
記住我

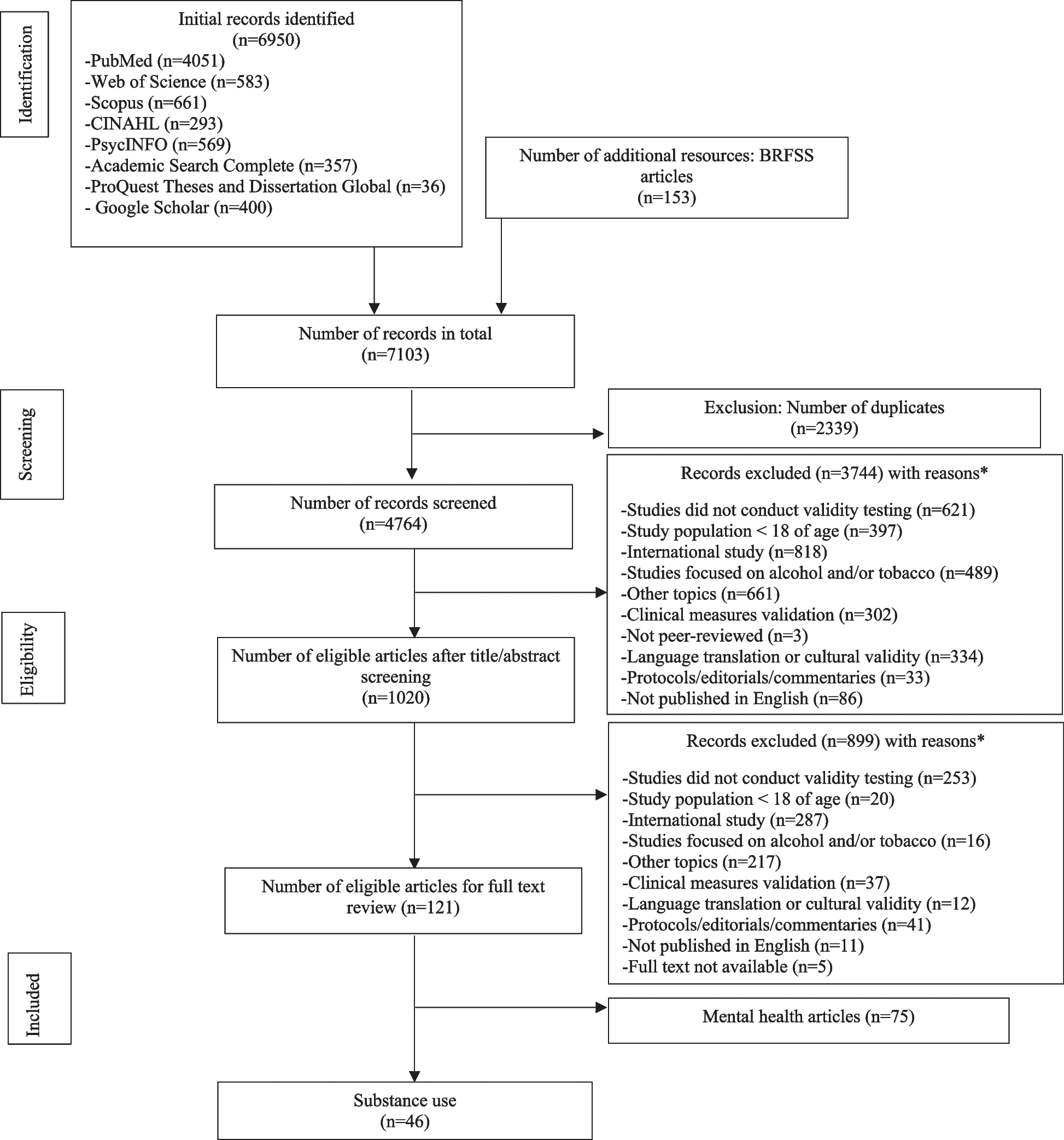


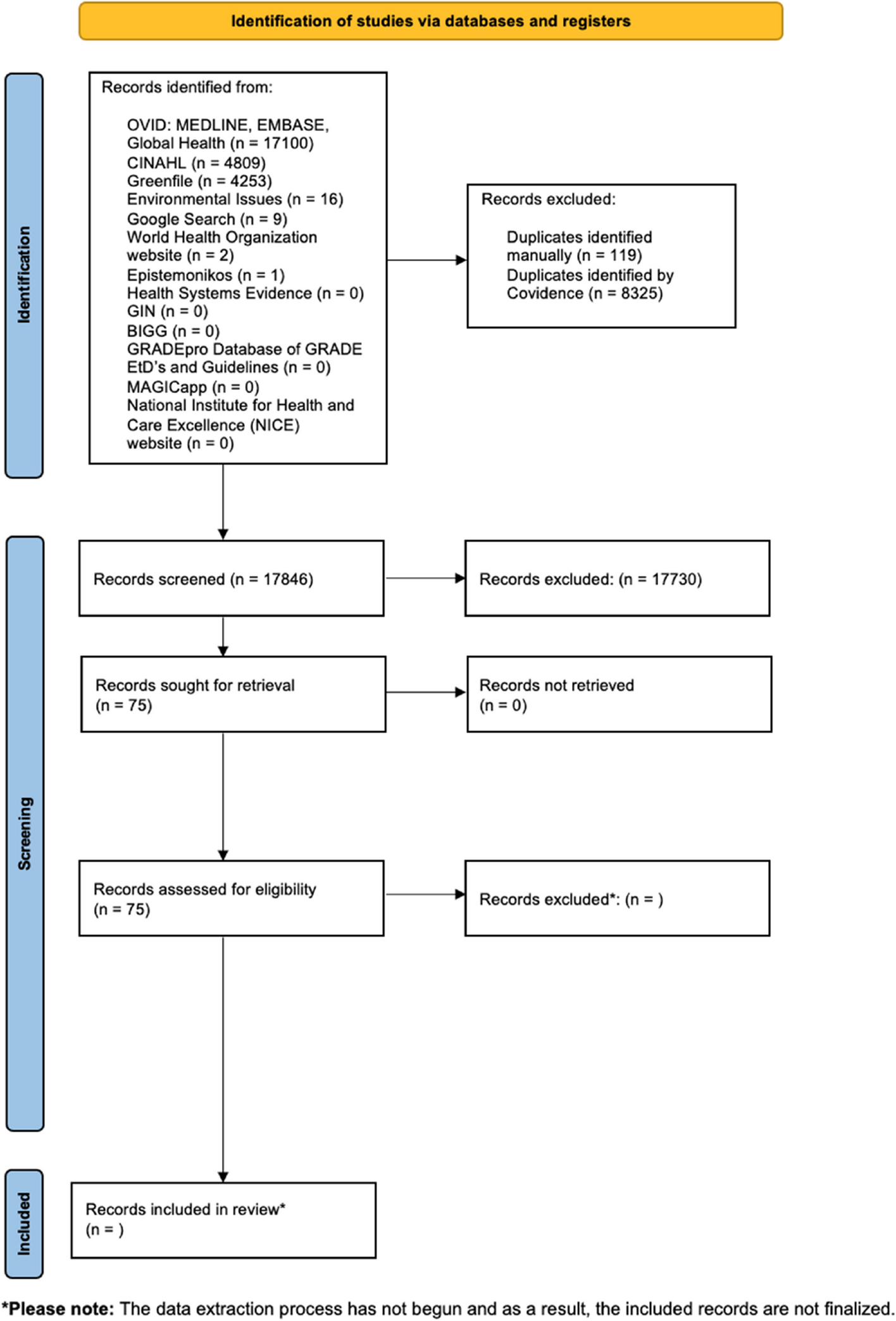
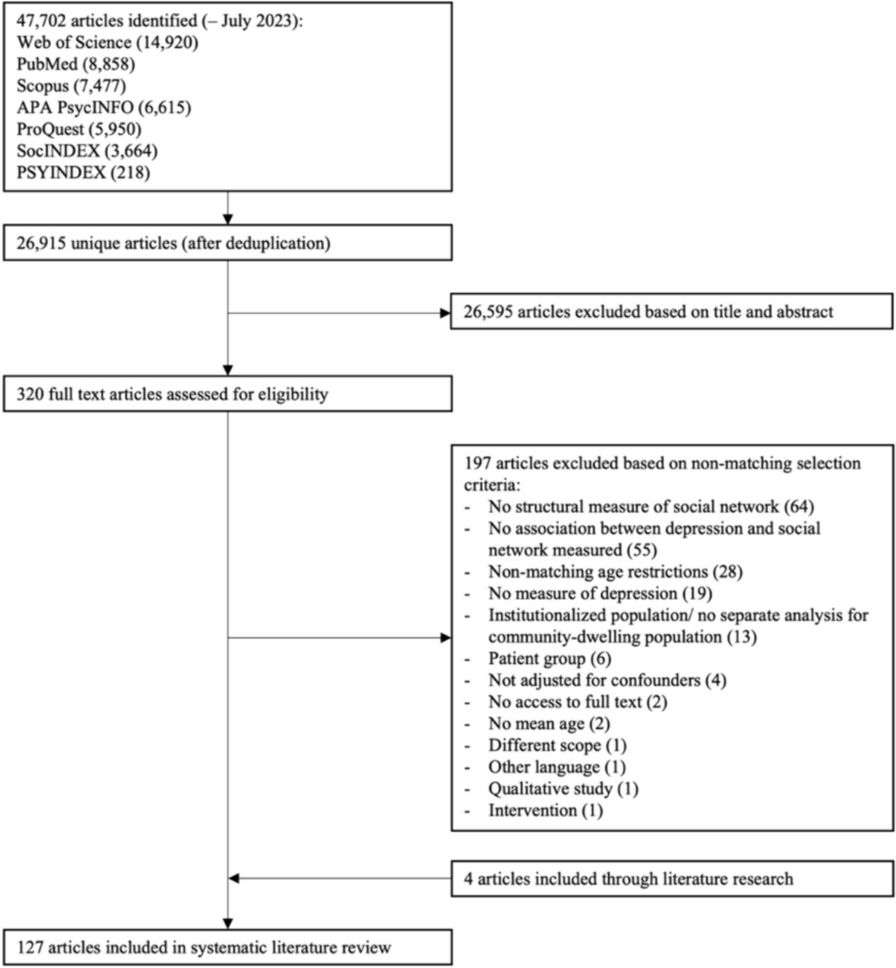




Our database searches retrieved 5673 unique citations. Nine citations were found from grey literature sources, all of which were ineligible for inclusion. After reviewing 907 full texts from these searches, 862 studies were excluded for reasons (Supplementary file 1). 428 records were screened from seven existing systematic reviews, our previous review’s excluded studies list, and stakeholder submissions. All of the eligible studies submitted by stakeholders were also found in our searches. Overall, we included 82 studies with five additional associated publications (Figure 1); 28 of these were included in the previous review. One of the previously included studies was excluded because more than 20% of the participants were below 35 years of age which was a revised criterion for this update [26].
