
記住我


Intravenous (IV) drug administration has been associated with a high risk of medication errors (MEs) and other adverse drug events in hospital settings.1–4 Observational multisite studies have reported a high prevalence of MEs and procedural failures,5,6 while some have estimated that up to 10% of IV medication administrations include an error.4 When compared to other administration routes, it has been found that errors are as much as five times more likely to occur when an IV route is used.3 Moreover, many intravenously administered drugs are high-alert medications, bearing a heightened risk of causing significant patient harm if used in error.7 Consequently, effective interventions to highlight and eliminate IV MEs within the medication management and use (MMU) process are needed to ensure medication safety in hospital settings.8–15
Studies have found preparation and administration errors to be the most common IV ME types, probably due to these phases of the MMU process being the most widely studied.4,16,17 However, the number of IV prescribing errors is likely to be higher as, when also considering other administration routes, prescribing and monitoring are associated with the highest prevalence rates of preventable MEs.18 Wrong administration rate errors have been identified as the most common error type in IV drug administration, followed by the wrong time of administration, and the remaining error types include administration of wrong dose, inputting wrong pump settings, and dose omission.4 When considering error defenses, a systematic review exploring IV preparation errors compared incidence by preparation site and/or method, finding the error incidence to be lower for doses prepared within a central pharmacy versus the nursing ward and lower for automated preparation versus manual preparation.17 In the same study, the error types and reported rates were found to vary substantially.
