
記住我
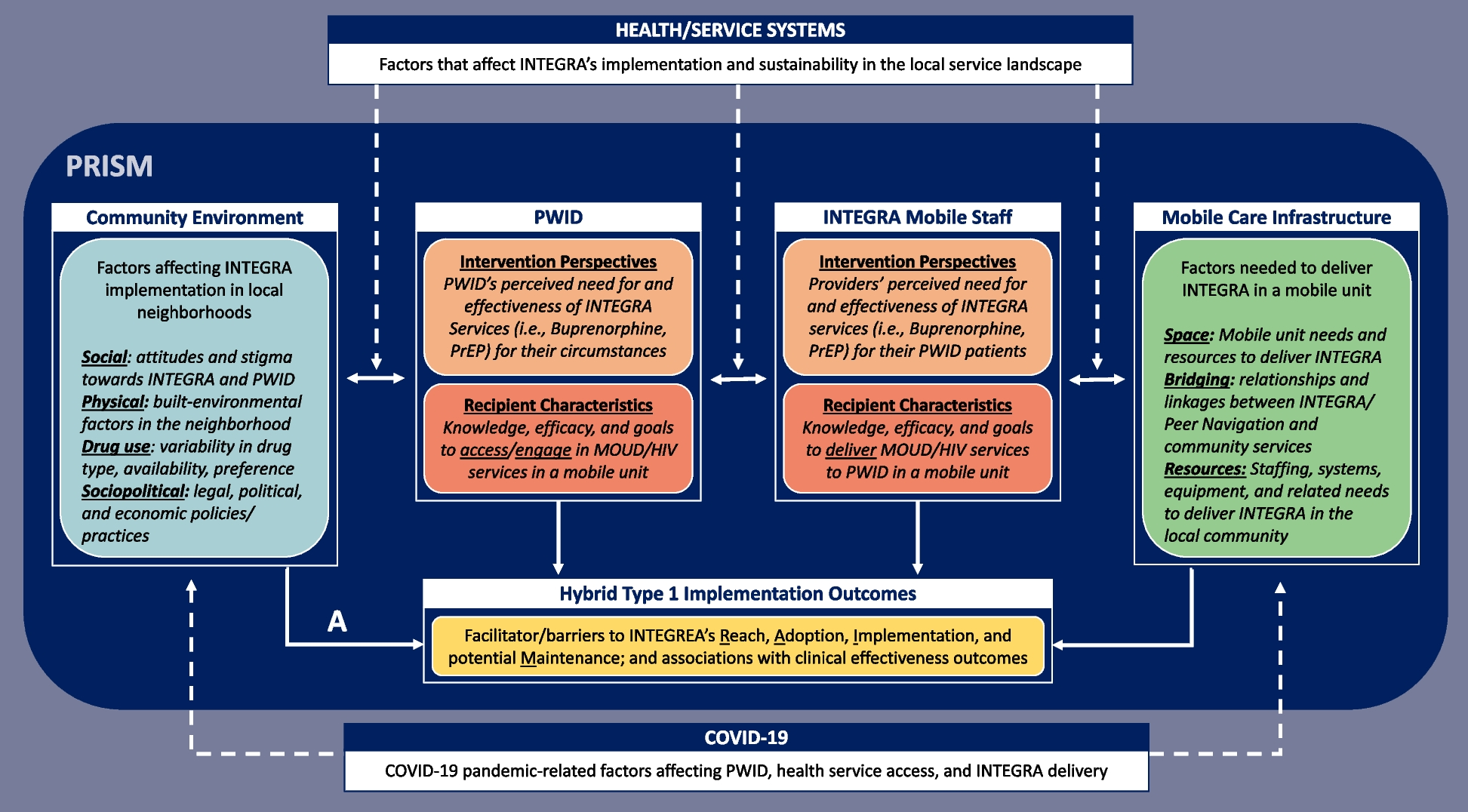
Findings are organized by pre-implementation neighborhood selection (Fig. 2A) and the range of geographic area covered across neighborhoods in the implementation phase (Fig. 2B). We report on the contextual barriers and facilitators that characterized the viability of implementation neighborhoods and the benefit of utilizing additional systems to guide real-time implementation decisions beyond the pre-implementation surveillance data.