Fig. 1 Health state utility valuesStudy characteristics
Health state utility valuesStudy characteristicsFor HSUVs, we included 38 studies [27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64] and one associate paper [65]. The mean age across studies was 56.7 years (≥ 70 years in 4 studies [27, 46, 53, 57]), and the total number of participants was 22,952 (range 30 to 8287). Studies came from the Netherlands [31, 39,40,41,42,43, 59], the USA [27, 28, 37, 55, 57, 60], South Korea [38, 44, 49, 61], Finland [51, 52, 54, 65], the UK [36, 53, 62], Australia [29, 34, 63], Japan [33, 58], Spain [45, 47], Norway [48], Italy [50], Croatia [64], Thailand [56], France [35], Greece [32], England and Wales [46], and multiple countries (UK, USA, Japan, France, Germany, Italy, and Spain) [30]. Other demographic information including race/ethnicity, comorbidities, and family history was scarce and not consistently reported. Of seven studies reporting on race/ethnicity, the percent of non-Caucasian/White participants was 0.8 to 60.7%. Recruitment strategies usually included cancer networks/centers or outpatient clinics.
Thirty studies used the EQ-5D index score with patient samples and three of four studies using direct methods (TTO and SG) used vignettes with a public sample (see Supplementary file 2 for details). One study using the EQ-5D visual analogue scale (VAS) in a public sample was included in a post hoc manner to assess the utility of interval breast cancers as this health state was not reported in any of the other included studies.
