
記住我
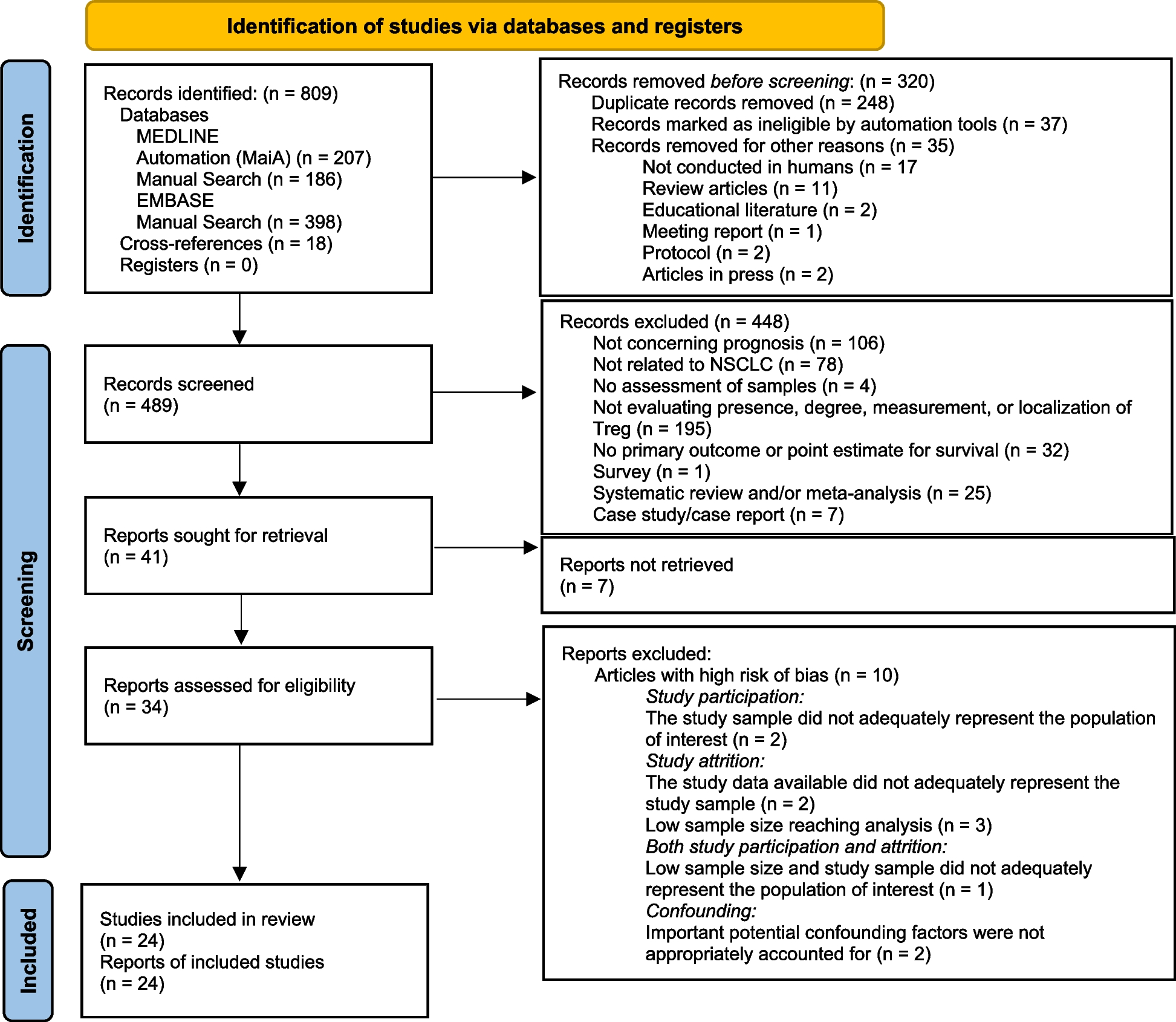
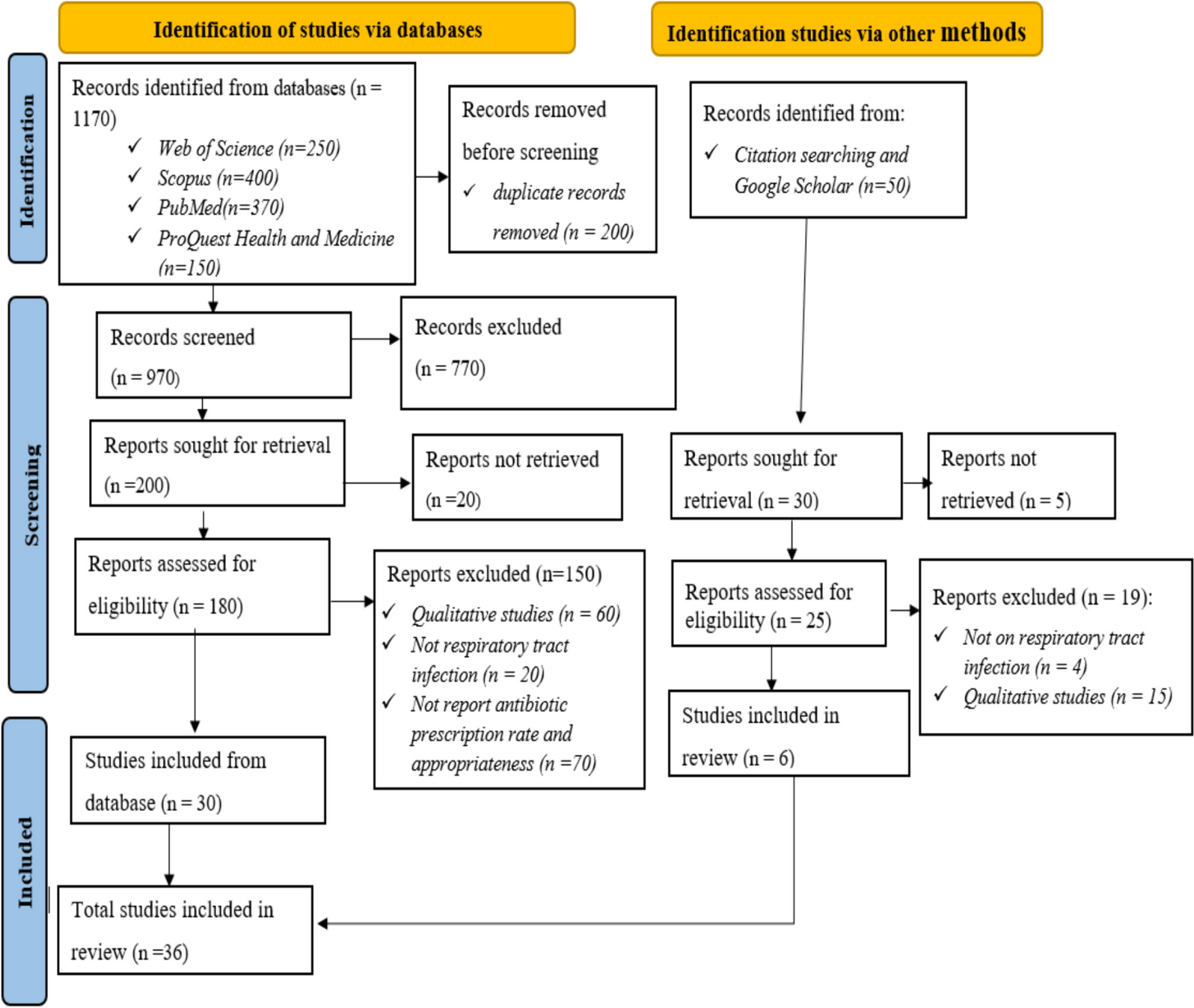
The search yielded 6620 studies. After removing duplicates, 5087 titles and abstracts were screened. Only 173 studies were assessed in full text, and 62 studies were finally included in the review (Fig. 1). The 62 studies included comprised 40 qualitative studies, 16 quantitative studies, and six studies using mixed methods. Characteristics of each included study are available in Table 2. In the mixed methods studies, factors affecting communication were found in the quantitative part of one study [24], the qualitative part of three studies [25,26,27] and in both parts of two studies [28, 29]. The year of publication ranged from 1990 to 2023 (Fig. 2). The studies were performed in eight countries, with Sweden as the main contributor, accounting for 47% of the studies (Fig. 3). The primary data sources for the qualitative studies comprised interviews with either the operator or the caller. Additionally, open-ended survey questions and audio recordings of interactions between operators and callers were employed. In the case of quantitative studies, the predominant data sources were surveys and audio recordings. Out of all the studies, the operator’s view was explored in 28 studies, and the caller’s view in 18, while the remaining 16 studies explored both viewpoints. Altogether, 13 factors were identified and categorised into four main groups: organisational factors, factors related to the operator, factors related to the caller and factors in the interaction. Additional core elements describing each factor were also identified. An overview of the main themes, factors and core elements is presented in Table 3.
