
記住我



Nurses must meet innumerable daily challenges, which various events of the last four years have compounded. The unprecedented difficulties nurses faced during the COVID-19 pandemic included rapid patient surges, constantly changing work environments, and worsening staff shortages, all of which added to the already stressful nature of nursing work––and chronic stress is a known precursor to burnout. Although the pandemic has waned, nurses' stress levels haven't necessarily abated. According to a 2022 survey by the American Nurses Foundation, nearly half of U.S. nurses reported experiencing burnout; another 36% reported feeling stressed.1 Among health care workers, burnout has been associated with the onset or exacerbation of physical illness, neglect of self-care, fatigue, decreased patient satisfaction, higher medication error rates, lack of nurse engagement, and increased nurse turnover.2-4
Given that workplace stressors can contribute to burnout,5 it's essential that we find effective ways to prevent or mitigate burnout. One such strategy may be physical activity, which is known to have many physical and mental benefits.6
Study aims. This study sought to determine whether a correlation exists between self-reported physical activity levels and nurses' perception of burnout. The secondary aim was to determine whether a correlation exists between the level of perceived burnout and the number of medication errors or near misses.
BACKGROUNDFirst described by researchers in 1974,4 burnout has plagued health care workers for years. Burnout is a psychological condition that manifests in various emotional, psychological, and physical ways; its three defining characteristics are emotional exhaustion, depersonalization, and a low sense of personal accomplishment.2 Burnout can negatively impact nurses both personally and professionally. At the personal level, it can lead to headaches, insomnia, fatigue, and depression,2, 7, 8 as well as neglect of self-care behaviors, including eating well and getting adequate sleep and exercise.9 Such inattention to one's health and self-care can then exacerbate burnout. Professionally, burnout can affect the quality of patient care nurses provide,4, 10 leading to suboptimal care, a higher rate of medication errors, decreased patient satisfaction, decreased nurse engagement, and higher absenteeism and turnover rates.2, 3, 11, 12
Taken together, these factors can cost health care organizations millions of dollars annually.2, 3, 13 Nurse turnover is notably costly. During the COVID-19 pandemic, national nurse turnover rates spiked from a prepandemic average of 17%3 to 22.5%13 in 2022; at our study facility, the nurse turnover rate jumped from a prepandemic average of 13% to 23.2% in 2021. A national survey of 273 hospitals found that, on average, it cost an organization $52,350 to replace one RN.13 Clearly, it is vital that organizations find ways to address nurse burnout and that nurse leaders actively participate in doing so.
Nationwide, chief nursing officers are working to identify areas within their organizations that show high levels of nurse burnout and to implement strategies that can prevent or mitigate burnout and support well-being. Many strategies have been proposed. These often combine measures at the levels of staff nurses, hospital leadership, and the workplace environment. In a meta-analysis exploring the effects on burnout of various coping strategies (including mindfulness-based programs and team support groups), Lee and colleagues found that whichever coping mechanism was used, if used consistently over time, reductions in burnout could last for a year or more.14 But while studies have found mindfulness-based programs to be useful in reducing nurses' stress and burnout,14-16 we found scant research examining the potential impact of physical activity on nurse burnout. Determining whether and to what extent physical activity affects nurse burnout levels could be invaluable in guiding the development of targeted interventions to improve nurses' mental and physical health.
METHODSStudy design and setting. This cross-sectional study was conducted in a 293-bed acute care suburban community hospital, part of an eight-facility health care system in the Southwest region of the United States. The health care system's institutional review board approved the study prior to data collection.
Sample. Convenience sampling was used to obtain the study sample. No power analysis was done; rather, per the team's statistician (one of us, NF), we aimed for a sample size of 19% to 30% of the potential participant pool. Participants were recruited via multiple routes, including email, flyers in nursing unit break rooms, digital learning boards on nursing units, and weekly executive newsletters. All RNs who were employed at the study hospital and had internet access were eligible; employees who were not RNs or who lacked such access were excluded.
To opt in, participants scanned a QR code or clicked on a link that took them to the study survey, which was hosted on the SurveyMonkey platform. Electronic consent was obtained before participants could access the full survey. The survey included demographic items, a 19-question burnout assessment instrument, and a six-question physical activity assessment instrument. A final question asked participants to recall how many medication errors or near misses they had contributed to within the past 12 months.
