
記住我
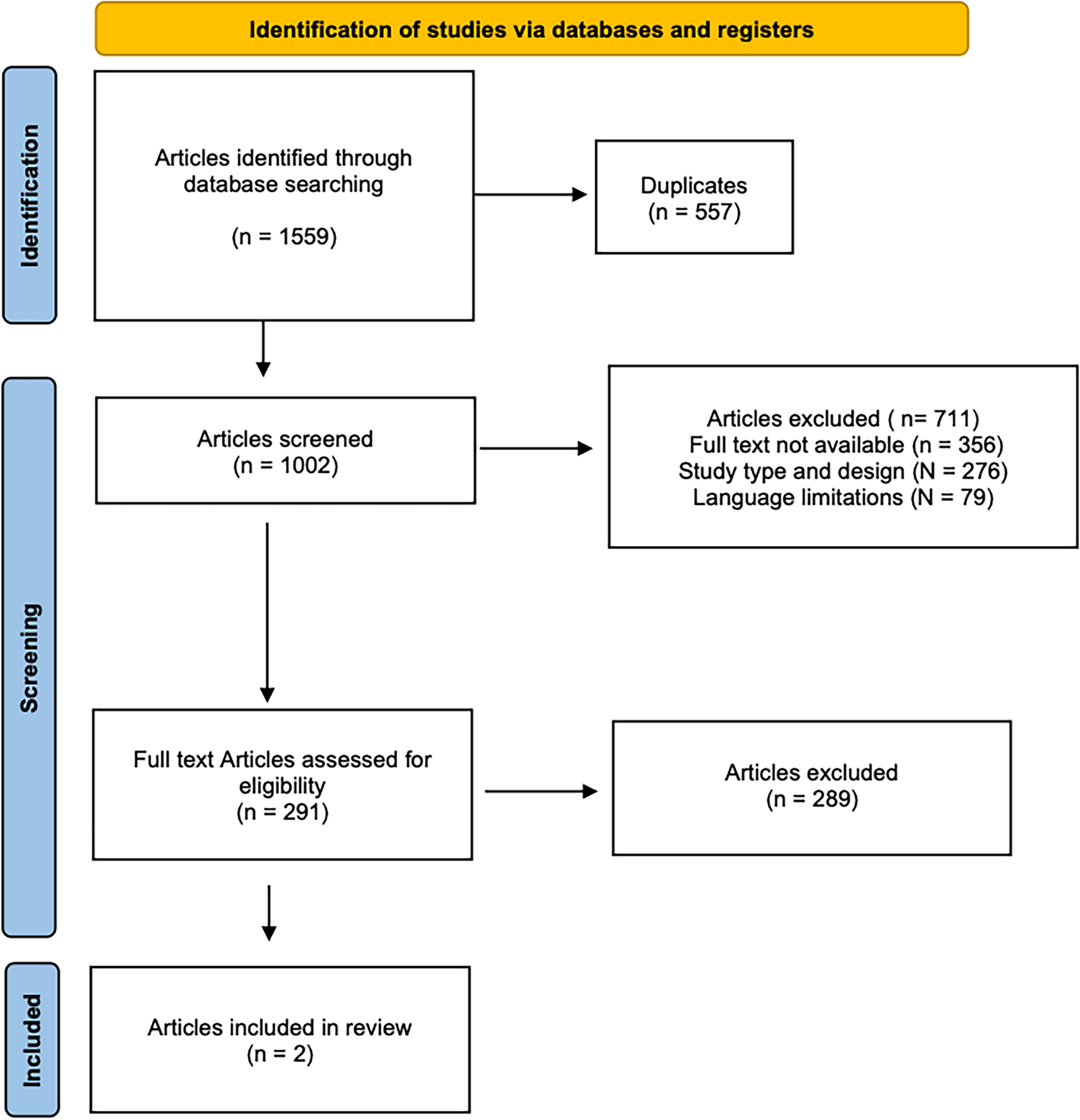

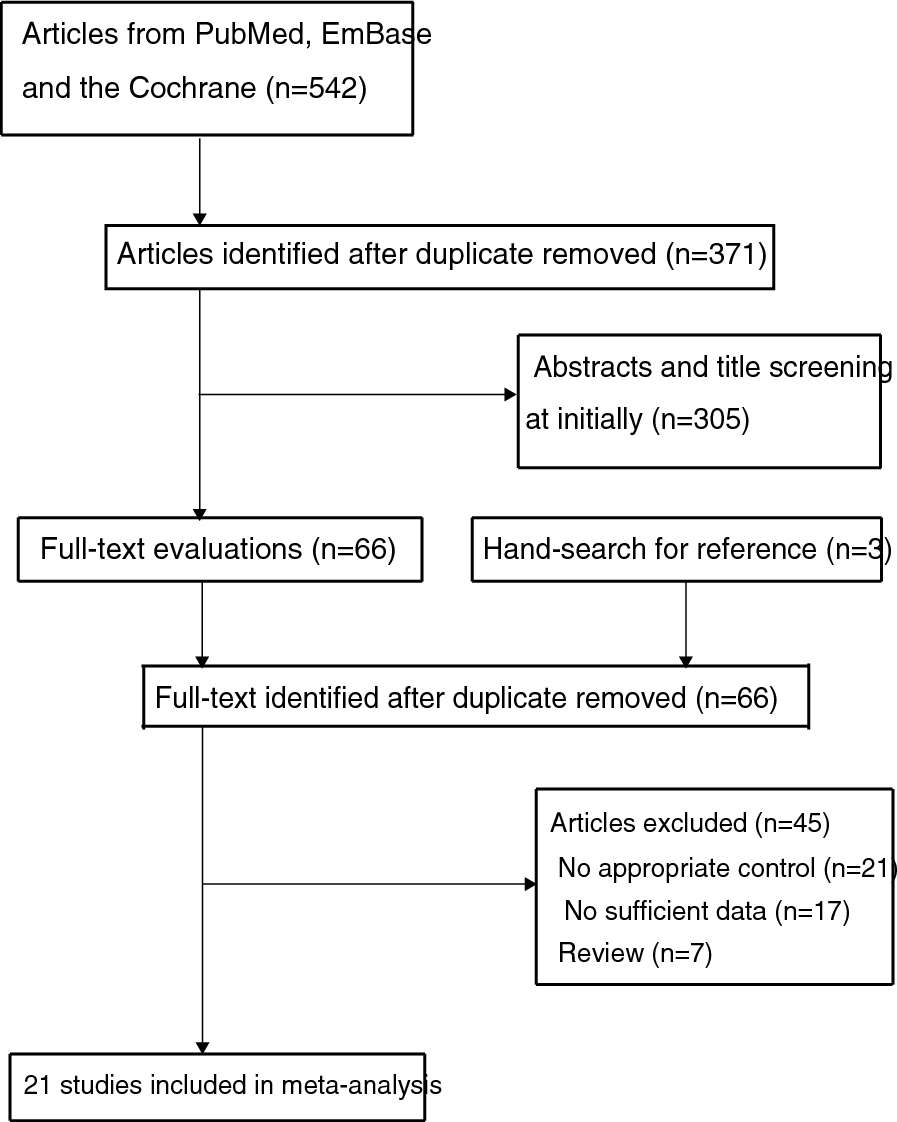



This scoping review was conducted in accordance with the guidance described in the Cochrane Handbook of Systematic Reviews. A search of the relevant electronic databases (Ovid, Medline and PubMed) was conducted using keywords relating to MSC or marrow aspirate in bone-healing applications. Articles were identified through the screening of titles and abstracts, with full texts retrieved for those articles relevant to this study.
Inclusion criteria included all studies published in the English language since 2010 that assessed the use of progenitor cells or marrow aspirate for the augmentation of bone healing. Once identified, data were extracted, including the condition treated, the product used (culture-expanded cells vs marrow aspirate), supplementary therapy, duration of follow-up, and both radiological and clinical outcomes. These data are summarised in Tables 1–10.