In 2016, we conducted systematic reviews exploring systemic causes of,19 and systemic defenses to prevent,20 IV MEs. Insufficient actions to secure safe use of IV high-alert medications, lack of knowledge of the drug, calculation tasks, failure in double-checking procedures, and confusion between look-alike sound-alike medications were identified as the leading causes of IV MEs.19 Most studies exploring systemic defenses to prevent IV MEs focused on the administration stage, with smart infusion pumps being the most widely studied systemic defense.20 A limited number of studies explored other stages of the MMU process, which represented a crucial area for future research. Moreover, most of the systemic defenses involved new technological solutions and features related to closed-loop medication management systems. The aim of the present narrative review was to describe the recent evolution of research on systemic causes of, and defenses to prevent, IV MEs in the MMU process in hospitals. A specific emphasis was to investigate whether the research on systemic causes has shifted more toward prospective risk management, and what the phases are of the IV MMU process to which the studied systemic defenses have been integrated.
METHODS Theoretical FrameworkThe theoretical framework of the present narrative review was psychologist James Reason’s (1995, 2000) systems-based risk management theory on preventing human errors, which has been widely applied in patient and medication safety research.12,21–23 In health care, risk management is defined as “clinical and administrative activities undertaken to identify, evaluate, and reduce the risk of injury to patients, staff, and visitors and the risk of loss to the organization itself.”22 These activities or measures aim to prevent, remedy, or mitigate the occurrence or reoccurrence of an actual or potential patient safety event.24 The starting point of the theory is that errors are inevitable when human action is involved, which is why systems relying on perfect performance by individuals to prevent errors are doomed to fail. Hospitals are considered as high-reliability organizations which should introduce safety culture to learn from errors and to implement systemic defenses for ensuring safer care.12,21,23 In recent decades, medication risk management has evolved from retrospective error detection and a person-centered approach toward prospective risk management and a just culture environment, where the accountability of errors is divided between the systems and the individuals.12,21,22,24,25
