
記住我




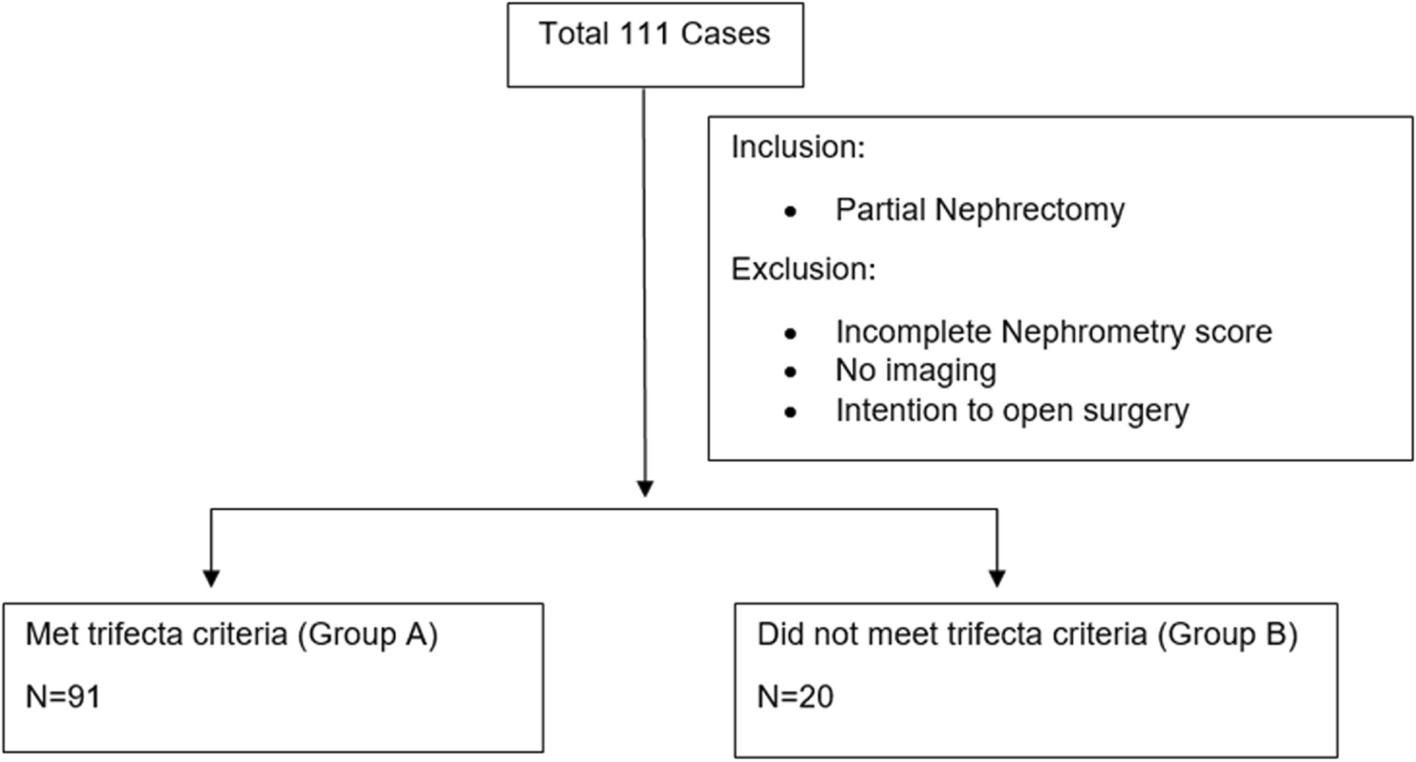

Using the above search criteria, a total of 704 documents were considered. After filtering out duplicates 254 documents remained and After screening by title, abstract and full text, 246 literatures were excluded for various reasons. Finally, A total of 8 papers were included in this review (Fig. 1).
Fig. 1
Among the included studies, seven were of medium to high quality, and two were of low quality. The specific scoring details are shown in Table 1. This study used the the Newcastle-Ottawa scale for the quality assessment.
Table 1 The score chart of NOSCharacteristics observed in the clinical settingMorbidity and mortalityA retrospective analysis was performed by Floriane et al. on French data from 2010 to 2018 [10]. To assess the incidence of bladder cancer (BC) in patients with multiple sclerosis (MS), spinal cord injury (SCI), and spina bifida (SB). This study included a total of 50,243,847 individuals, among whom 2015 patients (0.004%) were identified as having BC in conjunction with neurogenic bladder. With average age of onset 65.4 ± 12.3 years and affecting more men than women. And also showed that SCI patients had a higher incidence of BC than MS and SB, with a rate of 791.1/100 000 persons/year.