Fig. 2
Geographic Coverage of the HPTN 094 Complex Intervention Data-Driven Implementation Mapping Process. Figure 2 depicts the data-driven process to identify priority implementation neighborhoods in the pre-implementation phase and characterize viable implementation neighborhoods in the two-year implementation phase
Pre-implementation neighborhood selection for delivering INTEGRA to PWIDGuided by HIV and overdose surveillance data, a total of 24 priority neighborhoods were identified across all sites, 10 of which were in Houston (Table 1). Across priority neighborhoods, HIV incidence was highest in Downtown LA (1,106 per 100,000), followed by Houston (Greater Third Ward=562 and Kashmere Gardens=508 per 100,000, respectively). Comparatively, the highest overdose death rates were observed in Philadelphia’s Kensington neighborhood (327.0 per 100,000), followed by Downtown LA (175.5 per 100,000) and the Sunnyside neighborhood in Houston (151.7 per 100,000).
Table 1 Pre-implementation priority neighborhood characteristicsPriority neighborhoods differed regarding the number of community services providing HIV, MOUD, harm reduction, or primary care services within the neighborhood boundaries (Fig. 2B). Houston had substantially lower access to services within priority neighborhoods (Range: 0-3 community services per neighborhood; Table 1). Comparatively, priority neighborhoods in NYC, Philadelphia, and some areas of LA had greater access to services (Range 12-37), with the highest number of services documented in Philadelphia’s Kensington neighborhood. Probative observations identified that the higher number of services in Philadelphia was due to a standing order for all pharmacies to provide naloxone, substantially increasing access to harm reduction services across the city. Notably, systems where PWID may re-enter the community (i.e., emergency rooms, jails, prisons) were highest in NYC’s Melrose/Mott Haven and East Harlem Neighborhoods and Houston’s First Ward neighborhood.
Implementation neighborhood geographic coverage and enrollment characteristicsOf the 24 priority neighborhoods identified in the pre-implementation landscape analysis, 18 were initiated in the implementation phase, as were 17 new neighborhoods not previously identified through the landscape analysis. Six priority neighborhoods were never initiated, including three in NYC and Philadelphia due to existing high-enrollment neighborhoods, and three in Houston with limited mobile unit parking options (i.e., First Ward) or because other viable neighborhoods emerged via local response systems described below.
As observed in Fig. 2B, the geographic density of implementation sites within neighborhoods is greatest in NYC and Philadelphia, where open drug markets provided concentrated areas to reach eligible PWID (Table 2). Both East Harlem and Kensington high enrollment neighborhoods are characterized as well-known areas to procure drugs, so the need to move the mobile unit within these neighborhoods was minimal. Notably, the implementation sites in Kensington covered an area less than 1 mile in length but accounted for 398 of the 410 days the mobile unit was in the field. Field staff determined after 12 days that PWID identified in West Philadelphia were also frequenting the Kensington neighborhood, where they expressed preference for engaging with the mobile unit. Similarly, NYC teams described the need to move the mobile van a few blocks to reach PWID who can’t cross specific streets due to drug turf boundaries:
Identified a few places to move to keep things Fresh! Gated area called ‘Little Jungle’ an encampment where folks sleep at night and use two blocks from where the van (mobile unit) is parked. Some folks just don’t make it that far so bringing the truck over to this street… A block up from little Jungle is Big Jungle – runs under the L – another population that doesn’t make (it) two blocks down to our truck (mobile unit) so thinking to try this area out after next week.” (Steering Committee Meeting 09/09/2022)
Table 2 Implementation Neighborhood PWID Enrollment Characteristics (N=358)aIn contrast, new neighborhoods not identified in the pre-implementation landscape analysis were largely initiated in DC, Houston, and LA, where the locations of PWID were more dispersed throughout the cities (Table 2). This required sites to leverage additional data points to identify new neighborhoods and determine the viability of these neighborhoods, as described below. This approach supported the emergence of Downtown LA as a high enrollment neighborhood due to the concentration of PWID found through Project Room Key, a COVID-related housing response for homeless individuals in LA. In contrast, Ward 5 emerged as DC’s high enrollment neighborhood because it provided a safe and easily accessible location through which PWID identified via outreach in other neighborhoods could access the mobile unit using public transportation. Houston covered the largest geographic range, with 16 interconnected implementation neighborhoods, and was the only city without a high enrollment neighborhood.