Thirteen (34.2%) of the 38 studies were at high risk of bias for at least one timepoint of interest. Nine studies solely focused on screening health states, 25 were focused on treatment health states, and four studies included health states on both screening and treatment.
Table 2 summarizes the main findings and their certainty from the primary analysis of HSUVs relying on the utility-based HRQOL tools and supported by TTO and SG findings where available. Supplementary file 2 contains tables of the study characteristics, the risk of bias ratings, and a full summary of findings tables which include all findings from the main, sensitivity, and subgroup analyses. Detailed results are presented here when the evidence was rated to have low or higher certainty.
Table 2 Summary of findings on health state utilitiesScreening health statesDisutilities from outcomes during the breast cancer screening process were calculated in comparison with (subtracted from) the pooled utility (0.94) of a healthy screen-eligible population including individuals scheduled for genetic counseling (n = 33; results of genetic testing unknown), with a known negative screening result (n = 531), and healthy age and education matched comparators (n = 7992) [60, 61, 64]. This estimate had moderate certainty due to a lack of consistency from large reliance on one study [61]. When comparing results with trends observed in population norms (not all eligible for screening) for a Canadian province (Alberta) [66], we had low certainty (from indirectness to older ages) that the utility of 0.94 applies well to those over 70 years of age.
During the breast cancer screening process, the disutility of positive screening mammography (before diagnostic testing) is probably 0.07, with a rating down one level for some concerns of inconsistency and risk of bias [32, 59, 60]. Two of the studies excluded people who were later known to have cancer and the other only included women who’s screening mammography indicated low suspicion for breast cancer. After receiving imaging only or imaging plus biopsy and results of no cancer diagnosis, the disutility of knowing about a FP result may be 0.03 to 0.04 [59, 60].
The disutility of a true-positive result (screen-detected cancer) is probably on average 0.08, but may be higher for older ages and advanced stage operable breast cancer [31, 35, 44,45,46, 52, 53, 61, 64]. Removing two studies at high risk of bias did not impact the findings. There were some concerns about unexplained inconsistency; subgroup data based on age and stage of disease (including data from a SG; n = 156 [55]) was limited but suggested higher disutility with older ages and advanced-stage operable disease. There was also some indirectness because data were not specific to screen-detected cases, though concerns were not serious because the seven studies that reported stage of disease confirmed there were very few stage IV (0–0.7%) cancers which are not typically identified during screening.
Interval cancers were reported in one study using a hypothetical scenario and evaluated by VAS, where the disutility may be similar to screen-detected cancer (n = 131; low certainty) [28].
Treatment health states < 12 months from surgeryUtility values within 12 months from surgery for breast cancer were compared across different surgeries and different adjuvant therapies, to estimate the disutility of one treatment versus another. The disutility of mastectomy versus a BCS/partial mastectomy where all patients are receiving adjuvant therapy may be at least 0.02 to 0.03 [27, 29, 33, 47, 49, 52, 61,62,63]. The range in disutility values comes from the within-study estimate of 0.03 and the between-study estimate of 0.02 [mastectomy HSUV 0.80 vs. BCS 0.82]. All studies had at least 20% of patients receiving adjuvant therapies. Concerns included the risk of bias and unexplained inconsistency based on the types of adjuvant therapies received as well as an indication from direct measurements (in public samples) that the disutility may be higher (0.05 to 0.10) [29, 39, 56]. When looking at findings among subgroups where patients were all receiving chemotherapy or all receiving radiation therapy, thus controlling for these variables, the disutility of a mastectomy versus BCS was higher (0.04 to 0.08) but findings were limited by few studies. We are very uncertain about a major comparison of interest which was mastectomy without adjuvant therapy (no evidence) versus BCS/partial mastectomy with adjuvant radiation (a choice often provided for small node-negative estrogen-receptor-positive breast cancer, a common cancer found by screening).
The disutility of adjuvant chemotherapy versus no chemotherapy may be 0.02 to 0.04 among a mixed surgical population within 1 year from surgery, due to concerns of inconsistency and indirectness from reliance for our estimate on between-study comparison data [
留言 (0)