Similar findings were obtained by Böthig et al. [11]. who conducted a retrospective analysis of 7004 individuals suffering from SCI between 1998 and 2018. Four patients (incidence approximately 0.0571%) were diagnosed with BC after several years, with an average age of onset of 65.5 years (median age of 64 years [52–82]). In addition, Bothig et al. [12] found that the age at diagnosis of bladder cancer was 56.6, and the age of initial diagnosis is younger, at 19 years old. The average time spent in patients with urinary catheters from spinal cord injury to bladder cancer was significantly longer than that spent in patients with no-urinary catheters. Noteworthy, the age of onset and incidence rates were similar in both studies, and this finding is consistent with previous studies (Table 2).
Table 2 The occurrence of BC among individuals who have experienced a SCIHowever, other authors have derived incidence rates that are about ten times higher than the above two. Gui-Zhong et al. used the MEDLINE, EMBASE, CINAHL and the Cochrane Register database to search the literature found that out of 99,237 individuals with SCI, 596 were diagnosed with BC [4]. (An occurrence rate of 0.601%), with an average age of onset around 50 years. While, The incidence of bladder SCC was higher than that in the general population. To find the effect of chronic indwelling catheterization on the occurrence of bladder cancer, a study compared the effect of chronic indwelling urinary catheters(CIDC) between a non-SCI group and an SCI-group (control group) of patients. The incidence of bladder cancer in the SCI group and the CIDC-non-SCI group was 68.90 and 102.53 per 100,000 person-years and both were higher than the control group (12 per 100,000 person-years). This study was conducted in Taiwan on 1,816 individuals with SCI. Among who, 10 were diagnosed with BC, (incidence rate of 0.551%) with average age of onset of BC 47.42 ± 15.84 years [13]. Ammirati Enrico [14] evaluated 11 patients with SCI from 2011 to 2020 and all patients were treated with CIC. At late follow-up, one patient had found high-grade non-invasive bladder cancer after radical cystectomy. In this study, the investigators only randomly selected 11 SCI patients and did not include all SCI patients, so the results were not universal. However, the results show that long-term urinary catheterization treatment may increase the risk of bladder cancer. Hidalgo Romero A used a similar approach [15]. The authors selected 10 patients who developed bladder cancer after SCI / NTD from 2007 to 2023. By collecting various clinical and pathological information of patients, it was found that all patients had high-grade non-urothelial cell carcinoma. Three cases developed lymph node metastases. This follows that bladder cancer caused by SCI may have a worse prognosis.
The incidence of bladder cancer found in the above studies is not exactly the same. And The differences may be related to the diseased race, living environment and habits. Despite the differing conclusions among experts, all studies show that individuals with SCI can potentially experience BC at a younger age than the general population(Table 2).
A study conducted between 1960 and 2009 by Laura et al. involving 45,486 patients with SCI and a total follow-up of 566,532 person-years, revealed that out of the 10,575 patients who passed away, 99 deaths were attributed to BC [16]. The standardized mortality ratio (SMR) for BC was significantly higher (6.7) in SCI patients compared to the general population, indicating a substantial difference. Likewise, Böthig et al. yielded comparable outcomes. In a study conducted in Germany between 1998 and 2014 involving 6995 patients with SCI [17]. Among the cohort of 24 individuals diagnosed with spinal cord injury (SCI) and bladder cancer, a total of 12 individuals succumbed to the disease (50%). The median survival time for this group was found to be 11.5 months, while the mean survival time was calculated to be 22.71 months, with a standard deviation of 30.42 months (Table 3). Both studies discovered that individuals with SCI succumbed to BC at a younger age than the overall population. Additionally, they observed a correlation between SCI patients and a lower pathological staging, indicating that SCI patients tend to develop BC with a less favorable prognosis. These findings are consistent with the prevailing body of published literature on the subject matter.
