According to the World Health Organization Classification 2019, NENs are classified as highly differentiated neuroendocrine tumors (NET), poorly differentiated NEC, or MiNENs [2]. It has been reported that primary NEN in the bile duct accounts for approximately 0.22–1.8% of primary NEN in the pancreas and gastrointestinal tract, and little is known about how to diagnose or optimally treat MiNEN of the bile duct [3,4,5].
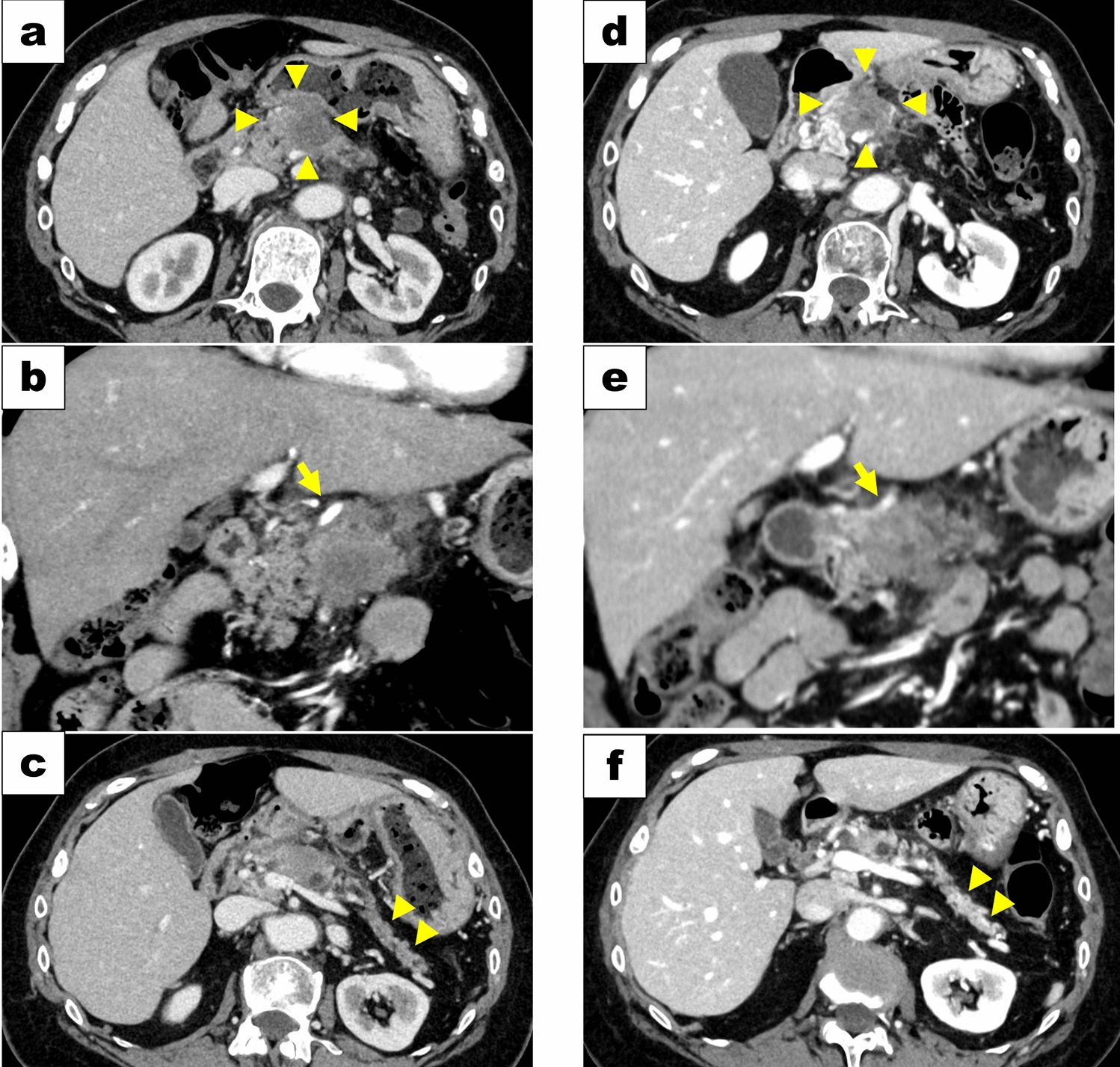
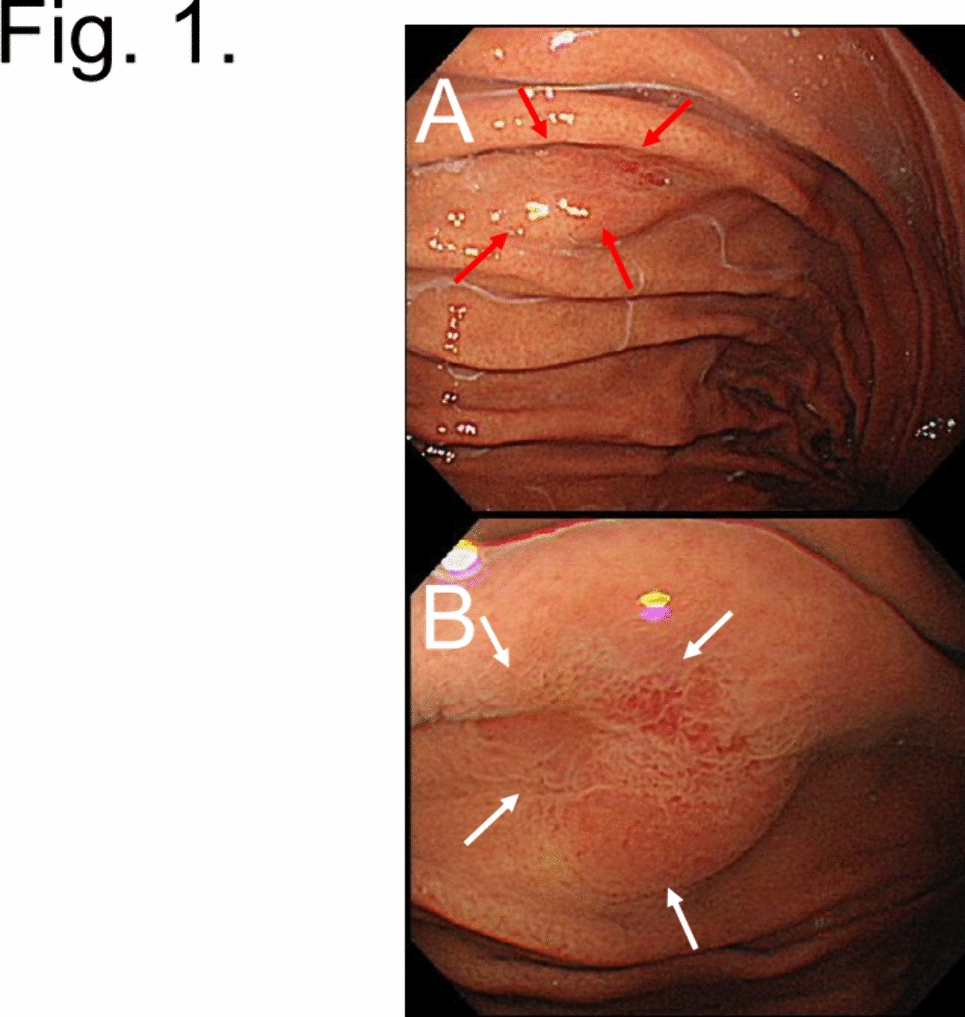
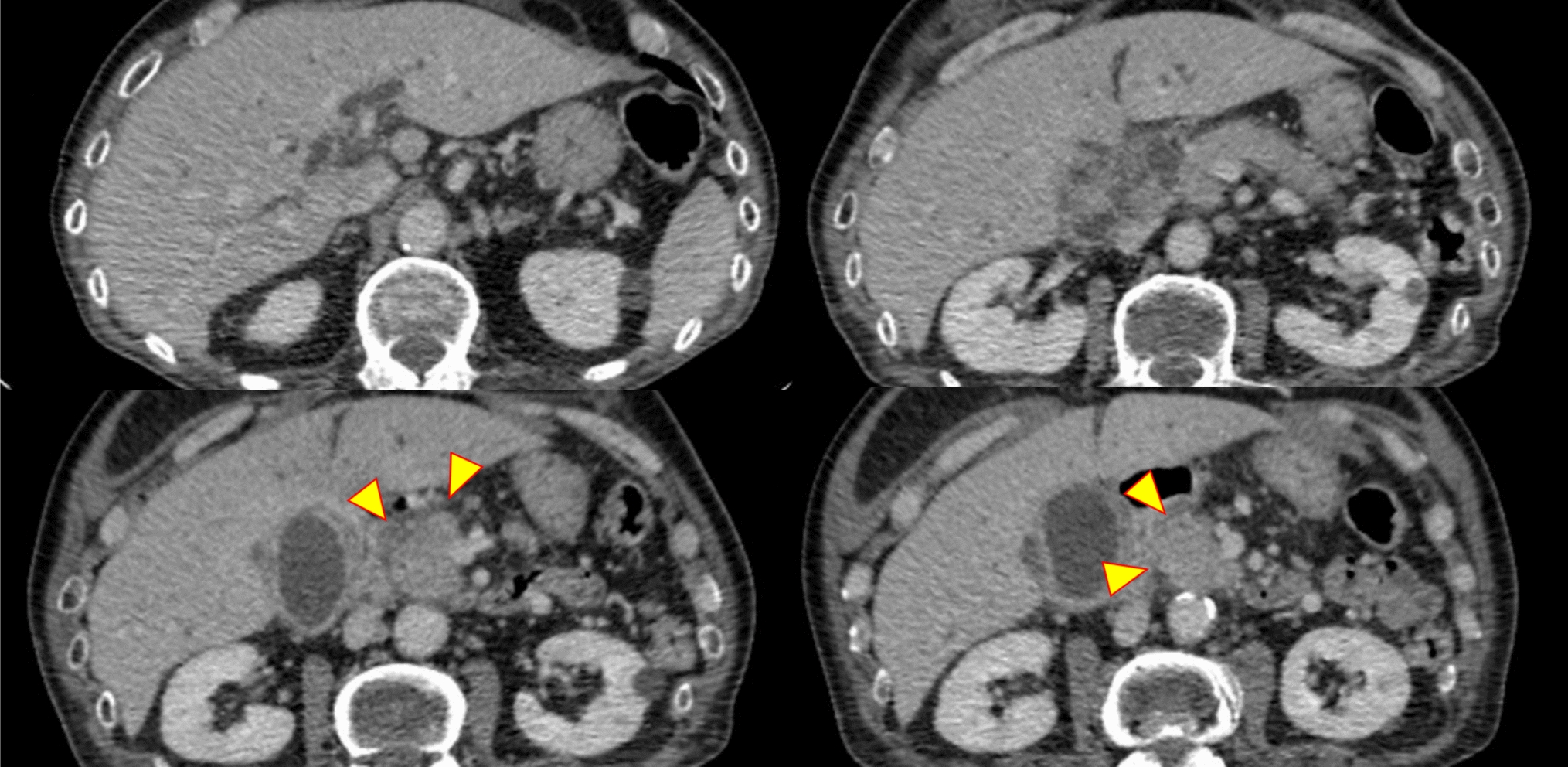
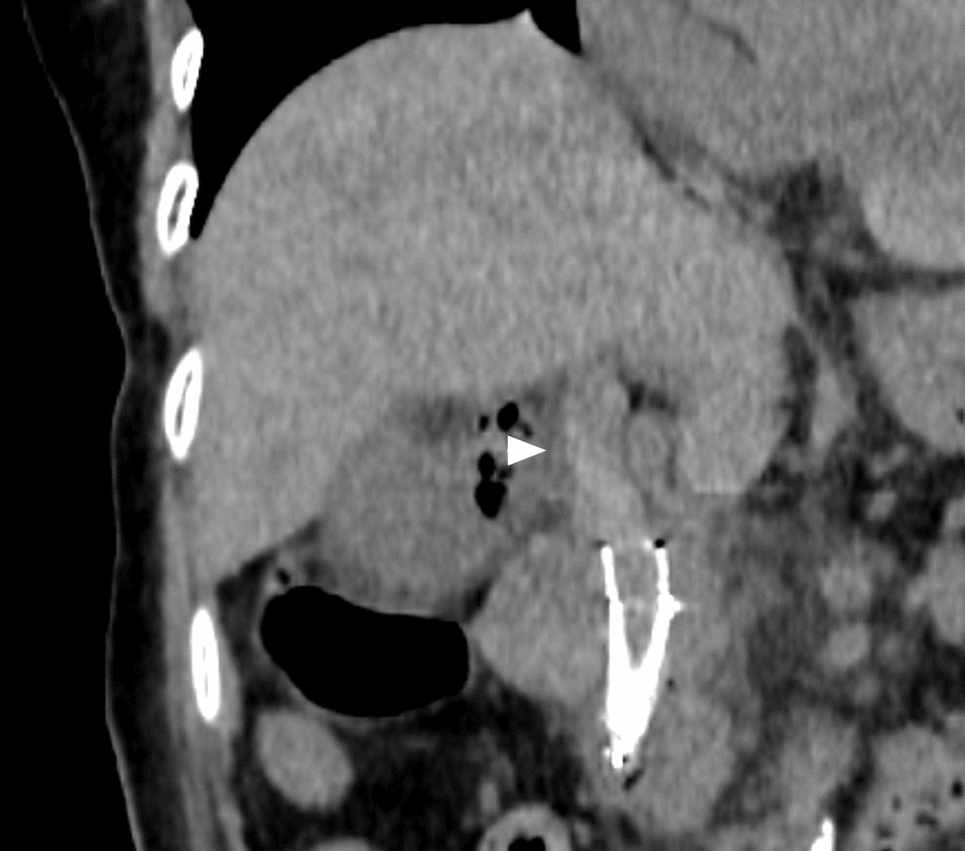
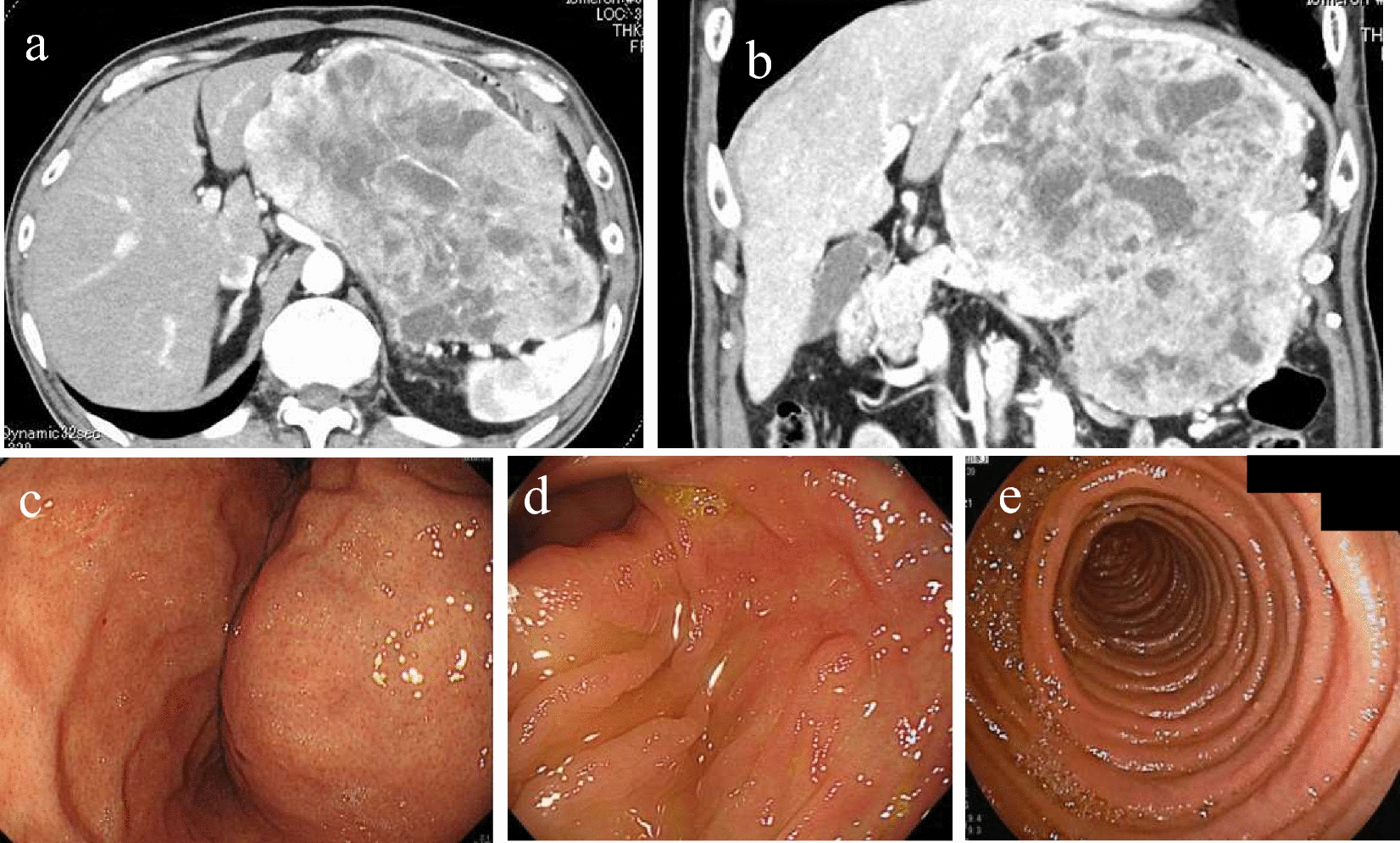
