
記住我
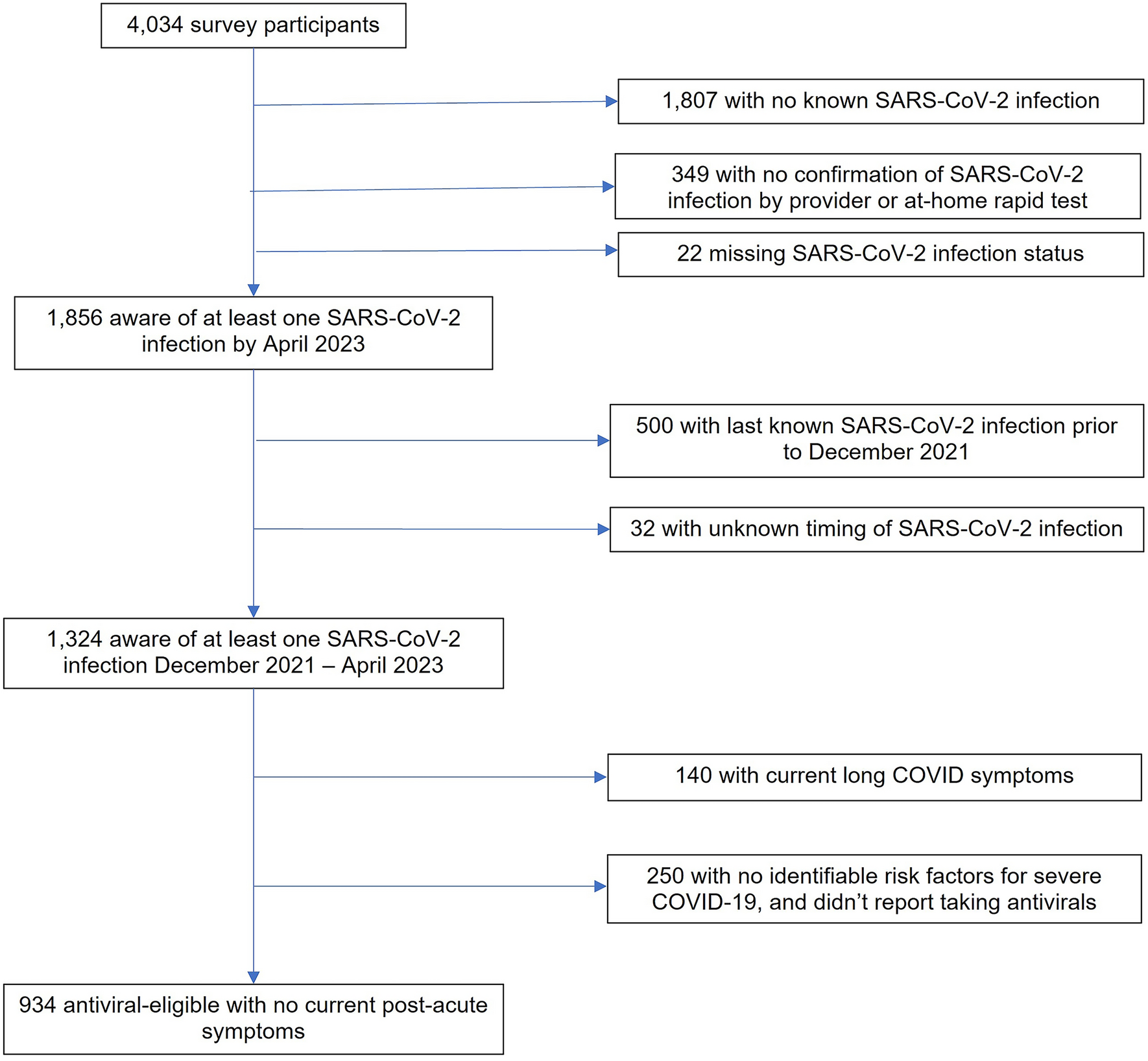
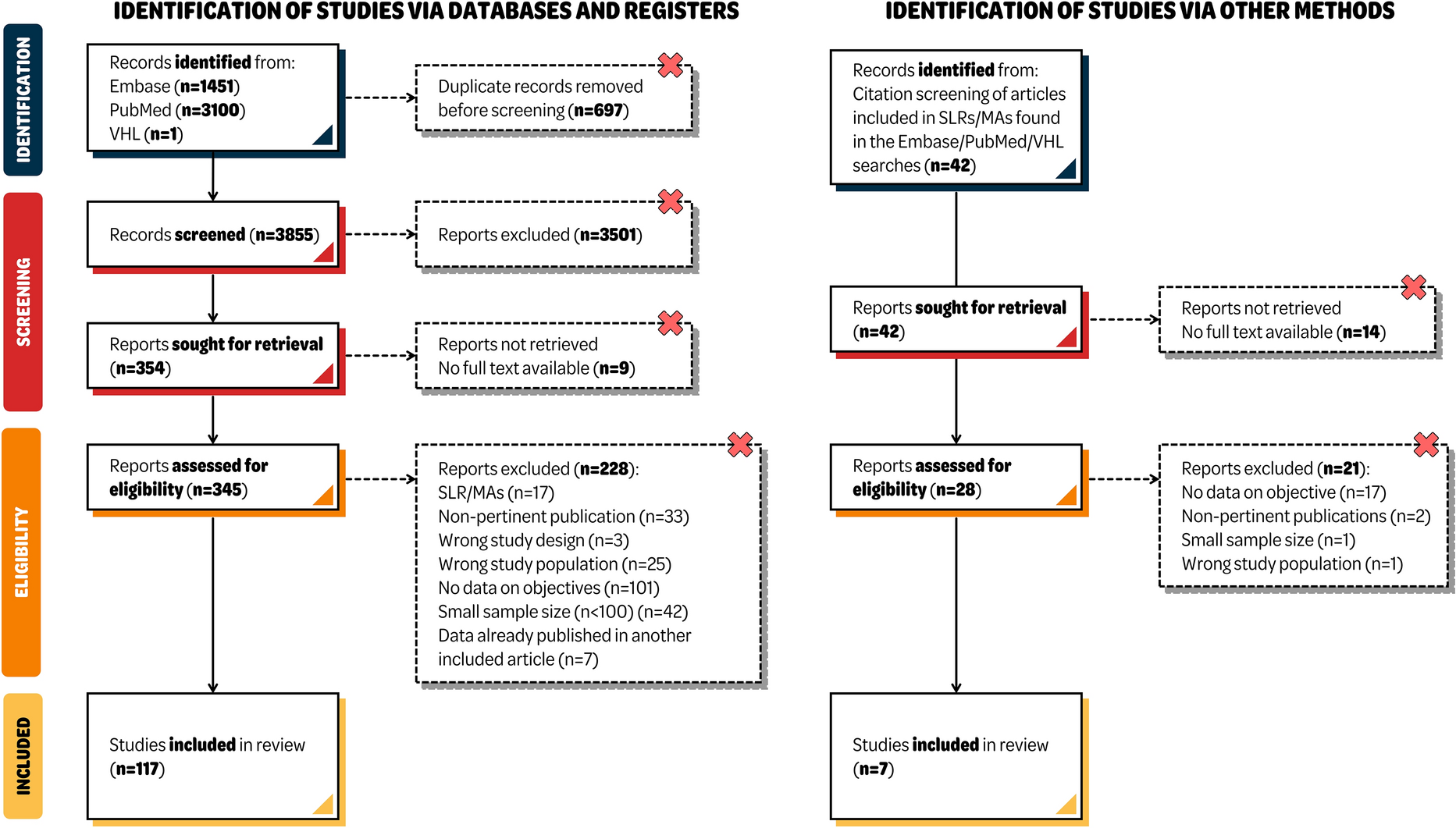
A total of 1006 publications were identified. After further screening and exclusion, 24 relevant full-length articles were included in the qualitative synthesis and 8/24 articles in the quantitative synthesis (meta-analysis) (Fig. 1). Included publications reported data for a total of 1114 patients (bacteremia: 946, nosocomial pneumonia: 168) treated with CAZ-AVI either as a part of monotherapy, combination therapy, or both, and 640 patients (bacteremia: 539, nosocomial pneumonia: 101) treated with alternative or comparator antibiotics. The majority of patients included had bacteremia or pneumonia due to Enterobacterales except for two studies where patients with P. aeruginosa (bacteremia: CAZ-AVI—24, other antibiotic—37) [22, 23] infections were included.