Table 3 The death rate of BC among individuals who have experienced SCIMechanism of occurrenceBC is primarily caused by smoking and prolonged exposure to chemicals such as aromatic amines [18]. While, diet may also increase the occurrence of bladder cancer, as Aveta et al. found that “red meat” and “processed meat” may be positively associated with bladder cancer risk [19]. In individuals with neurogenic bladder resulting from SCI, healthcare facilities often use catheters or suprapubic cystostomies for extended durations, which, along with the factors mentioned above, have been linked to chronic bladder inflammation and an increased risk of BC [20, 21]. Furthermore, the prolonged use of catheters can lead to intricate urinary tract infections and the formation of bladder stones, increasing the probability of developing BC (Fig. 2) [22]. Studies have found that lower bladder compliance and higher maximum bladder pressure are observed in SCI mice. Overactive bladder(OAB) increases, and an indwelling catheter is needed to relieve the patient’s disease [23]. For OAB, studies have found that capsaicin-sensitive bladder afferent neurons (B-AN) and type A voltage-gated potassium channel (KA) function were decreased in SCI mice compared with the control group [24]. Indicating that reduced KA channel activity is associated with hyperexcitability of capsaicin-sensitive C fiber B-AN after SCI. Therefore, studies targeting neuronal-type KA ion channels are expected to be a new therapeutic target for OAB. This method may be used to reduce the possibility of long-term indwelling urinary catheters. Von Siebenthal et al. [25] compared bladder function in the SCI (neurogenic) and bladder outlet obstruction (obstructive) mice by repeated urodynamic examination. This study found that the SCI group had dysfunctional bladder detrusor and sphincter and significantly increased bladder pressure 1 week after injury, and the bladder gradually developed fibrosis throughout the process. These factors are closely related to SCC and muscle infiltration into the bladder in cases of BC. However, what is the link between the two conditions at a microscopic level? Temporal and spatial mutations were discovered in the telomerase reverse transcriptase (TERT) promoter of BC tissue from the general population and in keratinized/non-keratinized squamous epithelial tissue from patients with neurogenic bladder, as found by Taylor et al. [26]. Understanding why chronic cystitis caused by indwelling catheters is related to a higher susceptibility to BC can be facilitated by considering the proposal that this mutation could serve as a plausible pathway for the progression of benign lesions to BC.
Nevertheless, a Meta-analysis revealed that approximately 1% of individuals with SCI who underwent prolonged catheterization experienced the development of BC [27]. Whilst, more than 50% of SCI patients without indwelling catheters experienced the development of BC. Meanwhile, Kalisvaart et al. found that 50% of the individuals included in their research who had BC were not using a catheter for an extended period. BC in patients with SCI can be attributed to various factors [28]. In line with the above data, it is reasonable to infer that indwelling catheters, persistent bladder inflammation, and urinary tract infections are the primary culprits, however, it is important to maintain a skeptical mindset and further investigate the diverse pathways of BC development in SCI patients.
Screening and diagnosisThe topic of contention among medical professionals revolves around the frequency of bladder cancer screening, the appropriate screening methods, and the efficacy of early screening in detecting bladder cancer in SCI patients [29]. According to Laura et al. [16], the average duration between SCI and the identification of BC in patients ranged from 16 to 34 years. A study conducted in Taiwan, in a group of 54,401 individuals with SCI monitored for an average of six years, results did not exhibit a greater likelihood of being diagnosed with BC compared to those without SCI [30]. Consequently, it is advisable to enhance the frequency of patient evaluations for individuals with SCI beyond a decade of SCI to attain prompt identification and medical intervention. and some researhers suggest conducting annual cystoscopy and urine cytology [29].
Urine cytology is not recommended for routine urinalysis in this group of patients due to the possibility of haematuria and pyuria caused by an indwelling catheter. Davies et al. have shown that urine cytology or urine biomarkers do not possess sufficient reliability as a screening technique for individuals with spinal cord injury. A study conducted between 1999 and 2004 examined 457 patients with SCI to evaluate the efficacy of urine biomarkers, specifically the BTA stat test, survivin assay, and cytology, in detecting bladder cancer cases. The findings of this study indicated that these aforementioned methods were not effective screening tools for bladder cancer [31]. Kinde et al. found that approximately 66% of patients with muscle-invasive BC carried TERT promoter activating mutations, which can be detected in urine and are strongly associated with BC recurrence, suggesting that TERT promoter mutations could serve as a useful marker for early detection and monitoring of BC (Fig. 2) [32]. Regarding cystoscopy, some scholars believe that it is still the ultimate basis for diagnosis [33]. In addition to the above mentioned techniques, alternative approaches are currently available to identify BC in individuals with SCI.