Table 1 Papers assessing the use of cell therapies in acute fracture careMSCs in acute fracture healingGiven their key role in osteogenic differentiation and the control of the local paracrine environment, direct implantation of MSCs into acute fractures has been an area of particular interest (Tables 1 and 2). Osteoporotic vertebral fractures are endemic and can lead to significant pain and disability [23]. To try and improve outcomes in this cohort, Shim et al. performed both local and systemic injection of Wharton-jelly-derived MSCs in combination with systemic administration of the synthetic parathyroid hormone (PTH) teriparatide [24]. Compared to teriparatide therapy alone, the experimental group demonstrated significantly improved pain scores, Oswestry disability index scores, and bone microarchitecture on CT at both 6 and 12 months. A number of authors suggest injecting MSCs in the early period following fracture fixation in an attempt to accelerate bone healing and facilitate a return to normal function. Liebergall et al. injected flow-selected MSCs into acute tibial fractures at between 3 and 6 weeks post-operatively and noted a reduction in the time to union of nearly half [25]. Similarly, Kim et al. examined the injection of cultured osteoblastic cells into a number of long-bone fractures (mostly tibias and femurs) at 6 to 8 weeks following the index procedure and also noted a significantly faster rate of radiological healing compared to standard treatment [26].
Table 2 Outcomes following the use of cell therapies for acute fracture careContrastingly, not all acute fractures appear to be associated with such positive results. Due to a retrograde blood supply, femoral neck fractures are associated with high rates of both nonunion and avascular necrosis (AVN) [27]. Verma et al. therefore attempted to improve outcomes through the application of bone marrow aspirate to the hip in young patients undergoing cannulated screw fixation of a displaced femoral neck fracture [28]. They demonstrated no difference in the rate of nonunion, AVN or Harris hip score at final follow-up, though it is worth noting that this injection was into the hip joint, with no way of discerning exactly where the cells would seed. Similarly, Seebach et al. examined the use of culture-expanded MSCs on β-TCP scaffolds following locking-plate fixation of proximal humeral fractures [29]. Whilst they were able to achieve healing in all patients by 12 weeks, functional outcomes as measured by the disabilities of the arm, shoulder and hand (DASH) score were poor when compared to comparable series [30].
MSCs in fracture nonunionFracture nonunion represents a complex problem, the key to which is disruption to the bone’s normal healing mechanisms. Definitions vary, with the Food and Drug Administration (FDA) defining a nonunion as a fracture that has not gone on to heal 9 months following injury, with no radiological evidence of progression of healing for 3 consecutive months [31]. A more pragmatic definition is that of a fracture that has not gone on to heal within the usual timeframe of the injury and, in the opinion of the treating clinician, will not go on to heal without further intervention [32]. Fracture nonunion occurs due to complex interplay between biology and mechanics. Historically, it was felt that atrophic nonunion occurs due to inadequate biology and hypertrophic nonunion due to inappropriate mechanics; however, increasingly, it is becoming evident that this is not the case, with each nonunion requiring careful assessment to ascertain which aspect of the diamond concept is not being supported [33]. Where surgeons aim to augment the biology, autologous bone graft remains the gold standard as a source of osteoconductivity, osteoinductivity and osteogenic cells. MSCs are, however, lost in the process of harvesting and preparing autograft, and, as such, augmentation with MSCs can be utilised to optimise the osteogenic stimulus (Tables 3 and 4) [15].
Table 3 Papers assessing the use of cell therapy in nonunionTable 4 Outcomes following the use of cell therapies for nonunionIn its simplest form, as a source of MSCs, marrow aspirate can be injected directly into the nonunion site [34]. Using this technique, Singh et al. achieved union in 10/12 patients that they treated with percutaneous bone marrow aspirate delivery into long-bone nonunion [35]. Hau et al. also employed marrow aspirate laden onto freeze-dried allograft as a carrier in their cohort of long-bone nonunions (nine of the femur, six of the tibia, two of the ulna and one of the humerus) [36]. Even when compared to the gold standard of autologous bone graft, they saw accelerated bone healing with marrow aspirate, reducing the average time to union by 28%. Figure 2 demonstrates the percutaneous application of bone marrow aspirate to a tibial nonunion, whereas Fig. 3 shows the percutaneous application of bone marrow aspirate to a femoral nonunion.