For completeness, data from five relevant case series with aggregate data reported for bacteremia and nosocomial pneumonia is presented separately in Supplemental Tables 2 and 3.
Study CharacteristicsPublications comprised 12 retrospective cohort studies [23,24,25,26,27,28,29,30,31,32,33,34], ten retrospective comparative/case–control studies [22, 35,36,37,38,39,40,41,42,43], and two prospective registry studies [44, 45] (Table 1, Fig. 2A). Most studies were 2020 onwards and were from China [22, 26, 30, 31, 33, 39, 41, 43] and Spain [23, 25, 32, 36, 42, 45] (Fig. 2B and C).
Table 1 Summary of studies included in quantitative and qualitative synthesisFig. 2
Pie charts for the study characteristics (A) study types, (B) study period, and (C) region/country
Of a total of 24 studies, 13 included patients with infection caused by K. pneumoniae, comprising six studies focused on CR-K. pneumoniae (CRKP, mechanism of resistance not reported), five studies focused on KPC- K. pneumoniae, and two studies focused on OXA-48K. pneumoniae. Six studies included patients with infections caused by more than one Enterobacterales comprising three studies focused on carbapenemase-producing Enterobacterales (CPE) and three studies focused on CRE. Two studies included patients with infection caused by P. aeruginosa (MDR/extensive drug-resistant, CR), and three studies with mixed pathogens.
Outcomes were not segregated based on the type of CAZ-AVI treatment (mono/combination) for bacteremia and nosocomial pneumonia in the included studies, hence outcomes extracted for the CAZ-AVI group include data from patients treated with either monotherapy, combination therapy, or both. We could extract separate outcomes for patients with bacteremia in 16/24 studies, patients with nosocomial pneumonia in 2/24 studies, and for both bacteremia and nosocomial pneumonia in 6/24 studies.
Patients with BacteremiaQualitative SynthesisMortality was reported in 18/22 studies which enrolled patients with bacteremia (Table 2). Overall, 30-day mortality was 24% (n = 217/904) in patients treated with CAZ-AVI and 40.12% (n = 199/496) in patients treated with other antibiotics.
Table 2 Outcomes of studies involving ceftazidime-avibactam for the treatment of patients with bacteremia or nosocomial pneumoniaClinical cure was evaluated in 11/22 studies. Overall, clinical cure rates were 80.33% (n = 196/244) in patients treated with CAZ-AVI and 54.15% (n = 124/229) in patients treated with other antibiotics.
Microbiological cure occurred in 58.33% (n = 42/72) of patients in the CAZ-AVI group and 35.90% (n = 14/39) of patients in the comparator group, which was in a single study (Table 2) [42]. Resistance to CAZ-AVI was observed in 2.89% (n = 19/656, repeat susceptibility data not available) patients during the therapy, reported across five studies [24, 28, 29, 36, 44].
Sources of bacteremia were reported in six studies, but outcomes could not be differentiated by source. Overall, 10.80–99.30% of patients had bacteremia secondary to a pulmonary source sites [22, 33, 35, 36, 40, 43].
Quantitative Synthesis (Meta-analysis)Of the total eight studies included in the quantitative synthesis, there was no statistical heterogeneity among included studies (I2 = 0%; P = 0.72–0.99), and therefore a common effect model was applied for all outcomes.
MortalityAll-cause 30-day mortality was evaluated in all eight studies (Fig. 3A). Overall, observed 30-day mortality was 15.38% (n = 32/208) in the CAZ-AVI group and 40.12% (n = 199/496) in the comparator group. Study heterogeneity was low (I2 = 0%, P = 0.99). Lower odds of 30-day mortality were evident among patients treated with CAZ-AVI versus comparators (Odds ratio [OR] = 0.30, 95% CI 0.19–0.46) (Fig. 3A) [22, 35,36,37,38, 40, 42, 43].
