Social support was measured 6 months after childbirth using the Social Support List 12 – Interactions (SSL12-I), a validated 12-item abbreviated version of the full Social Support List – Interactions [24, 25]. Women were asked to indicate whether people around them are nice to them (e.g. give them compliments, invite them to join a party or dinner) or would help them (e.g. provide help in case of illness or moving houses, provide good advice), rated on a 4-point scale from 1 (seldom or never) to 4 (very often). A sum score ranging from 12 to 48 was calculated with higher scores indicating more social support. Women in the lowest tertile were classified as having low social support.
Covariates
The following variables were included as covariates and were measured during pregnancy or at birth: maternal age, migration background, socioeconomic factors (maternal education and household income), marital status, maternal and paternal lifetime psychopathology, substance use (drugs, smoking, alcohol) and gestational age at birth [26,27,28,29].
Statistical analysis
Prior to analyses, multiple imputations were performed to replace the missing values in child behavior, unintended pregnancy, postnatal depression, social support and the covariates using MICE package [30]. We created 30 imputed datasets with 100 iterations. Performing multiple imputation on the variables of interest is recommended to minimize attrition bias, in particular when auxiliary variables are available [31, 32]. Besides our variables of interest and covariates, we used the following variables as predictors for imputation because they have been related to pregnancy intention and/or child behavior problems and contain only a small amount of missing data: four digit zip code at birth, parity, maternal pre-pregnancy body mass index, folic acid intake, number of sexual partners in the year prior to pregnancy; and child ethnicity, birth weight and Apgar score after 5 min. These variables were all self-reported, except for birthweight and Apgar score.
Though our method shares some similarities with mediation analyses, it does not estimate the controlled or natural direct or indirect effects, which target the effect of changing the ‘exposure’ while fixing the value of the mediator [33]. Changing the ‘exposure’ (unintended pregnancy) would be very complicated, if not impossible, because the counterfactual of an unintended pregnancy is either an intended pregnancy or no pregnancy at all. In practice, it would only be possible to prevent unintended pregnancies. Hence, the prevention of unintended pregnancies (no pregnancy) would result in an absence of the outcome (childhood behavior). Therefore, we examined whether hypothetically eliminating postnatal depression and increasing social support may improve internalizing and externalizing problems in children of unintended pregnancies and thereby have the potential to reduce the differences in behavioral outcomes between children of intended and unintended pregnancies. This modelling approach is called G-estimation [13, 34].
As a first step we estimated the observed difference in problem behavior, and the association between postnatal depression, social support and problem behavior based on the observed data. Second, we modelled a situation in which all participants were set to ‘no postnatal depression’ and ‘high social support’. Third, we used the models of the second step to estimate the difference in problem behavior after postnatal depression was hypothetically eliminated and social support was hypothetically increased. The epidemiological design requires three causal assumptions: exchangeability, positivity and consistency. Exchangeability means no residual confounding or selection bias in the relationship of postnatal depression and social support with child behavior. We therefore adjusted for the earlier mentioned covariates [26,27,28,29]. Positivity indicates enough variation in postnatal depression and social support by levels of the covariates, which is likely satisfied given the sample size of the study population and there are no known structural reasons why positivity would be violated. Consistency requires well defined interventions, which might be violated because postnatal depression and lack of social support can be intervened on in different ways possibly resulting in different causal effects. This should be kept in mind when interpreting the results.