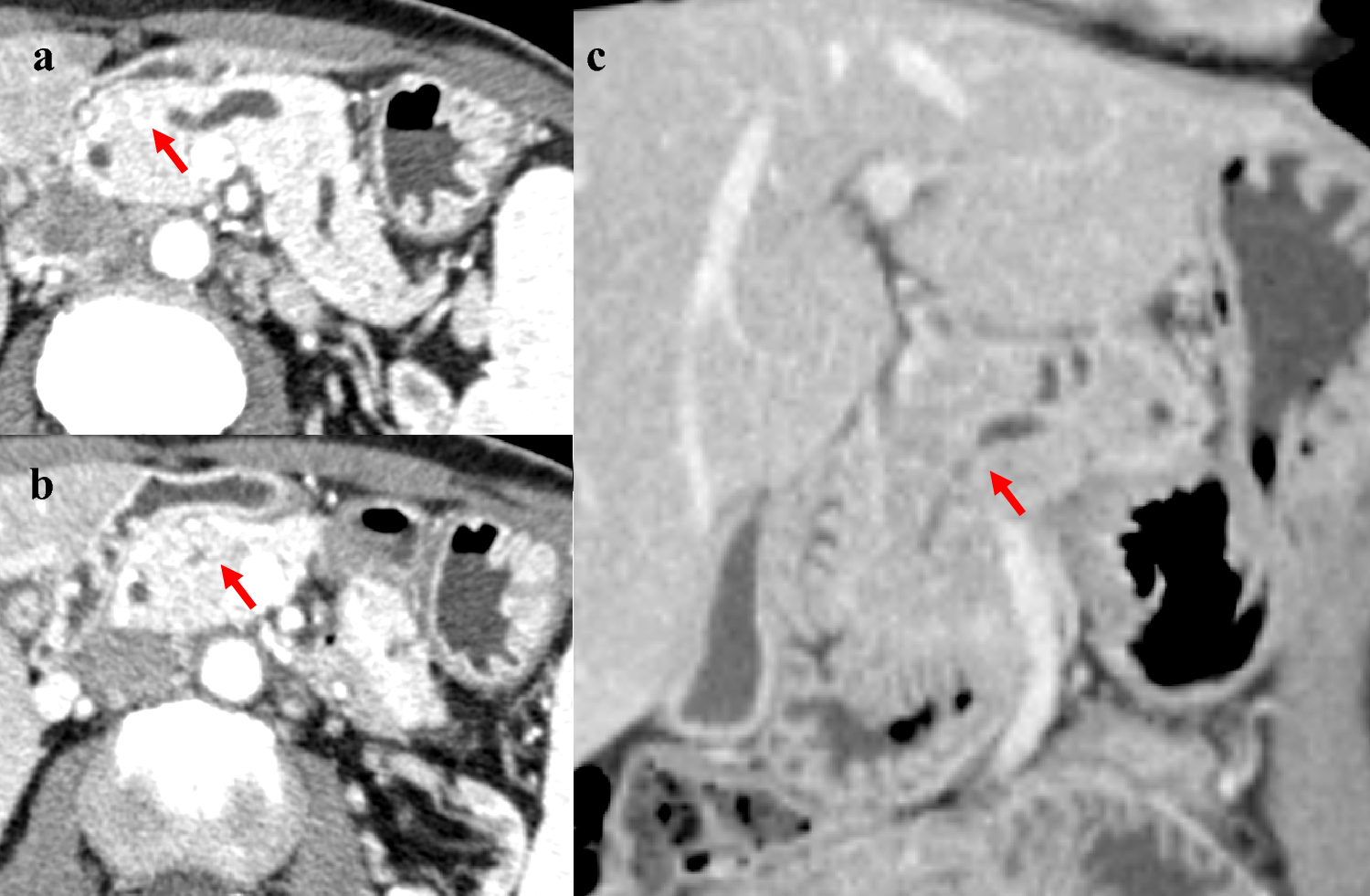
The characteristic imaging findings of biliary MiNENs are unclear because of their rarity and heterogeneity. In our case, the lesion presented as a nodular infiltrating type, and a more abundant blood flow signal was observed in the deeper part of the tumor than on the mucosal side on EUS. Compared with the postoperative pathology specimen, the difference in the blood flow signal may suggest two different tumor components with different regional characteristics. The nodular morphology, invasive nature of the tumor, and submucosal mass may reflect the deep proliferation of the NEC component, which arose from the ADC component. Hong et al. reviewed 11 cases of primary extrahepatic bile duct NEN (1 NET, 7 NEC, and 3 mixed adenocarcinoma neuroendocrine carcinoma [MANEC]) and reported that the tumors presented as nodular or intraductal growing-type lesions [8]. Kaino et al. suggested that MiNEN is an admixture of exocrine and endocrine components and that its contrast pattern may be heterogeneous [9]. Therefore, in tumors with lesions with different blood flow characteristics, close examination for MiNEN may be important; however, it is difficult to differentiate MiNEN from cholangiocarcinoma based on imaging alone.