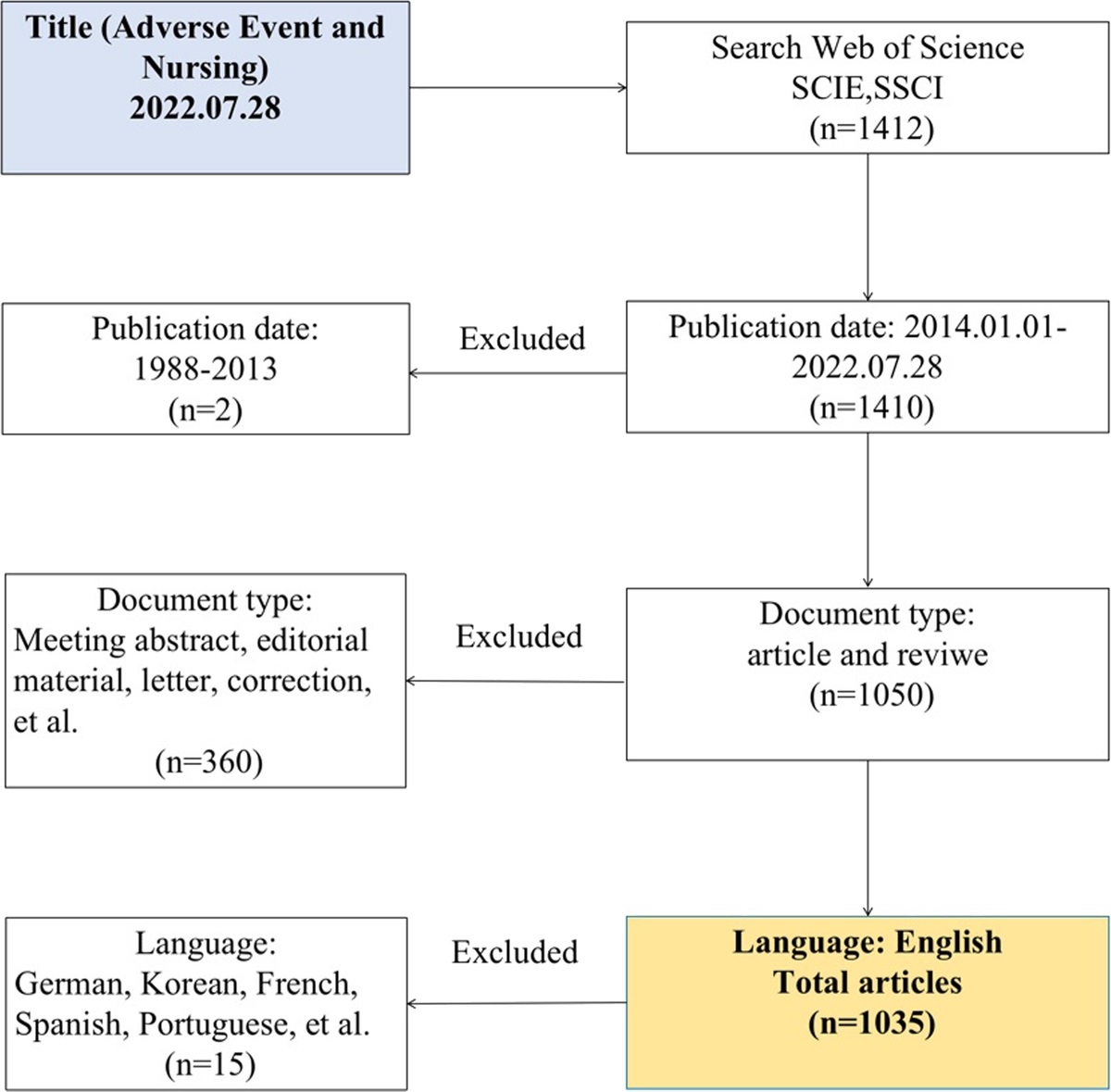
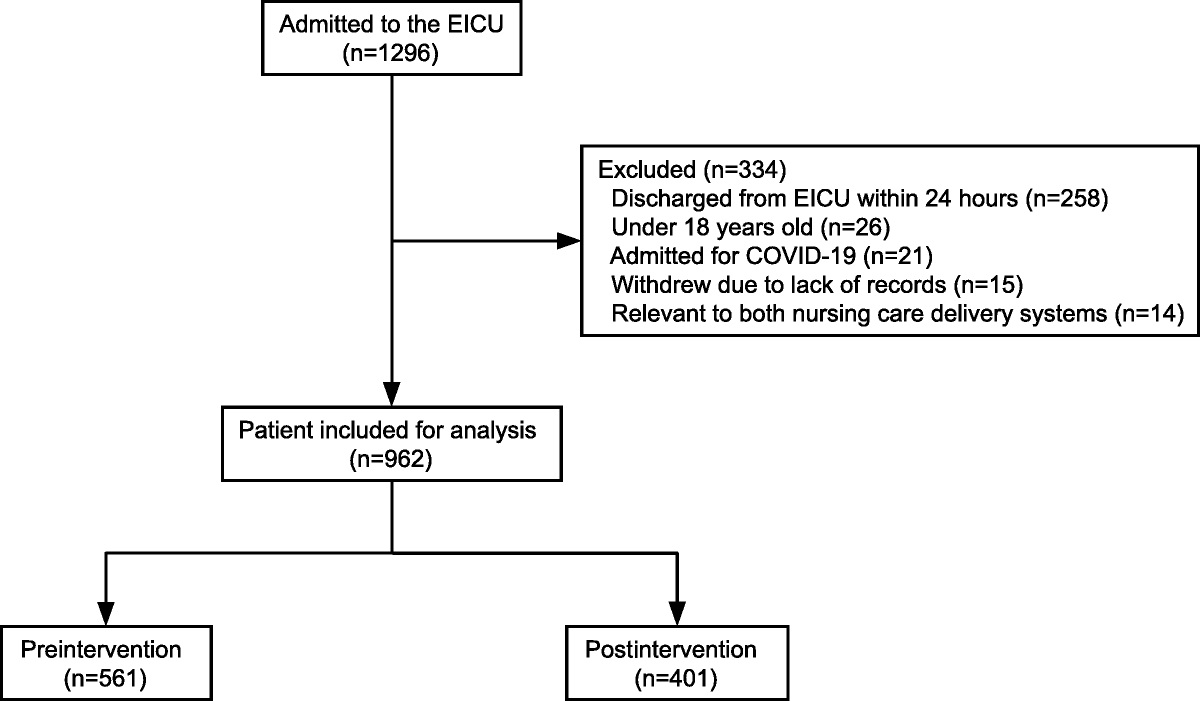
Search Strategy and Study SelectionThis narrative review was carried out according to the Scale for the Assessment of Narrative Review Articles (SANRA), which is a brief critical appraisal tool for the assessment of nonsystematic review articles (Supplementary File 1, https://links.lww.com/JPS/A611).26 A systematic literature search was performed on Medline (Ovid) in October 2021. We used the same search strategy as in our previous publications19,20 to review the most recent evidence. Medline (Ovid) was selected as a source of information as it represents a key database for medication safety research. Studies published within the period from 2016 to October 2021 were included. One reviewer (SK) selected the studies based on titles, abstracts, and full texts (Fig. 1). The PICO tool (participants, interventions, comparison, and outcomes) developed for our earlier publications19,20 was used to select studies for inclusion. The search found 435 articles, of which 63 articles were included in the narrative review.
 FIGURE 1:
FIGURE 1: Flowchart of an updated literature search (conducted in October 2021).
Data Extraction and AnalysisOne author (SK) carried out the data extraction and analysis, and the results were carefully reviewed by the other authors (A-RH, MA). At first, reference, country, study design, setting, and the main results of the included studies were extracted to 2 tables (Supplementary Files 2, https://links.lww.com/JPS/A612, and 3, https://links.lww.com/JPS/A613). After that, a classification and comparison of frequencies were performed to summarize key findings of the articles included in this narrative review (n = 63) (Fig. 2). Finally, the key findings were compared to our previous systematic reviews19,20 to illustrate the evolution of the IV medication MMU process in hospitals.