Fig. 2
A 42-year-old male sustained a closed distal tibial fracture following a fall (A, B). The fracture was stabilised with a MIPO plate and demonstrated little callus formation 6 weeks after surgery (C, D). A CT scan taken at 6 months demonstrates an established nonunion (E). The patient underwent the harvesting of 60 ml bone marrow from the ipsilateral iliac crest, which was concentrated down to 7 ml of BMAC. This was injected by a percutaneous technique into the nonunion site (F, G). Following this technique, union was achieved within 4 months (H, I). MIPO Minimal invasive plate osteosynthesis
Fig. 3
A 30-year-old female presented a CT-proven atrophic nonunion at 9 months following an IM nail for a closed femoral fracture (A, B). The patient underwent the harvesting of 60 ml of bone marrow, which was concentrated down to 8 ml volume and injected into the nonunion site (C, D). Images E and F demonstrate union at 3 months post-operation. IM Intramedullary
Culture-expanded MSCs, whilst more resource intensive, are beneficial in the management of fracture nonunion. Emadedin et al. injected culture-expanded MSCs into three femoral and two tibial nonunions, achieving radiological union in 3/5 cases [37]. In their series of three patients with tibial/femoral nonunion, Wittig et al. achieved a 100% union rate within 12 months following the injection of culture-expanded MSCs seeded onto collagen microspheres as an osteoconductive scaffold [38]. Similarly, Giannotti et al. loaded culture-expanded MSCs onto fibrin clot scaffolds augmented with autologous or synthetic bone graft in the management of eight patients with forearm and humeral nonunion. They were able to achieve union in 8/9 patients without further intervention by adopting this strategy [39]. Ismail et al. compared culture-expanded MSCs loaded on hydroxyapatite granules with autologous bone graft in ten patients with long-bone nonunion [40]. Even against the current gold standard, union was achieved significantly faster when using MSCs on a scaffold, with greater functional improvements also achieved in the first 4 months post-surgery. Finally, Gomez-Barrena et al. seeded culture-expanded MSCs on 20% hydroxyapatide/80% β-TCP scaffolds in 28 patients with long-bone nonunion [41]. They achieved union in 26/28 patients at 12 months, with excellent clinical outcomes.
With concerns about potential donor-site morbidity, the use of allogenic MSCs remains an option, though they also have associated concerns regarding disease transmission and immunogenicity. To investigate the role of allogenic MSCs, Jayankura et al. percutaneously injected allogenic MSCs (ALLOB, Bone Therapeutics) into 22 patients with long-bone nonunion [42]. Using this technique, they achieved union in 20/22 patients at 6 months, although they did note increased in anti-human leukocyte antigen antibodies in 23% of patients, albeit with no clinical hypersensitivity reactions. At present, the literature is limited with regards to allogenic MSCs, and therefore they should be used with caution, particularly when repeated doses are being considered [43].
MSCs in bone defectsAs with nonunion, bone defects are difficult to manage, as they require osteogenic cells, osteoinductive mediators and, importantly, an appropriate osteoconductive scaffold to bridge the existing gap until union is achieved. Current techniques for managing bone defects include bone transport, which takes advantage of the tension-stress principle (whereby continuous tensile stress results in callus as two bone segments are gradually moved away from one another) or bone grafting, be that acute or via a two-stage induced-membrane technique. Both of these techniques, whilst effective, carry high morbidity, both during and following treatment. As such, there is still interest in generating additional osteogenic stimulus in the management of bone defects to accelerate bone healing (Tables 5 and 6).
