We assessed the prevalence of PPD in Yunnan Province, China, and explored the associations between the full-time chain of pre-pregnancy–pregnancy–postpartum, sociodemographic–family support–social support, and PPD. We also expanded the time chain of PPD research, breaking through the causal mechanism of PPD occurrence beyond just physiological or social dimension. We realised the dynamic capture of PPD under the full-time chain, and mapped the vulnerability characteristics atlas of PPD from a multidimensional perspective. The study revealed a high prevalence of 46.1% for PPD in Yunnan Province, which is significantly higher than global (17.22%) and Chinese regional (21.4%) averages [18, 19]. Similar trends were observed when side-by-side comparing with cities such as Shanghai (23.2%) and Guangzhou (27.37%) [20, 21]. Traditional Chinese cultural beliefs regarding unique family dynamics and gender roles may lead to increased family conflicts and closed social networks [22], while China’s rapid economic growth has escalated life stress and elongated work hours [23]. Yunnan Province’s economy is relatively underdeveloped and the scarcity of healthcare resources led to mental health issues being easily neglected. In this study, the average age of childbearing for women was 34 years old. Considering the higher age of childbearing, concerns over medical risks contribute to an increased psychological burden [24]. These factors all contributed to the severe situation of PPD in Yunnan Province. Based on the full-time chain perspective, the PPD prevalence was higher among mothers with poor pre-pregnancy health (64.86%) and sleep problems during pregnancy (often insomnia, sleep poorly: 61.32%; somnolence: 51.74%); and mothers with double fetuses of one male and one female infant had better mental health status after giving birth. In the multidimensional analysis, only family care and only other people care were positive factors for PPD in the family support dimension; going to work or going online had a protective effect on mothers’ health.
Prevention and treatment of PPD should focus on the whole pre-pregnancy–pregnancy–postpartum period and extend the intervention chain.
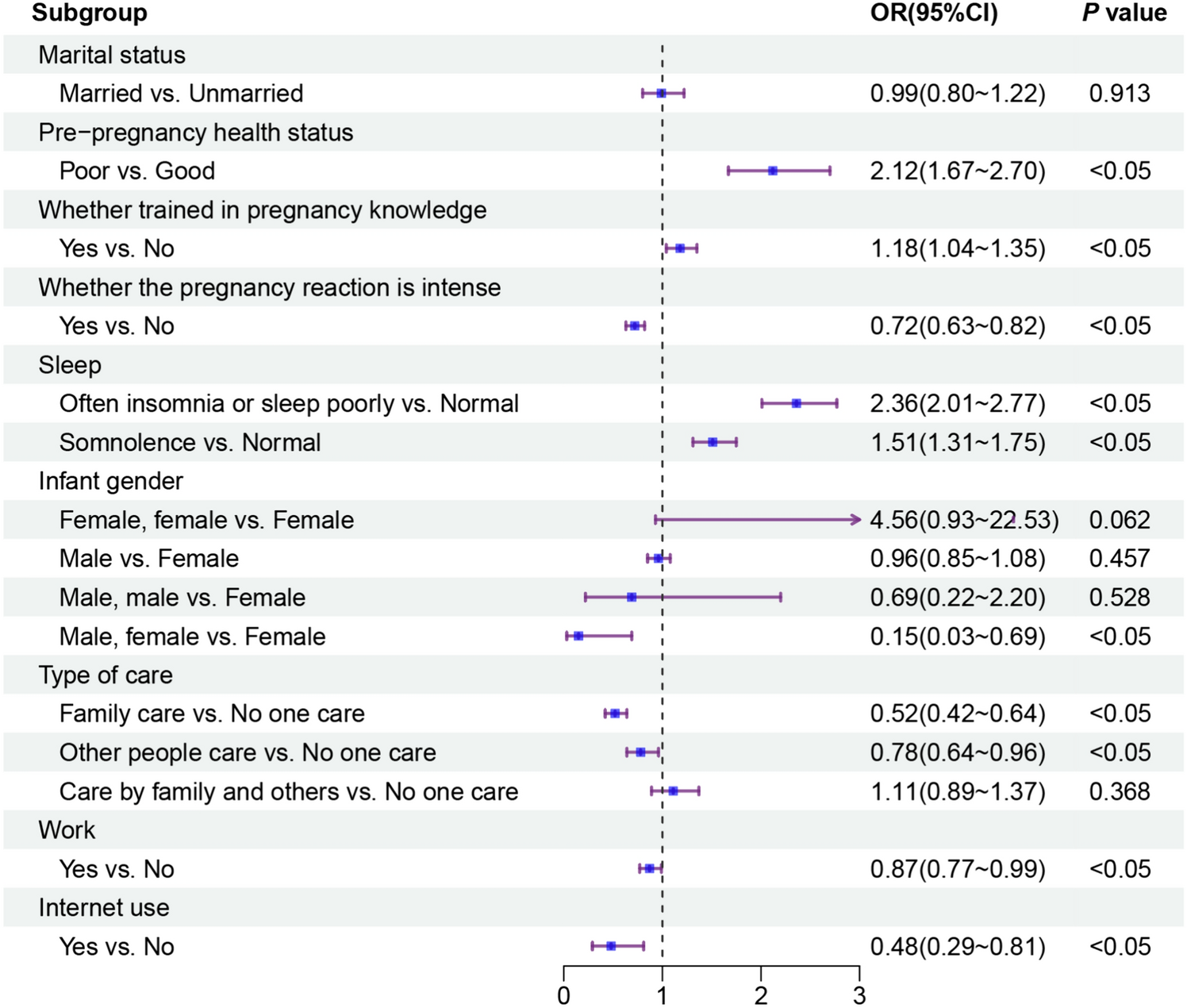
The PPD experience risk of women with poor pre-pregnancy health was (2.12 times) higher than women with good. This result is consistent with the findings of Michael W. O'Hara et al. [25]. In the pre-pregnancy period, mothers had a previous depression history or possible comorbidities such as hypertension, diabetes, gynecological disorders, with a low physical health level [26, 27]; and in the postpartum period, they suffered from fatigue, pain in wounds, and weakness [28, 29]. The multiple discomforts superimposition makes mothers more prone to postpartum psychiatric problems, such as anxiety, depression, and despondency. Notably, mothers with pregnancy knowledge training were more likely to experience PPD. The possible reason is the mothers with pregnancy knowledge training were more aware of the psychological and physiological changes, that occur during pregnancy and the postpartum period, and they were more likely to think what may cause unnecessary tension, anxiety, and uneasiness [30, 31]. And this increased the PPD experience risk. During the pregnancy period, often insomnia or sleep poorly/somnolence hurt mothers; Some