Contextual barriers affecting the viability of implementation neighborhoodsCross-site heterogeneity in sociopolitical and drug use environments affected the viability of some implementation neighborhoods. For example, the geographic diversity of cities required greater driving distances to cover larger geographic regions in Houston and across LA County to reach PWID. As noted, “LA geography – everything is out of the way – nothing is close – makes it challenging to get places because traffic is between distance” (Steering Committee Meeting, 03/24/2023). Similarly, proximity to and need for social services in low-income areas resulted in high engagement but low enrollment due to community members seeking access to housing, employment, and healthcare resources. For example, in Houston:
“Community member stated that most of the drug use in the area is non-injection crack and recommended mobile unit moves further East; stated main problem in the Sunnyside area is poverty, so social services (housing, jobs, ID, crime prevention) are needed more than help for opiate use.” (Sunnyside, Ecological Observation, 10/18/2021)
Policing and surveillance of PWID were observed across all study sites, particularly the policing of unhoused individuals ramped up in response to election cycles. Exposure to violence was reported across implementation sites, with more frequent reports occurring in Philadelphia, DC, and Houston. An illustrative quote from Philadelphia details, “more violence and gunshots around the past 6 months. Not affecting participants enrolled yet or ability to recruit, but violence is coming up more” (IS Team Meeting, 10/07/2022).
Increased police activity, driven by sociopolitical pressures and amplified surveillance efforts, sometimes hindered new enrollments across all sites. Specifically, in NYC and DC, the viability of certain implementation neighborhoods was affected. The East Harlem neighborhood, which had been NYC's exclusive implementation site for over a year, became untenable after an outdoor police command unit was established at a key drug-purchasing route. This sustained law enforcement presence altered drug activity in the area, prompting the NYC site to pursue an alternative implementation neighborhood. In DC, over-policing and 24-hour surveillance efforts linked to ongoing gentrification in Ward 1, 4, 7, and 8 neighborhoods effectively drove PWID from well-established drug-using neighborhoods, signaling a transition away from more open-air drug-use environments. As described, “Construction and gentrification in the area has pushed out much of the population that injects. We received information that most PWID can be found on the side streets… but most the people who hang out on the main road and wall in front of McDonalds snort or smoke” (Ward 7, Ecological Observation, 03/18/2022).
Heterogeneity in local drug use environments limited the utility of overdose data to identify viable neighborhoods in areas where PWID are more dispersed. In discussing surveillance data limitations in Philadelphia, one staff described:
“Starting to go more West Philly. Most folks are not injectors or not injecting opioids. West Philly (PWID) are going into Kensington anyway from home to go buy drugs and use (sterile syringe program) services. So, Kensington still most high enrollment.” (Steering Committee Meeting, 01/27/2023)
In Houston’s Sunnyside neighborhood, fatal overdoses did not reflect injection as the primary route of opioid administration. Insight into this was provided by staff who noted, “A lot of the spaces we are going to that have largely Black communities they are not injecting or they are not using opioids, mostly cocaine” (Steering Committee Meeting, 08/26/2022). Identifying viable neighborhoods when PWID are more geographically dispersed required additional strategies (e.g., support from Pastors [Houston]) to build rapport among people who use drugs in new neighborhoods and obtain insights on the local drug use environment.
Ecological observations documenting exposure to violence, both persistence and increases, were noted across sites and described as a key barrier to onboarding some implementation sites. For example, in an IS Meeting probing experiences related to safety and well-being, DC staff describe that there are:
“Increases in violence since the start of study… the team did witness a shooting across the street. This does determine where we will and will not go…Used to be more predictable; violence happened in the evening but it’s happening more in daytime. And yesterday shooting, at 12 noon, 4 people shot. But not too far from (implementation neighborhood with) high level of OD (overdose).” (10/07/2022)
All sites reported encountering opioid users who either refrained from injecting or switched to smoking due to the higher overdose risk with fentanyl in the drug supply. To address challenges in finding PWID in gentrifying neighborhoods, DC used pre-screen surveys delivered by outreach teams to engage with community members and assess the current drug use landscape. As reported:
“People are just not injecting opioids – opioid use is definitely changing. More cocaine and crack smokers. These (outreach sites) are areas driven by opioid deaths. Except that the stimulants are laced with fentanyl. 55% of participants are reporting poly substance use in the past month. Moving from injection to sniffing. The proportion of injectors is lower than before.” (Steering Committee Meeting, 08/26/2022)
Contextual facilitators affecting the viability of implementation neighborhoodsOutside of known open drug markets, our IS data revealed that identifying viable implementation neighborhoods in areas with geographically dispersed PWID was supported through a multi-faceted approach. Specifically, local overdose data needed to be augmented by community insights on where opioids and injection behaviors could be found in the neighborhood alongside proximity to built physical environmental factors and local integrated response systems. Through data triangulation, suitable neighborhoods for implementation were pinpointed.