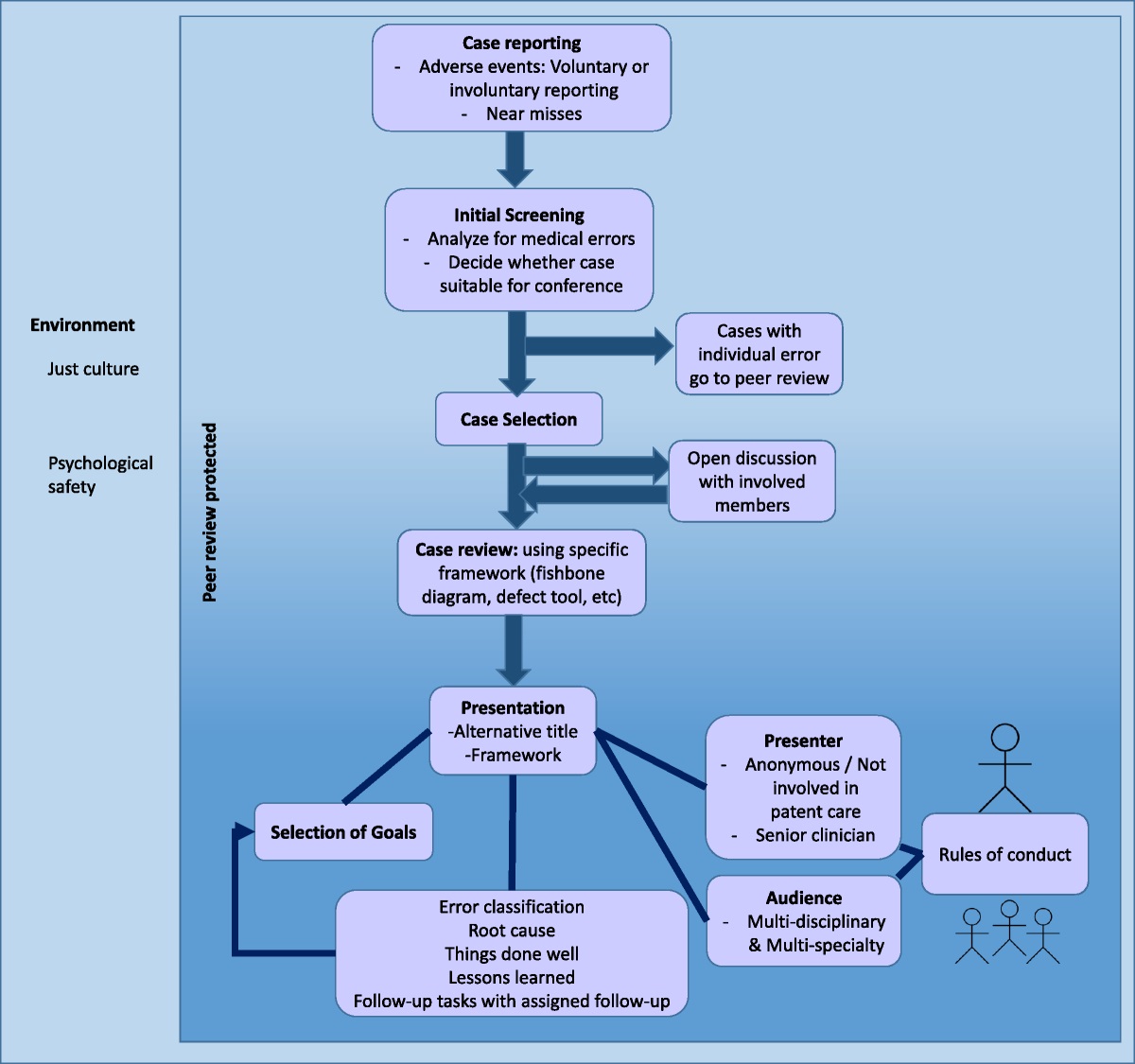
 FIGURE 2: Outline of the narrative review process, analysis of the included articles (n = 63), and comparison to our previous systematic reviews.19,20
FIGURE 2: Outline of the narrative review process, analysis of the included articles (n = 63), and comparison to our previous systematic reviews.19,20The articles on systemic causes of IV MEs (n = 16) were classified according to the stages of the MMU process they focused on (Fig. 2). The study designs employed in the articles were analyzed to recognize whether the studies aimed to identify ME risks prospectively or retrospectively (Fig. 2).12,24 Study designs focusing on learning from previous incidents to minimize similar errors in the future were defined as retrospective risk management (e.g., retrospective analysis of ME reports, observations, and medical records, or interviewing healthcare professionals about MEs they have encountered).12,24,27 On the contrary, studies with a purpose to identify and prevent MEs before they occur were considered as prospective risk-management (accomplished by, e.g., identifying medication safety risks from the literature or by utilizing proactive risk management activities, such as failure mode and effects analysis ((FMEA)) or medication safety self-assessment tools).27–29 The number of studies utilizing a design considered as prospective risk management was compared between our earlier systematic review19 and the present narrative review (Fig. 2).
The articles on systemic defenses to prevent IV MEs (n = 47) were classified according to the MMU process stages they focused on and compared to our earlier systematic review (Fig. 2).20 The evolution of systemic defenses was described using the “Swiss cheese model” comprising a central component of the systems-based risk management theory by James Reason (2000).12 Finally, the main findings related to the most studied medication management technologies within all the included articles were summarized in 2 tables.