Data collection. Data were collected for six weeks during the fall of 2022. In addition to standard demographic information such as age and gender, we asked about marital status, whether there were children living at home, years of nursing experience, shift and service area worked, whether the participant had cared for COVID-19 patients between 2020 and 2022, and whether the participant worked a second job. These data were collected because we were interested in the potential personal and work-related factors that might contribute to burnout.
The two assessment instruments were the Copenhagen Burnout Inventory (CBI)17 and the Godin Leisure-Time Exercise Questionnaire (GLTEQ; also known as the Godin-Shephard Leisure-Time Physical Activity Questionnaire).18
The CBI focuses on exhaustion as the core element of burnout, and measures burnout using three subscales: personal burnout, work-related burnout, and client-related burnout.17 The personal burnout subscale measures the degree of physical and psychological exhaustion a person is experiencing, regardless of employment status. The work-related burnout subscale measures the degree of physical and psychological exhaustion the person attributes to work, regardless of the type of work. The client-related burnout subscale, which applies specifically to people working in human services, measures the degree of physical and psychological exhaustion that the person attributes to their work with clients or patients. The CBI has 19 questions, each answerable on a five-item Likert-type scale with responses ranging from 0 (“Never/almost never” or “To a very low degree”) to 4 points (“Always” or “To a very high degree”). These points are rescaled as values from 0 to 100 (0 = 0, 1 = 25, 2 = 50, 3 = 75, 4 = 100). Each subscale score is calculated as the mean of its item scores, and the total score is calculated as the mean of the three subscale scores. The higher the score, the greater the level of burnout, with total CBI scores of 49 or less representing low or no burnout; 50 to 74, moderate burnout; 75 to 99, high burnout; and 100, severe burnout.19 The CBI has shown good internal consistency, with Cronbach α of 0.87 for the personal and work-related burnout subscales and 0.85 for the client-related burnout subscale.17
The GLTEQ asks participants to report how often in a typical week they engaged in mild, moderate, and strenuous exercise for at least 15 minutes.18, 20 The questionnaire defines each category and offers examples. For instance, mild exercise is characterized as requiring “minimal effort” (such as yoga, fishing), moderate exercise as “not exhausting” (such as fast walking, easy bicycling), and strenuous exercise as “heart beats rapidly” (such as running, vigorous bicycling).20 The number of responses in the mild, moderate, and strenuous categories are multiplied by the coefficient 3, 5, or 9, respectively, which represents the metabolic equivalents of that activity level. These values are then totaled to create a leisure score index (LSI). An LSI of 13 or less represents an insufficiently active lifestyle; an LSI of 14 to 23, a moderately active lifestyle; and an LSI of 24 or more, an active lifestyle. Although the GLTEQ's developers did not report Cronbach α, tests of the tool in healthy adults showed acceptable validity and an overall two-week test–retest reliability coefficient of 0.74.21
Data analysis. Statistical analysis was completed using Stata version 17 software. Frequencies and percentages were calculated for all categorical variables. The chi-square (χ2) test was used to assess the association between burnout and physical activity assessment scores, and unpaired t tests were used to assess differences between CBI subscales and participants' service areas. One-way analysis of variance (ANOVA) and post hoc tests were used to analyze relationships between service area and CBI work-related subscale score. The χ2 test was also used to assess the association between burnout and self-reported medication errors and near misses. Statistical significance was set at P ≤ 0.05.