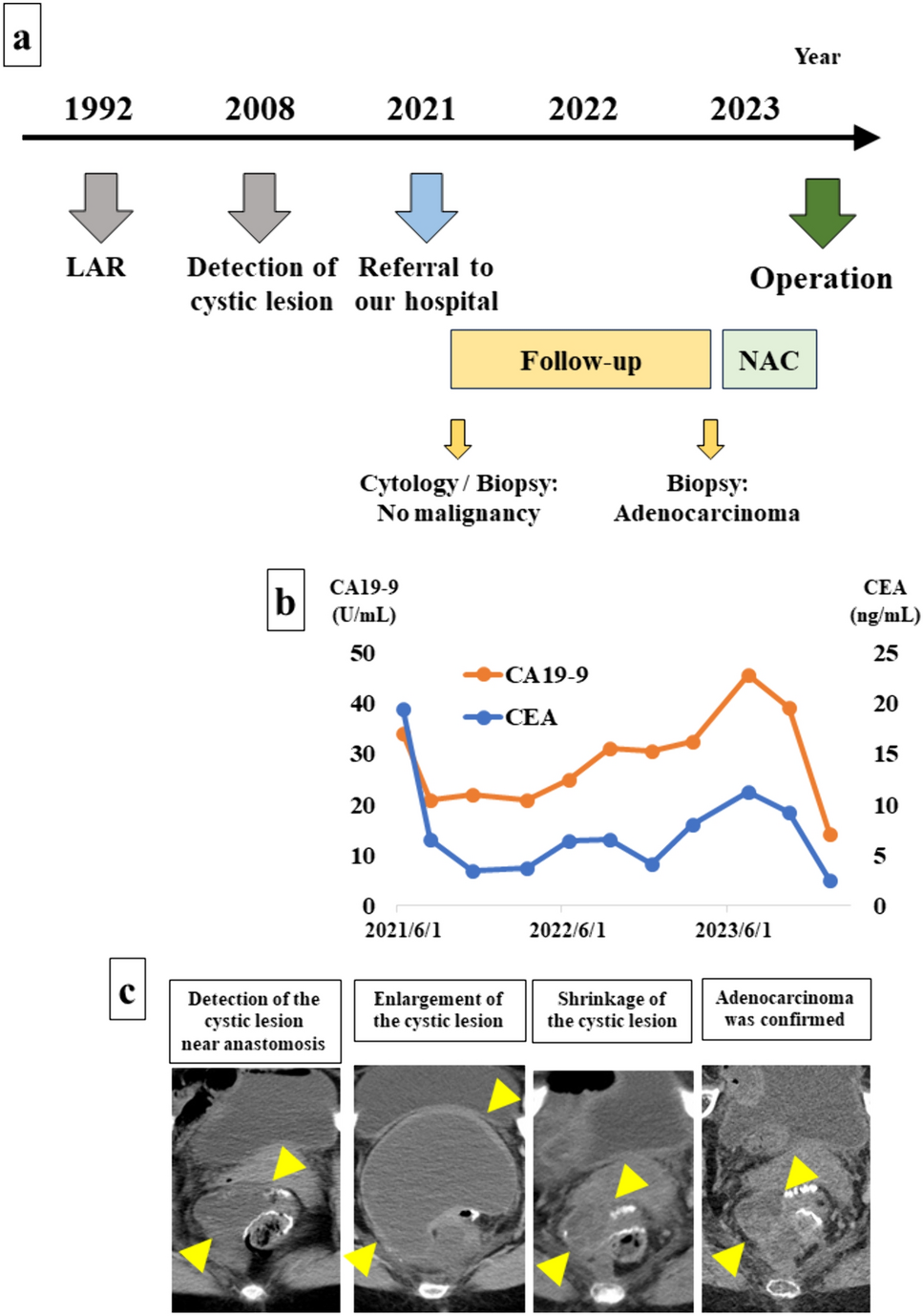
According to a systematic review, the accuracy of the preoperative endoscopic diagnosis was 24.1% in 67 patients who underwent surgical resection for biliary MiNEN [11]. In most cases, the ADC component is located on the mucosal side, and the NEC component is located deeper. It is difficult to detect deeply located NEC components with the commonly performed transpapillary examination, which may be the reason for its low accuracy [10, 11]. Furthermore, the lack of characteristic imaging findings of biliary MiNENs may lead to the diagnosis of cholangiocarcinoma once the ADC component is detected, thus interrupting efforts to detect the NEC component. In MiNEN, NEC is often the cancer component that triggers vascular invasion, liver metastasis, and lymph node metastasis [10, 12], suggesting that histological examination of lymph nodes and liver metastases is likely to detect NEC components. In our case, only the ADC component was detected by transpapillary examination; however, the NEC component was detected by EUS-FNA of the primary tumor and enlarged lymph nodes. For cases in which MiNEN is suspected, it may be necessary to consider not only the transpapillary approach but also the performance of EUS-FNA and the pathological examination of metastases. According to the WHO classification, more than 30% of both components are required to diagnose MiNEN [5, 6], so it is difficult to diagnose MiNEN from biopsy specimens alone. In this case, tumor shrinkage was achieved due to the effects of neoadjuvant chemotherapy, so unfortunately it was not possible to know the exact proportions of both. Therefore, this case cannot be strictly diagnosed as MiNEN. However, there are many similarities between the present case and previous reports. In addition, as a result of comparing the resected specimen and preoperative images, adenocarcinoma was discovered in the same section where the NEC component was present, and it was observed as a single tumor in the image findings before chemotherapy. Therefore, rather than assuming that adenocarcinoma and NEC were present at the same time in the same site, it is reasonable to assume that the tumor contained both components.