Konety [34] measured the urinary nuclear matrix protein BLCA-4 in the urine of healthy individuals, patients diagnosed with BC, and patients with SCI. The study revealed that 53 of 55 (96.36%) BC patients and 38 of 202 (18.81%) SCI patients had BLCA-4 levels that exceeded the defined limit (Fig. 2). Despite the absence of a connection between increased BLCA-4 levels and indwelling catheters, chronic bladder inflammation, and urinary tract infections, the presence of BLCA-4 in the urine holds great diagnostic promise. And, hopefully, it could serve as a valuable method for the early identification of BC in individuals with SCI.
In summary, various screening techniques exist for individuals with SCI in conjunction with BC, although a standard and universally recognized protocol is yet to be established. The presence of hematuria, back pain resulting from ureteral obstruction, recurrent urinary tract infections, or the identification of a pelvic mass during physical examination in individuals with SCI signifies a significant risk factor for bladder cancer. Consequently, it is imperative that these patients undergo routine screening procedures.
Molecular mechanismsNitric oxide (NO)The human body relies on NO for its vital biological functions, serving as neurotransmitter and other transmitters. For example, NO plays the role of messenger molecule, and when vascular pressure increases, it increases NO release by activating Ca + in endothelial cells, and then plays the role of dilating blood vessels [35]. NO also can act as a retrograde neurotransmitter. Glutamate activates N-methyl-d-aspartate receptor (NMDAR) to import Ca 2 + into the cell, and then generates nitric oxide. This is a reverse neurotransmitter that maintains glutamate secretion at the presynaptic terminals [36].
It contributes to vasodilation and prevention of platelet aggregation by enhancing guanylate-activating enzyme activity, which results in elevated levels of cyclic-geranyl phosphate (cGMP) [37]. Furthermore, NO has a significant impact on inflammation and cancer. Urinary tract infections cause the secretion of IL-6 and IL-8 by urinary tract epithelial cells, facilitating the migration of neutrophils to the infected region. Frequent urinary bladder inflammation, which occurs due to the presence of catheters in patients with SCI, is commonly accompanied by infiltration of cells that cause inflammation. Macrophages and neutrophils in inflammatory tissues have been found to produce inducible NO synthase (iNOS) (Fig. 2) [38]. Gecit et al. [39] found that the concentrations of harmful substances malondialdehyde, NO, and prolyl peptidase were elevated in cancerous tissues compared to non-tumor tissues. While, In contrast, the concentrations of beneficial substances superoxide dismutase, glutathione, and glutathione peroxidase were decreased compared to non-tumor tissues.
NO inhibit or promotes tumor growth depending on the concentration, duration of action, and tumor microenvironment, and shares similarities with oxygen radicals within the human body, thereby inducing oxidative and nitrosative DNA damage [40]. Consequently, this molecule can result in alterations in DNA sequence and impairment of DNA repair mechanisms [41, 42], ultimately contributing to the development of BC when acting over an extended period.
MiR-1949 and Rb1MiRNAs, also known as microRNAs, are natural non-coding RNAs that primarily function by attaching to the 3’-untranslated region of target mRNAs. MiRNA Regulates many cellular activities, including proliferation, migration, differentiation, and cell apoptosis [43]. The retinoblastoma (RB) gene is the first oncogene identified to date. This protein, which is phosphorylated by nuclear processes, controls the progression of cell cycle. Numerous research studies have indicated that deactivation of the RB gene is crucial in the formation of numerous tumors, such as retinoblastoma [44].
Furthermore, the expression of miRNAs in the rat bladder was studied after SCI, revealing a significant dysregulation in miR-1949 expression (Fig. 2). Through the utilization of TargetScan that a software used for the prediction of miRNA binding sites in mammals, the identification of the target gene miR-1949 revealed its potential involvement in the regulatory processes of Rb1. The specific regulatory role of miR-1949 in Rb1 was explored using qRT PCR, and it was observed that Rb1 expression was likely to be inhibited by miR-1949 translation. The findings suggest that miR-1949 may suppress Rb1, a target gene, potentially causing oncogenic effects. According to the above review, miR-1949 and Rb 1 may be associated with this disease, but there are few studies on its further step. We can only presumably infer that the mechanism of bladder cancer in SCI patients is related to the above, but the detailed mechanism needs further study. And perhaps researchers can continue to explore upper and downstream of molecules and related pathways and to understand how miRNAs promotes the development of bladder cancer after SCI.
Fig. 2
A sketch of the pathogenesis: bladder cancer in patients with spinal cord injury
留言 (0)