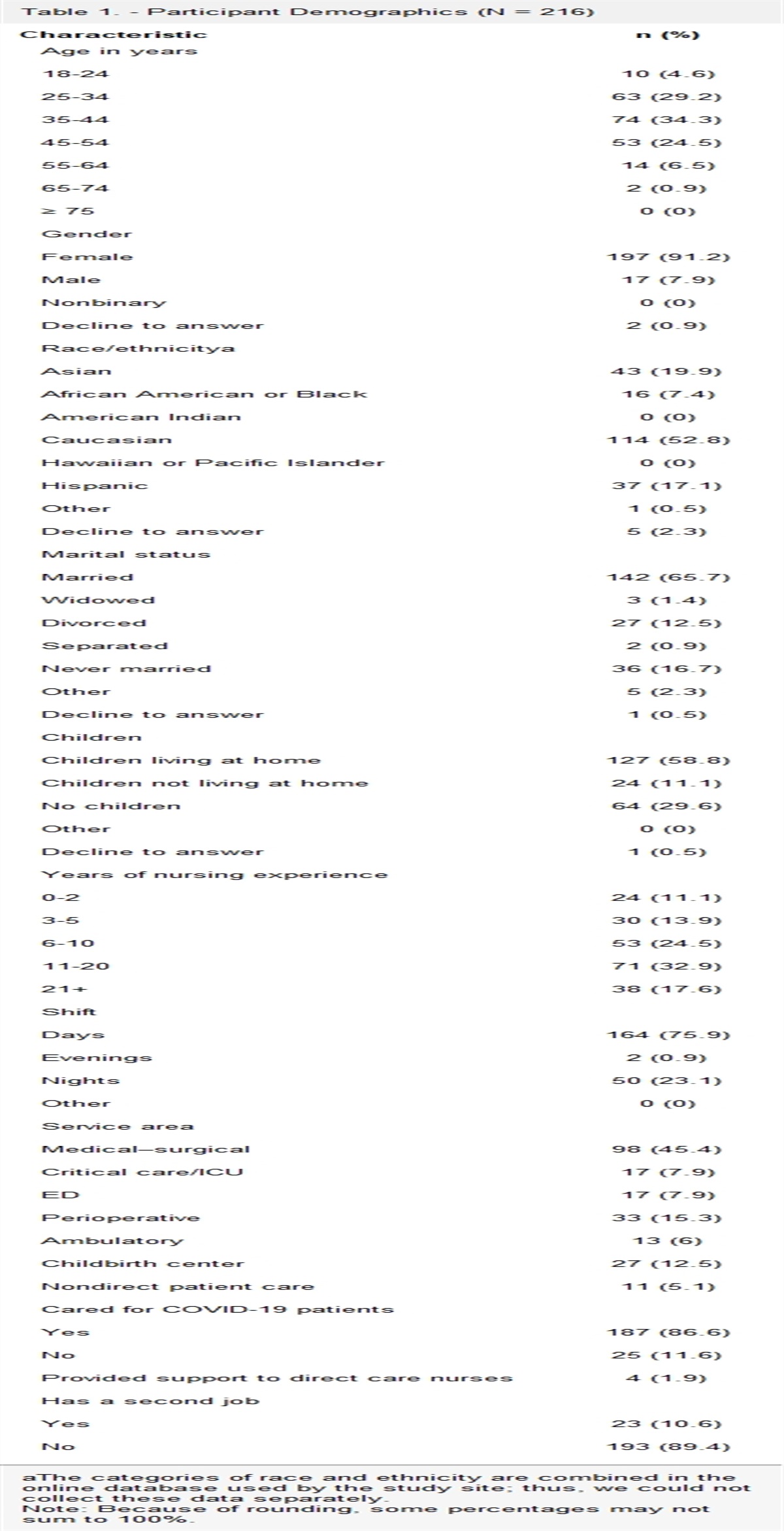
RESULTSSample. A total of 258 out of about 890 people submitted surveys, for a 29% response rate. Of these, 39 surveys were excluded because of incomplete responses and three were excluded because the respondents were not RNs. The final sample comprised 216 participants. Participants were predominantly female (91%) and a majority (63%) were between the ages of 25 and 44 years. About 53% identified as Caucasian, 20% as Asian, 7% as African American or Black, and 17% as Hispanic. Two-thirds (66%) were married and 59% had children living at home. Seventy-six percent worked the day shift, 75% had five or more years of nursing experience, and 45% worked in the medical–surgical environment. For detailed participant characteristics, see Table 1.