Table 5 Papers assessing the use of cell therapy in the management of bone defectsTable 6 Outcomes following the use of cell therapies for the management of bone defectsDealing with smaller alveolar cleft defects within reconstructive dentistry, both Shabaan et al. and Bajestan et al. employed cell therapies to try and reduce a defect size prior to siting implants [44, 45]. Shabaan utilised marrow aspiration, whilst Bajestan utilised culture-expanded MSCs on β-TCP scaffolds. Shabaan demonstrated significantly higher bone density with the use of MSCs when compared to bone graft alone; however, Bajestan noted that the use of MSCs with a synthetic bone substitute resulted in inadequate defect reconstruction compared to bone graft and was unable to site an implant in half of the cases.
Sponer et al. utilised culture expanded MSCs on β-TCP scaffolds and compared this to allograft in the management of proximal femoral bone defects following revision arthroplasty [46]. In the 19 patients managed with cell therapy, they noted similar graft incorporation at 1 year and no difference in the Harris hip score, suggesting that cell therapy could be safely used as an alternative to allograft, avoiding the risks of contamination or immunogenicity. Dufrane et al. utilised culture-expanded MSCs combined with DBM to facilitate the incorporation of intercalary replacement following bone tumour resection and resection of pseudoarthrosis, and they demonstrated excellent incorporation around the tumour prosthesis but poor outcomes with a high rate of failure (2/3) when utilised to reconstruct defects in pseudoarthrosis [47].
In the field of trauma, Marcacci et al. utilised culture-expanded MSCs combined with hydroxyapatite scaffolds to manage long-bone defects in four patients (average defect size: 5.25 cm; two ulna, one tibia, one humerus) [48]. All four cases achieved consolidation within 7 months of the procedure, with no reported complications. Similarly, Utomo et al. reconstructed one tibial (6 cm) and one humeral (5 cm) defect combining bone marrow aspirate with freeze-dried allograft and platelet-rich plasma, achieving union with good functional results in both cases [49]. The literature surrounding cell therapies in the management of bone defects is limited, and they are often used in conjunction with other techniques. The addition of an osteogenic stimulus does appear to provide a benefit, particularly in cases where this is combined with bone graft, although further larger series are required to demonstrate this.
MSCs in avascular necrosis of the femoral headAvascular necrosis (AVN) of the femoral head occurs as a result of disruption to the blood supply, which leads to osteocyte death. It may occur spontaneously, following trauma, or due to risk factors such as corticosteroid use or alcoholism [50]. Early AVN is often an incidental finding on a magnetic resonance imaging (MRI) scan, with the disease progressing to femoral head sclerosis, subchondral fracture and, eventually, femoral head collapse. In its early stages, management is based on joint-preserving procedures, including core decompression, vascularised graft or re-directional osteotomies. Once femoral head collapse occurs, joint-preserving procedures become ineffective, and arthroplasty becomes the treatment option of choice [50]. In the setting of AVN, cell therapies provide an exciting avenue to regenerate subchondral bone, preventing femoral head collapse and therefore the requirement for future arthroplasty (Tables 7 and 8).
Table 7 Papers assessing the use of cell therapy in the management of avascular necrosis of the femoral headTable 8 Outcomes following the use of cell therapies for the management of avascular necrosis of the femoral headMSCs can be delivered to the femoral head via several mechanisms, including injection into the local circulation, percutaneous injection into the offending lesion, or application on scaffolds following core decompression. Three recent studies have examined the use of local injection of MSCs for femoral head AVN. Chen et al. injected umbilical cord MSCs into the femoral artery in nine patients with stage 2 and stage 3 AVN [51]. In all patients, the AVN lesion remained stable over 24 months of follow-up, with no patient requiring conversion to total hip arthroplasty (THA). Mao et al. similarly injected bone-marrow-derived mononuclear cells into the medial circumflex artery in 78 patients with grade 1–3 AVN, and they demonstrated that there was little progression in stage 1 and 2 hips at 5 years and a requirement for THA in just 7.7% across all stages [52]. Two years later, the same group also published their results on porous tantalum rod insertion ± infusion of peripheral blood stem cells into the medial circumflex femoral artery, demonstrating that there was an improved radiological and clinical outcome in the infusion group at 36 months [53]. Within this cohort, the requirement for THA was reduced from 22% in the control group to 6% in the infusion group. A number of authors have also examined the injection of cells only into the necrotic lesion. Dalto et al. injected minimally manipulated bone marrow into the hips of 89 patients with stage 1 and 2 disease; they demonstrated that lesions were stable in all patients at 5 years and that there were no conversions to THA [54]. Li et al. obtained similar results at a year following the injection of bone marrow, adipose-derived stem cells and PRP [55].