Fig. 3
Meta-analysis of studies reporting 30-day mortality and clinical cure outcomes in patients with bacteremia. I2 significance of heterogeneity, CI confidence interval, OR odds ratio, Te number of events observed in the treatment group, TN total number of patients in the treatment group, Ce number of events observed in the comparator group, CN total number of patients in the comparator group
Clinical CureClinical cure was evaluated in five studies (Fig. 3B) [36,37,38, 40, 42]. Overall, the clinical cure rates were 89.19% (n = 132/148) in the CAZ-AVI group and 54.15% (n = 124/229) in the comparator group (Fig. 3B). Study heterogeneity was low (I2 = 0%, P = 0.72). Higher clinical cure rates were evident among patients treated with CAZ-AVI vs. comparators (OR = 4.90, 95% CI 2.60–9.23).
Patients with Nosocomial PneumoniaQualitative AnalysisOf a total of eight studies that reported outcomes of patients with nosocomial pneumonia, mortality was reported in 6/8 studies (Table 2). Overall, all-cause 30-day mortality rates were 32.17% (n = 46/143) in patients treated with CAZ-AVI based therapy and 34.62% (n = 27/78) in patients treated with other antibiotics. Clinical cure was evaluated in 5/8 studies. Overall, clinical cure rates were 61.16% (n = 63/103) in patients treated with CAZ-AVI and 34.62% (n = 27/78) in patients treated with other antibiotics.
Microbiological cure was evaluated in five studies with overall rates of 63.21% (n = 67/106) in patients treated with CAZ-AVI and 30.77% (n = 24/78) in the patients treated with other antibiotics. Resistance was not reported in any of the studies.
Quantitative Synthesis (Meta-analysis)Mortality and Clinical CureAll cause 30-day mortality and clinical cure was evaluated in two studies (Fig. 4) [39, 42]. The 30-day mortality was 27.27% (n = 18/66) in the CAZ-AVI and 34.62% (n = 27/78) in the comparator group (Table 2). Study heterogeneity was low (I2 = 0%, P = 0.47). However, since data was available from two studies with high confidence interval (OR = 0.73, 95% CI 0.35–1.49), no definitive conclusions can be made (Fig. 4A). Clinical cure rates were 65.15% (n = 43/66) in the CAZ-AVI and 34.62% (n = 27/78) in the comparator group. Study heterogeneity was low (I2 = 28%, P = 0.24). Higher clinical cure rates were evident among patients treated with CAZ-AVI versus comparators (OR = 3.20, 95% CI 1.55–6.60) (Fig. 4B).
Fig. 4
Meta-analysis of studies reporting 30-day mortality, clinical cure, and microbiological cure in patients with nosocomial pneumonia. I2 significance of heterogeneity, CI confidence interval, OR odds ratio, Te number of events observed in the treatment group, TN total number of patients in the treatment group, Ce number of events observed in the comparator group, CN total number of patients in the comparator group
Overall, in patients with nosocomial pneumonia higher rates of clinical cure were noted among patients treated with CAZ-AVI versus the comparator group; however, no differences were noted for mortality.
Microbiological CureMicrobiological cure was 63.63% (n = 42/66) in the CAZ-AVI and 30.76% (n = 24/78) in the comparator group, also evaluated in the above two studies [39, 42]. Study heterogeneity was low (I2 = 0%, P = 0.55). Higher microbiological cure rates were evident among patients treated with CAZ-AVI versus comparators (OR = 4.95, 95% CI 2.34–10.46) (Fig. 4C).
Renal Failure at BaselineRenal failure at baseline in patients with bacteremia was present in 26.50% of patients with CAZ-AVI (n = 159/600, four studies) and 19.51% in patients received other antibiotics (n = 16/82, two studies [28, 29, 36, 42]. The 30-day mortality in these studies was 22.17% in the CAZ-AVI and 28.40% in other antibiotics group; clinical cure was 93.65% in the CAZ-AVI and 75.45% for other antibiotics group. For nosocomial pneumonia, renal failure at baseline was reported in a single study (CAZ-AVI: 26.10%, other antibiotics: 12.5%) [42]; 30-day mortality was 21.70% in the CAZ-AVI and 37.50% in other antibiotics group; clinical cure was 91.30% in the CAZ-AVI and 56.20% for other antibiotics group.
Mortality PredictorsMortality predictors were reported in 19 studies, of which 17 used multivariate analysis [22,23,24, 26, 28, 29, 31,32,
留言 (0)