Table 1. - Participant Demographics (N = 216) Characteristic n (%) Age in years 18-24 10 (4.6) 25-34 63 (29.2) 35-44 74 (34.3) 45-54 53 (24.5) 55-64 14 (6.5) 65-74 2 (0.9) ≥ 75 0 (0) Gender Female 197 (91.2) Male 17 (7.9) Nonbinary 0 (0) Decline to answer 2 (0.9) Race/ethnicitya Asian 43 (19.9) African American or Black 16 (7.4) American Indian 0 (0) Caucasian 114 (52.8) Hawaiian or Pacific Islander 0 (0) Hispanic 37 (17.1) Other 1 (0.5) Decline to answer 5 (2.3) Marital status Married 142 (65.7) Widowed 3 (1.4) Divorced 27 (12.5) Separated 2 (0.9) Never married 36 (16.7) Other 5 (2.3) Decline to answer 1 (0.5) Children Children living at home 127 (58.8) Children not living at home 24 (11.1) No children 64 (29.6) Other 0 (0) Decline to answer 1 (0.5) Years of nursing experience 0-2 24 (11.1) 3-5 30 (13.9) 6-10 53 (24.5) 11-20 71 (32.9) 21+ 38 (17.6) Shift Days 164 (75.9) Evenings 2 (0.9) Nights 50 (23.1) Other 0 (0) Service area Medical–surgical 98 (45.4) Critical care/ICU 17 (7.9) ED 17 (7.9) Perioperative 33 (15.3) Ambulatory 13 (6) Childbirth center 27 (12.5) Nondirect patient care 11 (5.1) Cared for COVID-19 patients Yes 187 (86.6) No 25 (11.6) Provided support to direct care nurses 4 (1.9) Has a second job Yes 23 (10.6) No 193 (89.4)aThe categories of race and ethnicity are combined in the online database used by the study site; thus, we could not collect these data separately.
Note: Because of rounding, some percentages may not sum to 100%.
CBI and GLTEQ results. All 216 participants completed the CBI; their scores indicated that, overall, 51.4% had low or no burnout, 38.9% had moderate burnout, and 9.7% had high burnout; none had severe burnout. Regarding the CBI subscales, the mean score for personal burnout was 54; for work-related burnout, it was 51; and for client-related burnout, it was 41.
Of the 210 participants completing the GLTEQ, their scores indicated that a majority were either active (57.1%) or moderately active (13.8%), while 29% were insufficiently active. For a summary of CBI and GLTEQ results, see Table 2.
Table 2. - Participants' Results: Copenhagen Burnout Inventory and Godin Leisure-Time Exercise Questionnaire CBI Score Groups (N = 216) Results Overall burnout, mean 49 Overall burnout levels, n (%) Low or no burnout 111 (51.4) Moderate burnout 84 (38.9) High burnout 21 (9.7) Severe burnout 0 (0) Personal burnout subscale, mean 54 Personal burnout levels, n (%) Low or no burnout 92 (42.6) Moderate burnout 87 (40.3) High burnout 34 (15.7) Severe burnout 3 (1.4) Work-related burnout subscale, mean 51 Work-related burnout levels, n (%) Low or no burnout 93 (43.1) Moderate burnout 100 (46.3) High burnout 22 (10.2) Severe burnout 1 (0.5) Client-related burnout subscale, mean 41 Client-related burnout levels, n (%) Low or no burnout 137 (63.4) Moderate burnout 60 (27.8) High burnout 17 (7.9) Severe burnout 2 (0.9) GLTEQ Score Groups (n = 210) Results Insufficiently active, n (%) 61 (29) Moderately active, n (%) 29 (13.8) Active, n (%) 120 (57.1)CBI = Copenhagen Burnout Inventory; GLTEQ = Godin Leisure-Time Exercise Questionnaire.
Note: Because of rounding, some percentages may not sum to 100%.
To explore possible relationships between burnout and physical activity levels, data were analyzed for the 210 participants who completed both the CBI and the GLTEQ. This analysis showed that there was a significant overall association between the CBI score groups and the GLTEQ score groups (P = 0.019). Specifically, the most physically active participants tended to have significantly lower burnout levels, with 68.5% of nurses with low burnout CBI scores also having an LSI of 24 or more. The insufficiently active participants tended to have significantly higher burnout levels, with 47.6% of those with high burnout CBI scores also having an LSI of 13 or less. See Table 3.
Table 3. - Correlations Between Burnout and Physical Activity Levels (n = 210) CBI Score Groups, n (%) GLTEQ Scores (LSI) Total Burnout Low or No Burnout (n = 108) Moderate Burnout (n = 81) High Burnout (n = 21) P Valuea 0.019 ≤ 13: Insufficiently active 61 (29) 24 (22.2) 27 (33.3) 10 (47.6) 14-23: Moderately active 29 (13.8) 10 (9.3) 15 (18.5) 4 (19) ≥ 24: Active 120 (57.1) 74 (68.5) 39 (48.1) 7 (33.3)CBI = Copenhagen Burnout Inventory; GLTEQ = Godin Leisure-Time Exercise Questionnaire; LSI = leisure score index.
aP reflects significance of an overall association between GLTEQ score groups and CBI score groups. The most active nurses were more likely to report low burnout (68.5%), while the least active nurses were more likely to report high burnout (47.6%).