Decompression is a key feature of the early management of AVN. A number of authors have applied marrow or expanded MSCs following decompression to try and stimulate healing in the subchondral area. Hauzer et al. compared core decompression with bone marrow aspirate concentrate (BMAC) injection to core decompression and saline, demonstrating that there was no difference between the two groups with regards to radiological progression, clinical outcomes or need for THA [56]. It should be noted, however, that all patients in this cohort had stage 3 disease. Gao et al. similarly injected marrow aspirate supplemented with recombinant bone morphogenetic protein-2 (rhBMP-2) into adolescent patients following core decompression, achieving good clinical outcomes for 96% and 83% of stage 1 and stage 2 hips, respectively, at 6.8 years [57]. Outcomes were poorer for stage 3 hips, with only 67% achieving a good outcome; however, only one patient had proceeded to THA. Hauzer et al. also examined the use of expanded osteoblastic cells vs BMAC in patients undergoing core decompression for stage 1 and 2 AVN [58]. Outcomes were significantly better with culture-expanded cells, with fewer demonstrating radiological progression and just 15% requiring THA, compared to 35% in the BMAC group.
To further provide osteoconductivity, various authors have utilised both native and synthetic material as scaffolds to try and further improve the bone healing response. Li et al. combined bone marrow buffy coat with an angioconductive bioceramic rod and compared this to a control of β-TCP granules without marrow [59]. Within this cohort, patients managed with bone marrow had significantly higher Harris hip scores at 5 years (84 vs 73) and a significantly lower conversion rate to THA (4.5% vs 17.2%). Aoyama examined the use of culture-expanded MSCs seeded on β-TCP scaffolds combined with vascularised iliac crest graft in nine patients with stage 3 disease [60]. At 2 years, all patients remained functionally high-performing, with no radiological progression and no conversions to THA. Both Li et al. and Zhao et al. examined the combination of culture-expanded MSCs with bone graft [61, 62]. In a 10-year follow-up of core decompression, bone graft ± BMAC, Li established that the addition of marrow reduced radiological progression from 50 to 24%, produced significantly better functional outcomes, and reduced the requirement for arthroplasty from 20% to just 9.5%. Similarly, when treating exclusively stage 3C and 4 hips, Zhao demonstrated that a combination of a porous tantalum rod with culture-expanded MSCs and vascularised iliac crest graft prevented radiological progression in 8/31 hips, with a THA rate of just 16% at 5 years.
Cell therapy is particularly exciting in the management of early AVN, as it demonstrates strong utility in preventing progression beyond stage 1 and 2 disease. Nonetheless, when combined with other gold standard techniques such as autologous bone grafting, it can still provide value, even in advanced disease.
Other applications of MSCsWhilst cell therapies are currently most commonly utilised in the management of AVN and nonunion, they have wide-ranging potential (Tables 9 and 10). Both Di Bella et al. and Li et al. utilised bone marrow for the management of paediatric bone cysts [63, 64]. In both of these series, the addition of bone marrow resulted in improved healing compared to the current standard of management. Lee et al. also demonstrated great efficacy of BMAC during distraction osteogenesis [65]. Injection of BMAC at the time of osteotomy in this cohort of 20 patients undergoing bilateral tibial lengthening over a nail resulted in faster cortical consolidation and a faster return to full weight-bearing. Cell therapies have also been trialled in spinal fusion as an alternative to autologous graft. Unfortunately, however, despite positive clinical outcomes, the nonunion rate was 61%, and therefore their use is not routinely supported for this indication [66].
Table 9 Miscellaneous papers assessing the use of cell therapyTable 10 Outcomes of miscellaneous papers assessing the use of cell therapy
留言 (0)