RESULTS Description of Studies Exploring Systemic Causes of IV MEs (n = 16)Our systematic search on Medline (Ovid) found 16 articles describing systemic causes of IV MEs published between June 2016 and October 2021 (Supplementary file 2, https://links.lww.com/JPS/A612). These studies were conducted in the following 6 countries: United States (n = 6),6,30–34 United Kingdom (n = 5),35–39 France (n = 2),40,41 Canada (n = 1),42 South Korea (n = 1),43 and Spain (n = 1).44 Most of the studies were carried out in a hospital setting without a specification of a specialty area (n = 7),6,30,31,34,36,37,43 whereas some were conducted in a pediatric hospital setting (n = 3),35,39,41 hospital pharmacy (n = 2),32,42 emergency department (n = 1),33 intensive care unit (ICU) and hematology sterile unit (n = 1),40 neonatal intensive care unit (NICU) (n = 1),44 and a simulated pediatric medical facility (n = 1).38 There was a lot of variation between the study designs and research methods; the most used methods were observation (n = 7)5,6,36,38–40,42 and retrospective analysis of ME reports (n = 2).30,35 Other methods included a systematic review (n = 1),34 analysis of IV compatibility data in literature (n = 1),44 failure mode and effects analysis (FMEA) (n = 1),32 inductive preliminary hazard analysis (PHA) (n = 1),41 retrospective analysis of smart pump alert log data (n = 1),31 retrospective analysis of medical records (n = 1),43 and structured chart and video review (n = 1).33
All studies focused on a specific phase of the IV MMU process (Fig. 3). Most of the studies concerned administration (n = 8, 50%)6,31,33–35,40,41,44 or preparation (n = 6, 38%)32,33,36,39,41,42 phases. Up to 31% (n = 5)32,34,38,41,44 of the studies utilized research designs that could be interpreted as proactive risk management, while in our earlier systematic review19 features of prospective risk management could be identified only in 2 studies (18%).45,46
 FIGURE 3: An overview of the studies focusing on systemic causes of IV MEs (n = 16).6,30–44 The studies are categorized according to the MMU process stages they focused on. Two studies (*) were displayed in 2 categories. Studies aiming to identify ME risks prospectively (n = 5)32,34,38,41,44 are highlighted in red. HRA, human reliability analysis; PCA, patient-controlled analgesia.Description of Studies Exploring Systemic Defenses to Prevent IV MEs (n = 47)
FIGURE 3: An overview of the studies focusing on systemic causes of IV MEs (n = 16).6,30–44 The studies are categorized according to the MMU process stages they focused on. Two studies (*) were displayed in 2 categories. Studies aiming to identify ME risks prospectively (n = 5)32,34,38,41,44 are highlighted in red. HRA, human reliability analysis; PCA, patient-controlled analgesia.Description of Studies Exploring Systemic Defenses to Prevent IV MEs (n = 47)
The systematic search on Medline (Ovid) found 47 articles describing systemic defenses to prevent IV MEs published between June 2016 and October 2021 (Supplementary file 3, https://links.lww.com/JPS/A612). The studies were conducted in the United States (n = 16),47–62 the United Kingdom (n = 7),63–69 Australia (n = 3),70–72 Brazil (n = 3),73–75 Spain (n = 3),76–78 Mexico (n = 2),79,80 Saudi Arabia (n = 2),81,82 Singapore (n = 2),83,84 Canada (n = 1),85 China (n = 1),86 France (n = 1),87 Germany (n = 1),88 Italy (n = 1),89 Netherlands (n = 1),90 and Switzerland (n = 1).91 Some studies (n = 2) were carried out in multiple countries.92,93 The studies were conducted in hospital settings without a specification of a specialty area (n = 10),55,56,61–63,66,73,76,82,90 adult ICU (n = 9),49,50,52,69,75,78–80,92 hospital pharmacy (n = 7),47,51,57–60,93 pediatric intensive care unit (n = 5),65,68,72,74,77 pediatric hospital (n = 3),54,64,71 emergency department (n = 2),70,84 anesthesia department (n = 1),87 cancer hospital (n = 1),86 and pediatric emergency department (n = 1).81 Some studies (n = 8) were carried out in simulated environments comprising an anesthesia setting (n = 2),83,88 hospital setting (n = 2),48,67 ICU (n = 1),85 NICU (n = 1),89 operating room (n = 1),53 and pediatric emergency department (n = 1).91
A lot of variation between the study designs and research methods was identified (Supplementary file 3, https://links.lww.com/JPS/A613). The designs used in more than one study were observational simulation studies (n = 8),48,53,67,83,85,88,89,91 retrospective analysis of drug preparation reports (n = 6),47,51,57,59,60,93 mixed-methods studies (n = 5),63,64,68,69,76 observational studies (n = 5),49,50,56,58,81 retrospective analysis of smart infusion pump alert log data (n = 5),55,62,77,80,82 studies measuring costs or cost effectiveness of the studied defense (n = 4),66,74,87,90 observational intervention studies (n = 3),61,71,73 retrospective or observational studies measuring drug consumption (n = 2),52,79 chart reviews (n = 2),70,72 and studies to design and develop systemic defenses (n = 2).65,92 Other methods included an analysis of administration error reports (n = 1),54 a survey study (n = 1),84 healthcare failure mode and effects analysis (HFMEA) (n = 1),86 a systematic review (n = 1),78 and a systematic review with a meta-analysis (n = 1).75