Note: Because of rounding, some percentages may not sum to 100%.
Regarding participants' work characteristics, the nurses who reported caring for COVID-19 patients had significantly higher CBI scores than the nurses who did not (P = 0.034). Ninety percent of the nurses with high burnout had directly cared for COVID-19 patients at some point between 2020 and 2022. Moreover, nurses who cared for COVID-19 patients had significantly higher CBI subscale scores for client-related burnout than nurses who hadn't cared for such patients (P < 0.001).
Compared with nurses working in other service areas, the medical–surgical nurses experienced the highest levels of burnout (P < 0.001). The medical–surgical nurses also had significantly higher CBI work-related subscale scores than nurses in other service areas (P < 0.001). One-way ANOVA testing further revealed a statistically significant difference between nurses working on medical–surgical units and those working on other high acuity units (ICU, ED) regarding level of work-related burnout (F = 9.36, P < 0.001). Post hoc testing showed a statistically significant difference in mean CBI work-related subscale scores for the medical–surgical nurses compared with the outpatient or procedural unit nurses (P < 0.001; 95% CI, 5.63 to 19.57). There were no significant differences for other CBI subscales. For more detailed subscale findings, see Table 4.
Table 4. - Comparison of CBI Work-Related Subscale Scores by Participants' Service Area One-Way ANOVA Results Sum of Squares df Mean Squared F P Value Between groups: medical–surgical vs. high-acuity 7420.29 2 3710.14 9.36 < 0.001 Within groups: medical–surgical and high-acuity 84442.71 213 396.45 Total 91863 216 427.27 Post Hoc Test Results Service Area Pairs Difference Between Pairs SE Q Value 95% CI Critical Mean P Value Medical–surgical and high acuitya 8.52 2.83 3.01 −0.93 to 17.96 9.45 0.09 Medical–surgical and outpatient/proceduralb 12.6 2.09 6.03 5.63 to 19.57 6.97 < 0.001 High acuitya and outpatient/proceduralb 4.08 2.89 1.41 −5.57 to 13.74 9.66 0.58ANOVA = analysis of variance; CBI = Copenhagen Burnout Inventory; df = degrees of freedom; SE = standard error.
aHigh acuity is the ICU and ED.
bOutpatient/procedural is perioperative, ambulatory, childbirth center, and nondirect patient care.
Participants self-reported 102 medication errors or near misses, for an average of 0.5 errors per participant. Seventeen participants who never administered medications were not included in this analysis. There was no statistical relationship between self-reported medication errors or near misses and CBI scores.
DISCUSSIONOur results indicate that there is a negative correlation between levels of burnout and physical activity. In this study, the nurses who reported being most physically active also tended to report low levels of burnout, while those who reported being most sedentary tended to report high levels of burnout. Although these findings do not prove a causal relationship between physical activity and burnout scores, they do show a relationship between the two. While we recognize how busy nurses are in their day-to-day activities, we propose that raising nurses' physical activity levels may be essential to solving the problem of burnout. The next phase of research at the study hospital will be an interventional study assessing nurses' burnout levels before and after participating in physical activities. In consideration of the constraints of nurses' schedules and workloads, the intervention will offer a wide array of onsite, offsite, individual, and group options, ranging from mindfulness practices to high-intensity interval training classes.
Given that burnout can lead to neglect of self-care––and that a lack of self-care can contribute to burnout9––it is unsurprising that the participants experiencing higher levels of burnout tended to report being insufficiently active (sedentary). An exploratory study by Das and Adams found that physical activity improved nurses' mental and physical health and mitigated the effects of stress.22 Considering how costly nurse burnout can be, contributing to suboptimal patient care and higher rates of absenteeism and turnover,2, 3, 11, 12 it's important that nurse leaders better understand how physical activity can prevent or ameliorate burnout. Once they do, nurse leaders must begin to educate, encourage, and support their nursing staff in this regard—for example, including a dietician or wellness coach in staff meetings or incorporating a physical activity (such as running a 5K) into team-building practices.