studies have indicated that mothers who sleep 6 h or less were more likely to experience PPD, and sleeping more than 8 h did not significantly decrease the PPD prevalence [32]. The major neurotransmitter systems in the brain involved in regulating sleep have been linked to the development of psychiatric disorders [33]. Therefore, neurotransmitter imbalances can lead to PPD increase. In the postpartum period, twin births of a male and a female infant were a protective factor compared to having only single female infant. In the context of traditional Chinese fertility culture, family members may show some negative reactions to female infants’ birth, that may result in less support for mothers giving birth to a female fetus; whereas a preference for male fetus may be communicated to mothers, and ease their postpartum stress [34]. Additionally, lower marital satisfaction following the birth of female fetus may explain for the increased risk of PPD among the mothers with female fetus. Family members should be well-informed about pregnancy-related matters and offer psychological support to pregnant women. mothers need to maintain a healthy lifestyle and engage in activities that alleviate stress. After childbirth, the focus should shift from solely preventing PPD to prevention and treatment. Nursing interventions are provided to mothers without PPD. Receiving prompt follow-up visits and developing personalized treatment plans is crucial for individuals who have suffered from PPD.
The prevention and treatment of PPD are inseparable from the dual support of family and society, with social support playing an increasingly prominent role.
In terms of family support, only family care and only other care were protective factors of PPD. Family care is the main resource of family support [35]. Family not only provides tangible support such as material and financial support, but also offer mental support from family members, especially husbands, which greatly enhances mothers’ self-esteem and self-confidence, alleviating tension and stress during various pregnancy stages. In addition to family members, medical personnel, friends and colleagues also influence mothers by providing information support, emotional accompaniment and value recognition [36, 37]. In terms of social support, going to work or going online can reduce the risk of PPD, it not only increases mothers’ self-efficacy, but also provides the understanding and appreciation they need as they transition to motherhood [38]. The social climate in social networks reflects a stigma associated with mental health problems, which acts as a barrier to seeking professional help for mothers. However, positive social behaviours can enhance cognitive abilities of mental health problems, overcome perceptual barriers and help-seeking intentions, and reduce the stigma of mental illness [39]. Family support for mothers should encompass emotional, informational, material, and interactive aspects, focusing on recognizing emotional shifts, providing comfort, sharing childcare knowledge, and ensuring effective communication. Communities ought to deliver holistic primary health care, including early detection, education, and postpartum support. The government should consider establishing childcare allowances and creating job opportunities to facilitate mothers’ societal reintegration post-birth.


留言 (0)