The evolution of systemic defenses to prevent IV MEs between our previous systematic review20 and the present narrative review (n = 47 articles) is presented in Figure 4. A growing research interest in systemic defenses related to IV preparation (n = 13)47,51,53,57–60,65,68,72,76,89,93 and ready-to-use IV drugs (n = 5)48,56,64,87,90 was identified. Administration remained the most widely studied phase of the MMU process (n = 13).55,62,63,69,74,75,77–80,82–84 Overall, research of systemic defenses to secure IV medication safety has shifted more toward introduction of new technologies, especially in IV preparation and administration.
 FIGURE 4: Evolution of systemic defenses to prevent IV MEs. The defenses identified in the articles (n = 47)47–93 found in the updated literature search on Medline (Ovid) in 2021 are highlighted in red. For comparison, the defenses identified in our original systematic review are displayed in normal text.20 The defenses are classified according to the stages of the MMU process and presented using the “Swiss cheese model” by Reason (2000).12 CDSS, clinical decision support system; CPOE, computerized prescriber order entry; CVC, central venous catheter; DERS, dose error reduction software; SOP, standard operating procedure.The Most Studied Technological Solutions to Secure Safe IV MMU Process
FIGURE 4: Evolution of systemic defenses to prevent IV MEs. The defenses identified in the articles (n = 47)47–93 found in the updated literature search on Medline (Ovid) in 2021 are highlighted in red. For comparison, the defenses identified in our original systematic review are displayed in normal text.20 The defenses are classified according to the stages of the MMU process and presented using the “Swiss cheese model” by Reason (2000).12 CDSS, clinical decision support system; CPOE, computerized prescriber order entry; CVC, central venous catheter; DERS, dose error reduction software; SOP, standard operating procedure.The Most Studied Technological Solutions to Secure Safe IV MMU Process
The most studied medication management technologies in all the included articles (n = 63) were smart infusion pumps (n = 13, 21%)6,31,34,55,62,63,69,74,75,77,79,80,82 (Table 1) and IV preparation workflow systems (n = 8, 13%)32,47,51,57,59,60,89,93 (Table 2). Most of these studies were focused on investigating smart pumps and IV preparation workflow systems as systemic defenses (n = 17),47,51,55,57,59,60,62,63,69,74,75,77,79,80,82,89,93 while only some explored the causes of MEs related to implementation and use of these technologies (n = 4).6,31,32,34 The studies of smart infusion pumps focused on pump compliance,55,77,80,82 cost-effectiveness,74,79 the ability of smart pumps to prevent IV MEs,63,75 and interoperability with electronic health record (EHR) system (Table 1).62,69 IV preparation workflow systems were examined from 2 different perspectives: prospective risk management in system implementation,32 and to describe the benefits of these systems in terms of preventing preparation errors (Table 2).47,51,57,59,93 In addition, 2 studies investigated feasibility and effectiveness of IV robotic system as a systemic defense.60,89
TABLE 1 - A Summary of the Key Findings of Studies Investigating Smart Infusion Pumps (n = 13)6,31,34,55,62,63,69,74,75,77,79,80,82 Reference Study Design Objectives Key Findings Systemic causes of IV MEs related to smart infusion pumps (n = 3 studies) Kirkendall et al, 202034 A systematic review. To identify the types of human based MEs and associated error prevention strategies related to smart pump use. Smart pumps produce new previously unknown classes of MEs associated with their use. Extraction of error types and prevention strategies resulted in the identification of 18 smart pump-specific error types (e.g., drug library errors and programming errors), 21 error subtypes, and 10 prevention strategies (e.g., technological integration of systems and uniform pump brand/function. Marwitz et al, 201931 A retrospective descriptive analysis of the infusion pump alert data. To use the REMEDI dataset, an aggregate, multihospital database inclusive of smart pump analytics, to improve the current understanding of clinical practices for IV HAM administration. Over 70% of smart pump alerts were bypassed by clinicians in 17 hospitals, which is a symptom of alert fatigue. Schnock et al, 20176 A multisite study using the prospective point prevalence approach. To investigate the types and frequency of intravenous medication errors associated with smart pumps in the USA. 60% of the observed infusions in 10 hospitals were associated with one or more MEs. The MEs were predominantly associated with violations of hospital policy (e.g., labeling errors, bypassing the smart pump and the drug