During the COVID-19 pandemic, burnout among nurses rose sharply; indeed, during the first wave, one study found that 90% of nurses at one Italian hospital “met the criteria for medium/high burnout.”23 Our study found that 90% of the nurses with high burnout reported having cared for COVID-19 patients. The pandemic moderately affected the study site, a 293-bed acute care hospital. In 2020, two of its six medical–surgical units were converted to COVID-19 units, and approximately 50% of the ICU beds were occupied by COVID-19 patients. In subsequent surges in 2021 and early 2022, the hospital added a temporary 12-bed unit to accommodate non–COVID-19 patients displaced from the medical–surgical units. In addition to these changes, nurses found themselves caring for sicker, more unstable patients in unprecedented situations; they saw numerous patients deteriorate, go into cardiac or respiratory arrest, and often die. More nurses floated to temporary units, taking them out of their customary environment and away from their usual colleagues. These are among the factors that can contribute to higher rates of stress and burnout.1
An unexpected finding of this study was that medical–surgical nurses had the highest rates of burnout overall as well as work-related burnout. This result runs counter to the commonly held belief that critical care nurses are most susceptible to burnout. Staffing changes (and the resulting heavier workloads) on the medical–surgical units may have been a factor, as inadequate staffing has been associated with nurse burnout.24, 25 Before the pandemic, typical staffing ratios on the medical–surgical units were four patients per nurse on the day shift and five patients per nurse on the night shift. As the pandemic progressed, increasing rates of nurse turnover and COVID-19–related absenteeism resulted in significant understaffing, such that each nurse now cared for five or six patients on both shifts. As the pandemic eased, nursing leadership was able to focus on improving nurse turnover and staffing ratios. Our turnover rate has dropped from 23.2% in 2021 to 11% in 2023, and no contract labor has been hired since December 2022. Other contributing factors specific to medical–surgical nurse burnout will be explored in future research at the study site.
Another important finding was that nurses who cared for COVID-19 patients scored significantly higher across all three subscales of the CBI. Although we didn't measure COVID-19's effect on burnout, this finding is in keeping with evidence of the pandemic's lasting impact on stress and burnout levels in the nursing workforce.1, 5, 23 Leaders must recognize that even though the pandemic has abated, nurses' experiences during the past four years may still be affecting them. Long-term solutions to burnout are needed.
Regarding this study's secondary aim, we found no direct correlation between burnout levels and self-reported medication errors or near misses. That said, as Wakefield and colleagues noted, reporting such errors requires four steps: error recognition, assessment of the need to report the error, incident report preparation, and follow-up response from the report recipient.26 Prior research has established that only 10% to 20% of medication errors are reported.27 It stands to reason that a lack of time and energy on the part of nurses and other providers would affect reporting. Further research exploring the relationship between nurse burnout and self-reported medication errors is recommended.
An analysis of participants' demographic data showed that the nurses who worked in medical–surgical environments, those who had cared for COVID-19 patients between 2020 and 2022, and those who worked the day shift were most likely to experience higher burnout levels. Several factors at the study hospital may have contributed to these results. For instance, during the pandemic, many medical–surgical nurses had to care for higher acuity patients than they were used to, as well as more patients who had cardiac and respiratory arrests. Further studies are needed to better understand the long-term impact of the pandemic on medical–surgical nurses and nurses working with COVID-19 patients.
Limitations. This study had several limitations. First, it was limited to one community hospital in a single state. Its work conditions, employee demographics, and nursing practices may not be representative, limiting the generalizability of the findings. This includes our finding that medical–surgical nurses had the highest burnout levels of all the service areas; it's possible that, at other facilities, nurses in other specialty areas would report differently. Second, both participants' physical activity levels and involvement in medication errors were self-reported. Self-report is subject to recall and reliability errors. Lastly, although we found a negative correlation between burnout and physical activity levels, other factors must be considered before definitive conclusions can be drawn. For example, some factors that in themselves might increase burnout (such as working long hours) may also prevent getting adequate exercise.
CONCLUSIONSThis study found that nurses continued to experience burnout even as the pandemic waned, and that the nurses who reported high levels of physical activity tended to report the lowest levels of burnout. Among all service areas in the study facility, the medical–surgical nurses reported the highest levels of burnout. Having cared for COVID-19 patients at some point between 2020 and 2022 was also associated with high burnout levels, a notable finding given that the disease remains endemic. No relationship was found between burnout and medication errors.