Fig. 1 Table 2 Key information about the included studies (N = 62)Fig. 2
Table 2 Key information about the included studies (N = 62)Fig. 2
Year of publication of the studies (N = 62)
Fig. 3
Country in which the studies (N = 62) were performed
Table 3 Overview of factors and core elements belonging to each main themeQualitative findingsOrganisational factorsThe organisational theme contained three factors: availability, working conditions, and decision support systems.
AvailabilityThe availability of the service affected the communication. Queuing and waiting to get through to the operator were described by both callers and operators as negatively affecting communication [27, 30,31,32,33]. Callers found the uncertainty of the waiting time frustrating, which could make them irritated and angry, requiring operators to spend extra time to calm them down [27, 30,31,32].
When operator resources did not correspond to needs, the queues of callers increased and the operators reported a high level of stress [9, 27, 31, 32, 34,35,36]. The operators communicated faster and more mechanically, which could lead to quick decisions being made based on little information [27, 31, 32, 34,35,36,37,38]. Time to express their needs was highlighted as important for the callers [39, 40]. Sufficient operator resources also allowed for collaboration with other colleagues to discuss difficult issues [8, 9, 27, 35], which increased operators’ self-confidence [41] and callers’ faith in the advice given [39, 42, 43].
The operators’ ability to make decisions during the conversation was affected by shortages of other resources, such as doctors on call, ambulances and mental health services [9, 27, 31, 32, 34, 37, 44, 45]. When a shortage of resources, the operators had to spend time on explaining the lack of available resources [31, 32].
Working conditionsThe construction of the workspace was described as influencing communication [31, 41]. The opportunity to move and stretch helped the operators to concentrate better [31], and proximity between the operators’ workspaces allowed for collaboration [41].
Organisational attitudes affected how rigidly the operators used guidelines [31, 35, 46,47,48]. If the employer had high-efficiency expectations, the operators felt they were monitored and described the same effect as we found under lack of operator resources: less time for good communication [9, 32, 34, 45]. The organisation of work shifts could reduce the quality of communication, due to physical and psychological limitations during long shifts or night shifts [35, 37, 47].
Technology, such as the use of video, could clarify or prevent misunderstandings [28]. However, multitasking between different technical aids while gathering and interpreting information from the callers was described as cognitively demanding [35, 48, 49]. Beginners spent most of their cognitive capacity on technology, which suppressed the use of their own medical knowledge and communication skills [35]. Technical failure caused problems with focusing, stress and a lack of control, which led to disruptions in the conversation [27, 31, 34, 45, 50, 51].
Decision support systemsDecision support systems (DSS) were described by the operators as ensuring quality by giving structure to the conversations, providing evidence-based knowledge, and being a checklist for important questions when the operators’ own clinical knowledge and experience were limited [8, 41, 48, 50, 52]. Also, callers were more receptive to advice when informed that it came from the DSS [36, 48, 50].
However, DSS structured the conversation in a way that deviated from normal conversations, particularly when operators followed a DSS with a fixed checklist structure [49, 53, 54] that used standardised sentences and closed yes/no questions [54, 55]. Consequently, this restricted the caller’s provision of a detailed description of the situation and made the operators convert all reasons for calling into a problem that suited the system [54]. The operators described feeling controlled, directed, passive and less attentive to the callers when using a fixed checklist structure [50, 56]. The callers described the operators’ use of checklists as frustrating and impersonal, due to an increased number of questions that sometimes seemed irrelevant [38, 57, 58]. If the DSS lacked information, was non-intuitive or used medical terminology, the operators spent time searching the tool or translating words into everyday language, which led to pauses in the conversation [49,50,51]. In contrast, the operators’ attention was notably more oriented to the ongoing conversation when they did not use DSS [53].
Factors related to the operatorFactors related to the operator comprised three categories: knowledge and experience, personal qualities, and communication strategies.
Knowledge and experienceSufficient medical knowledge was described by the operators as essential for asking the right questions and being confident when gathering information and making decisions [32, 47]. Similarly, the operators’ organisational knowledge was described as a basis for decisions and thereby also the information conveyed to the callers [8, 9]. Callers described greater trust when they spoke to operators who were more competent than themselves [7, 33, 39, 42].
During calls, operators used personal and professional experience to assess symptoms and problems. This influenced the questions asked, the operators’ perception of the situation and the advice given [34]. As they became more experienced, operators developed tacit knowledge and the ability to visualise the patient’s situation. Tacit knowledge was explained as intuition or a gut feeling, which made the operators able to read between the lines and catch information that was not verbalised [8, 27, 31, 37, 58,59,60]. Visualisation was described as crafting a mental image of the patient’s circumstances and served as a means of promoting understanding [
留言 (0)