library). Smart infusion pumps with DERS as a systemic defense (n = 8) Giuliano et al, 201855 A retrospective one-way analysis of variance and a descriptive overview of smart pump alerts. To improve the overall understanding of IV smart pump drug library compliance by using the REMEDI data set to describe end-user compliance. There are differences in IV smart pump compliance both within and between hospital systems. IV smart pump type and the number of drug library profiles may be influencing factors for smart pump compliance. Ibarra-Perez et al, 202180 A descriptive retrospective analysis of the smart pump alert reports. To investigate the efficacy of IV smart pumps with drug libraries and DERS to intercept programming errors entailing high risk for patients in an adult ICU. Drug library compliance was 70%. MEs were intercepted in 30% of infusions when using a drug library. Upper hard limit alerts accounted for 26% of pump reprogramming events. Jani et al, 202063 A retrospective review of ME reports and observed MEs. To explore the role of smart infusion devices in preventing or contributing to medication administration errors using retrospective review of 2 complementary data sets. Smart pumps both prevent and contribute to MEs. Using any infusion device rather than gravitational administration may have prevented 8–13% of MEs. EHR-integrated pumps could have prevented 52–73% of MEs. Manrique-Rodriguez et al, 201677 A prospective, observational interventional study with analytical components. To estimate the impact of smart pump implementation in a PICU in terms of number and type of administration errors intercepted. Drug library compliance was 84% and 283 MEs were intercepted for a study period of 62 months. A high-risk drug was involved in 58% of prevented MEs, which is why smart pump implementation was proven effective in intercepting programming errors of high-risk drugs. Moreira et al, 202075 A systematic review and meta-analysis. To identify the scientific evidence for the frequency of handling errors of conventional and smart pump infusions in IV insulin therapy in ICUs. An error rate of 10%–40% was associated with conventional pumps and 0–14% with smart pumps. Meta-analysis of 2 studies favored smart pumps to reduce the relative risk of programming errors by 51%. Palacios Rosas et al, 201979 A retrospective observational study with a pre-post design. To evaluate the economic impact of the implementation of smart infusion pumps in the consumption of IV solutions in an ICU. Implementation of smart infusion pumps allows savings by reducing the annual consumption of IV solutions measured in both units (18%) and liters (22.3%). Silva et al, 201974 A mathematical modeling for economic analysis to analyze cost-effectiveness. To analyze cost-effectiveness and to calculate incremental cost-effectiveness ratio of the use of infusion pumps with drug library to reduce errors in IV drug administration in pediatric and neonatal patients in ICUs. Infusion pump with a drug library may be the best strategy to avoid IV administration errors. Although it has the lowest cost, the conventional pump also has lower effectiveness. Waterson et al, 202082 A retrospective review of drug library reports. To establish baseline data to show how metrics in the set-up and programming phase of IV medication administration can be produced from medication library near-miss error reports from infusion pumps. Drug library compliance was 74%. Wrong drug selections (LASA errors) represented 3% of drug library alerts and 22% of canceled infusions. Wrong dose selection was responsible for 3% of alerts and 19% of canceled infusions. Smart infusion pump interoperability with EHR as a systemic defense (n = 2) Furniss et al, 202069 A sociotechnical investigation utilizing in-depth qualitative observations and interviews. To gain an in-depth understanding of the patterns of working that had evolved in an ICU where a closed-loop IV medication administration documentation system had been implemented and of the consequent effects on patient safety. Several benefits were identified (e.g., hard and soft limits for different drugs, bolus limits for certain drugs, automatic recording of drug administration). Challenges included inadequate and outdated drug libraries, pump or medications not mapped with the EHR system, and inconsistency in dosing units between the drug library, EHR and usual pump-programming practices. Wei et al, 202162 Retrospective analysis of infusion pump log data. To describe the patient safety and financial impact of pump-EHR interoperability at a community hospital. Pump-EHR interoperability leads to safer administration of IV medications based on improved drug library compliance (74% versus 83%) and more accurate smart pump programming (infusions generating alerts 4% versus 3%).DERS, dose error reduction software; LASA, look alike sound alike; ME, medication error; PICU, pediatric intensive care unit; REMEDI, Regenstrief National Center for Medical Device Informatics.