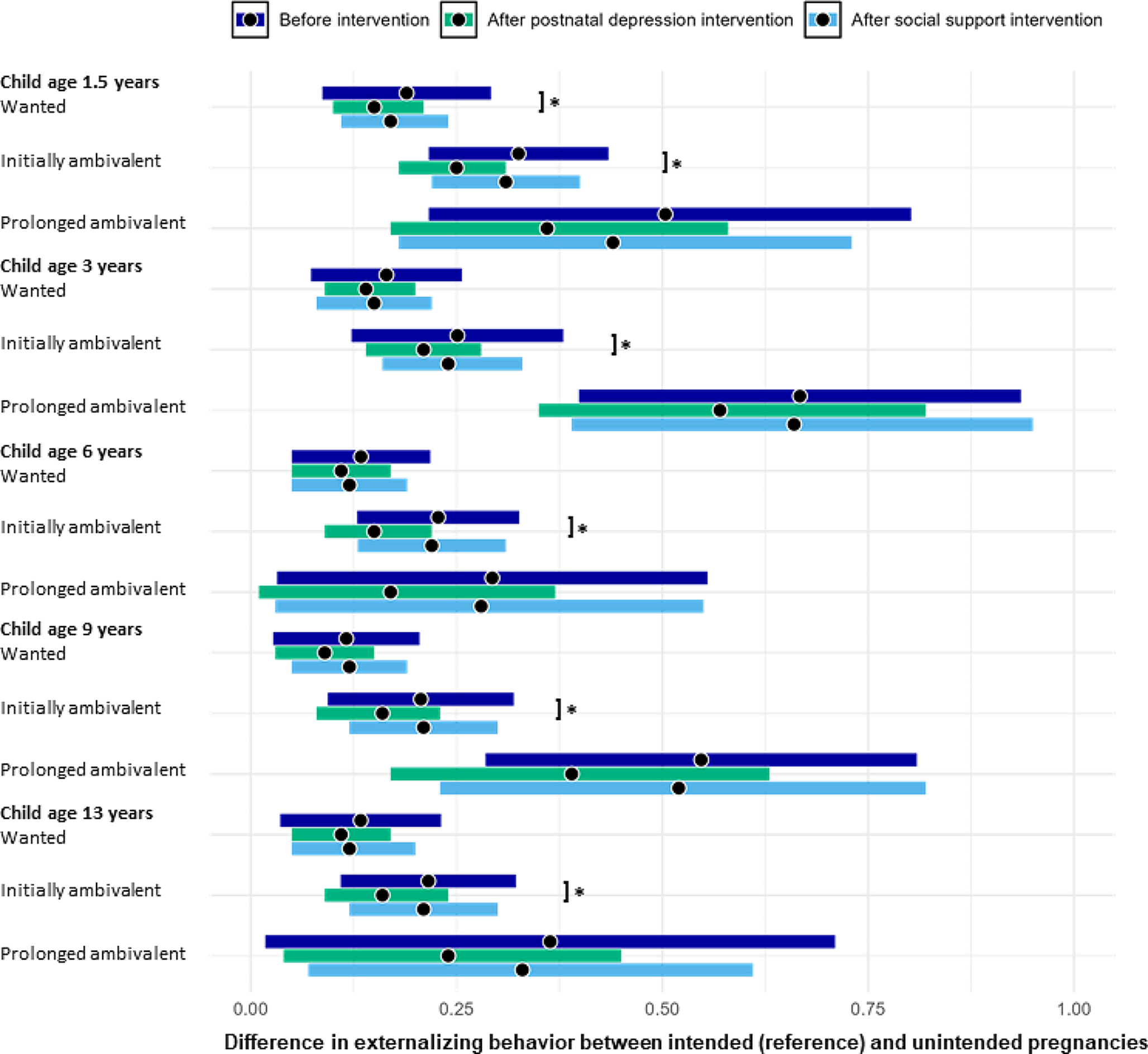
First, differences in internalizing and externalizing problems between pregnancy intention groups were estimated using linear regression models adjusted for child age and sex. Second, the associations of (1) postnatal depression, and (2) social support with internalizing and externalizing problems were estimated using linear regression analyses adjusted for the earlier mentioned covariates [26,27,28,29]. This model was subsequently used to obtain the estimated child behavioral outcomes if all study participants were set to ‘no postnatal depression’ or ‘high social support’. By comparing child behavior before and after adjusting postnatal depression and social support, the reduction in the differences in child behavior was estimated [13]. All analyses were run for internalizing and externalizing problems at ages 1.5, 3, 6, 9 and 13 years separately. Bootstrapping with 1000 iterations was used to calculate the 95% confidence intervals. Several sensitivity analyses were performed. Firstly, we used child self-reported internalizing and externalizing problems from the BPM at age 9 years and the YSR at age 13 years to determine whether reporting bias may have influenced our results. Secondly, in women who participated in the study with multiple pregnancies and/or women who gave birth to twins, a random child was excluded (analytical sample N = 9621). Thirdly, complete case analyses were performed by excluding dyads with missing data on unintended pregnancy, postnatal depression, social support or all child behavior questionnaires (N = 4244 for analyses with postnatal depression, and N = 3484 for analyses with social support). Finaly, as posthoc analyses, we repeated the analyses with dichotomized outcomes to assess the reduction in borderline clinical cases if all postnatal depression cases would be eliminated. All analyses were conducted in IBM SPSS version 28 and R statistical software version 4.2.1.


留言 (0)