Owing to the difficulty of preoperative diagnosis and the rarity of the disease, there is insufficient consensus on treatment for MiNENs with NEC components. In general, treatment for NEC is recommended.
Surgery is the treatment of choice for localized digestive NEC, but relapse is frequent and associated with a poor prognosis. For localized NEC, the presence of regional lymph node metastases and the primary tumor site are considered important prognostic factors [13]. The NCCN guidelines state that treatment options vary depending on the location of the disease, and list neoadjuvant chemotherapy, radiation therapy, chemoradiotherapy, and postoperative adjuvant chemotherapy with or without RT as treatments for resectable NEC [14]. This case was a MiNEN that occurred in the distal bile duct, with lymph node metastasis. The surgical method was pancreaticoduodenectomy, which was highly invasive, and it was suggested that R0 resection might not be possible due to tumor invasion, so we decided to start preoperative chemotherapy. Chemotherapy for NEC recommends combination therapy of cisplatin (CDDP) and ETP, and as an alternative therapy is recommended to use CBDCA instead of CDDP [1, 13]. We chose treatment with CBDCA because the patient was relatively elderly and we wanted to reduce the occurrence of adverse events. There are few reports of neoadjuvant chemotherapy for primary NEC or MiNEN of the bile duct. Terashima et al. reported a case of primary bile duct NEC in which small cell carcinoma was found in biopsy under ERCP and preoperative chemotherapy was performed. CT scan after 2 courses of preoperative chemotherapy (CDDP + ETP) showed no significant change in the size of the tumor, and surgery was performed 2 months after the start of chemotherapy. No postoperative chemotherapy was performed, and CT scan 5 months after surgery showed multiple liver metastases and recurrence [15].
The majority of patients with stage II–III digestive NEC who underwent resection develop recurrence, suggesting that adjuvant chemotherapy may be helpful [13].
A large cohort study of 1861 patients with 519 patients with digestive NEC reported that postoperative chemotherapy was associated with improved survival [16]. Therefore, adjuvant chemotherapy with 4 to 6 cycles of platinum plus ETP may be considered after definitive surgery for local gastrointestinal NEC [13].
Treatment strategies for MiNEN of the bile duct are quite different from those for cholangiocarcinoma. To obtain an accurate preoperative diagnosis, it is important to suspect MiNEN based on atypical tumor images and to make an aggressive histological diagnosis. We believe that patients with MiNEN of the bile duct may benefit from accurate preoperative diagnosis. Neoadjuvant chemotherapy and postoperative adjuvant chemotherapy may be effective treatment options for MiNEN of the bile duct. However, many issues need to be resolved, including the duration of neoadjuvant chemotherapy administration, surveillance intervals, and the timing of planned resection. Therefore, it is desirable to establish a treatment system based on the accumulation and analysis of more cases in the future.




留言 (0)