The study findings can help guide the development of interventions that will prevent or mitigate nurse burnout and improve their mental and physical health, thereby potentially reducing turnover and easing the staffing crisis. Further research to determine whether increased physical activity directly reduces burnout is warranted. Targeted programs to reduce work-related burnout, in particular, as well as organizational sponsorship of and unit-level support for such programs, are urgently needed. Our findings suggest that promotion of physical activity may be an essential component to alleviating burnout.
REFERENCES 1. American Nurses Foundation. Three-year annual assessment survey: nurses need increased support from their employer. Silver Spring, MD; 2023 Jan 24. Pulse on the nation's nurses survey; https://www.nursingworld.org/~48fb88/contentassets/23d4f79cea6b4f67ae24714de11783e9/anf-impact-assessment-third-year_v5.pdf. 2. Mudallal RH, et al. Nurses' burnout: the influence of leader empowering behaviors, work conditions, and demographic traits. Inquiry 2017;54:46958017724944. 3. Muir KJ, et al. Evaluating the costs of nurse burnout-attributed turnover. J Patient Saf 2022;18(4):351–7. 4. Reith TP. Burnout in United States healthcare professionals: a narrative review. Cureus 2018;10(12):e3681. 5. Norful AA, et al. Primary drivers and psychological manifestations of stress in frontline healthcare workforce during the initial COVID-19 outbreak in the United States. Gen Hosp Psychiatry 2021;69:20–6. 6. Kebaili L, et al. The effect of physical activity on the mental health of the individual. HIV Nursing 2023;23(3):243–46. 7. Patrick K, Lavery JF. Burnout in nursing. Aust J Adv Nurs 2007;24(3):43–8. 8. Spence Laschinger HK, et al. Workplace empowerment as a predictor of nurse burnout in restructured health care settings. Healthc Q 2003;6(4). 9. Couser G, et al. Develping a course to promote self-care for nurses to address burnout. Online J Issues Nurs 2020;25(3). 10. Theofanidis D, et al. A ‘new pandemic’ at hand: burnout of nursing staff. Int J Caring Sci 2022;15(1):228–35. 11. Gupta SJ, et al. Interest in online interprofessional elective mind-body skills (MBS) training. Complement Ther Med 2018;36:137–41. 12. Vahey DC, et al. Nurse burnout and patient satisfaction. Med Care 2004;42(2 Suppl):II57–II66. 13. NSI Nursing Solutions. 2023 NSI national health care retention and RN staffing report. East Petersburg, PA; 2023. https://www.nsinursingsolutions.com/Documents/Library/NSI_National_Health_Care_Retention_Report.pdf. 14. Lee HF, et al. A meta-analysis of the effects of coping strategies on reducing nurse burnout. Appl Nurs Res 2016;31:100–10. 15. Foureur M, et al. Enhancing the resilience of nurses and midwives: pilot of a mindfulness-based program for increased health, sense of coherence and decreased depression, anxiety and stress. Contemp Nurse 2013;45(1):114–25. 16. Ghawadra SF, et al. Mindfulness-based stress reduction for psychological distress among nurses: a systematic review. J Clin Nurs 2019;28(21-22):3747–58. 17. Borritz M, et al. Burnout among employees in human service work: design and baseline findings of the PUMA study. Scand J Public Health 2006;34(1):49–58. 18. Amireault S, Godin G. The Godin-Shephard leisure-time physical activity questionnaire: validity evidence supporting its use for classifying healthy adults into active and insufficiently active categories. Percept Mot Skills 2015;120(2):604–22. 19. Bolatov AK, et al. Psychometric properties of the Copenhagen burnout inventory in a sample of medical students in Kazakhstan. Psychol Russ 2021;14(2):15–24. 20. Godin G. The Godin-Shephard leisure-time physical activity questionnaire. Health and Fitness Journal of Canada 2011;4(1):18–22. 21. Godin G, Shephard RJ. A simple method to assess exercise behavior in the community. Can J Appl Sport Sci 1985;10(3):141–6. 22. Das BM, Adams BC. Nurses' physical activity exploratory study: caring for
留言 (0)