The viability of implementation neighborhoods was improved by identifying factors in the built physical environment, such as local venues in LA and Houston (e.g., gas stations, encampments/apartment complexes) and services systems, particularly public transportation hubs, in Houston and DC. For example, “Heavy overdoses in the… tent city in Northside Village where we got lots of (internal) referrals” (Steering Committee Meeting, 08/26/2022). These points of connection facilitated outreach and recruitment via greater foot traffic in the neighborhood when venues were known to be associated with drug sales/use, as reflected in Houston’s observations of the Greater Third Ward neighborhood:
“New Neighborhood. Very tight-knit community, historically low-socioeconomic status and (racial/ethnic) minority residents. Location chosen due to very high level of drug activity/sales in the area. Very high foot traffic... 26 visitors which is about 3 times the usual amount of visitors… A few blocks from Metro Light Rail line. New site is at a gas station that is frequented by community members... Community members that stopped by were very welcoming and accepting … stated that we are parked in the right spot for what we are doing.” (Ecological Observation, 10/18/2022)
Less viable neighborhoods in Houston had convenient freeway access to the implementation sites, yet, these locations were mainly accessible to PWID with personal vehicles, driving from different parts of the city to reach the mobile unit. For example, "(Sunnyside is) not offering candidates that live in the neighborhood. Candidates drive from other neighborhoods (East of Downtown) (Ecological Observation, 10/07/2021).”
Uniquely, DC leveraged a well-known and busy intersection at a strip mall (the metro center in Ward 5) to establish its strongest implementation site. This strip mall is a trusted area PWID felt safe traveling to meet up with the mobile unit when recruited via outreach teams in neighborhoods where it was deemed unsafe to park the unit for prolonged periods of time. As such, DC staff noted, “Having a second mobile unit that is smaller is very helpful… (for) field safety and security…Smaller unit (not used to implement integrated care) is making it easier to get in and out of these places quickly to scope them out.” (Steering Committee Meeting, 02/10/2023)
Leveraging local response systems as a real-time data-driven strategyAll sites continued to monitor local overdose data to identify potential implementation sites. Identifying and linking into local overdose and housing response systems was beneficial where there was greater geographic dispersion of PWID. This process helped to identify viable implementation neighborhoods in Houston and LA. Monitoring overdose data from the Houston Fire Department's overdose response unit and the city's homeless outreach team helped identify viable neighborhoods and where to move the mobile unit within existing neighborhoods in real-time.
“Houston Fire Dept has an outreach worker that follows up with individuals that received care for overdose. (Our Peer Navigation) Supervisor rides along with outreach worker and shares neighborhood information with HPTN 094 Team when there are clusters of overdoses.” (Northside Village Neighborhood, Ecological Observation, 05/02/2022)
“Planning to move to another parking location within the same neighborhood because the area was listed on the Houston Fire Dept "overdose surveillance list". Participants from the community gathered at mobile unit for moral and emotional support after getting news of recent overdose death of a participant.” (Magnolia Park Neighborhood, Ecological Observation, 02/21/2022)
While DC's overdose data confirmed overdose hotspots in their implementation neighborhoods, responses to overdose spikes often led to increased police presence and community surveillance, pushing PWID further underground and out of reach of the study team. Following a cluster of ten overdoses, the DC site reported, “Doing a lot of community work with the Department of Behavioral Health and community-based organizations. We are now part of the rapid response (to) overdose spikes… (It’s become) public news, by (the) 7-11, police put remote devices in the areas where there are overdoses” (Steering Committee Meeting, 02/25/2022).
In comparison, the LA site connected with housing response systems that emerged during the COVID-19 pandemic (e.g., Project Room Key in Downtown Hotels, Tiny Home Villages across LA County). This approach proved more effective in identifying viable implementation neighborhoods than solely relying on local surveillance data.
“Overdose data and HIV maps took us to Long Beach, but (the data are) really not granular. So hard to locate where to actually park. (When we first moved) into downtown LA – we followed overdose data to MacArthur Park. It was not useful. There were overdose deaths yes, but they were not our people. Our (next) struggle was following these transitional housing units in place - in response to COVID, but (the housing units) are staying in response to housing crisis. Find these units - park there, 10% of the population at a given site meet inclusion criteria. So tiny homes at Highland Park 100 units, enrolled 10, Eagle Rock 40 units, enrolled 4. Multiple enrollments in Project Room Key (Downtown LA) - originally had 4 sites, the other 2 sites were outside our geographic desired areas.” (IS Meeting, 08/05/2022)
留言 (0)