FMEA = failure mode and effects analysis, IV = intravenous, IVWMS = intravenous workflow management system, ME = medication error, TAWF = technology-assisted workflow.
Our narrative review demonstrated a recent expansion of, and growing interest in, research related to medication safety of IV drug therapy. When compared to our previous systematic reviews,19,20 the present updated literature search resulted in similar numbers of publications, although the search timeframe was shorter than in the original search, and the current search was conducted only in one database. While our previous review of systemic causes of IV MEs highlighted the need for more research into prescribing, preparation, and administration phases,19 the present narrative review indicated that research interest in drug preparation and administration has remained, but research into causes of prescribing errors is still lacking. In addition, the transition from using retrospective research methods and study designs toward prospective risk management was identified in studies investigating systemic causes of IV MEs, because methods such as FMEA32 and inductive PHA41 were increasingly used in recent studies. This may represent a currently increasing trend of study focus in preventive IV medication risk management and has not been demonstrated in such an extent in previous literature.
In relation to studying systemic defenses to IV MEs, the stages of prescribing, preparation, and administration remained dominant.20 However, the identified widely expanding research interest in systemic defenses to secure safe IV drug preparation represents a key finding. This is central, as manual IV drug preparation has been identified as an especially high-risk task.4,16,17 If an IV workflow management system is not available, it is recommended that a second individual performs an independent verification of manual additions to ensure that the proper medications (and diluents) are added, including confirmation of the proper volume of each medication (and diluent) before its addition to the final container.15 However, without technological assistance, manual double-check procedures have been recognized as complex, laborious, and rarely executed to full extent.94,95 Our present review identified a growing interest in IV preparation workflow software and robotic systems that could secure and, at least to some extent, replace risky manual work steps.47,51,57,59,60,89,93 Implementation of these systems has also been highlighted elsewhere, accompanied by technology utilized in telepharmacy operations.15,27
In addition to streamlining the preparation workflow and equipment, standardizing IV infusions is one of the key components of error prevention both in adult and pediatric populations.10,65,68,72,76,96,97 However, the most powerful safeguard against preparation errors is to dispense IV medications in ready-to-administer packaging without further manipulation by the person administering the medication (e.g., withdrawing doses from containers or reconstituting powdered drug products).27,96,97 This trend was also noticeable in our review, as safety and cost-effectiveness of ready-to-use IV injections and infusions represented a new individual research area.48,56,64,87,90 Overall, our work shows that several alternative systemic defenses to secure safe preparation of IV medications are available, with the aim to either reduce or secure risky manual work steps. When it comes to IV medication guidelines, user-testing seems to be worthwhile to ensure practical and easy-to-understand instructions.38
Smart infusion pumps remained one of the most widely studied technological defense in IV drug therapy.55,63,74,75,77,79,80,82 Examples of new perspectives include studies employing larger datasets collected from multiple hospitals31,55 and smart infusion pump cost-effectiveness.74 In the literature, smart infusion pumps have been associated with alert fatigue resulting in insufficient compliance with drug library use and high override rates of soft limits.10,20,98,99 Other barriers include limitations in pump capabilities, availability of pumps in clinical care areas, unfunctional programming workflow, risks associated with secondary infusions, pump data analysis not utilized in q
留言 (0)