
記住我



A major contributor to the pain experienced by a patient after abdominal surgery is the incision made in the abdominal wall [1]. Almost 80% of patients undergoing surgery experience postoperative pain, and 80% of them reported moderate-to-severe pain intensity [2].
Failure to control postoperative pain causes significant clinical effects on the pediatric patient’s daily activities [3]. Children who experience significant postoperative pain experience slower recovery and increased postoperative morbidity, including poor oral intake, sleep disturbances, and behavioral changes [4]. This has led to regional analgesic approaches gaining tremendous popularity as crucial elements of postoperative analgesia regimens [5]. Evidence suggests that pain control achieved by regional blocks is at least comparable and, in many cases, superior to the intravenous techniques [6]. There is also greater hemodynamic stability, improved gastrointestinal function, less nausea and vomiting, and a reduced neurohumeral stress response [7]. Epidural block (EB) is a well-established and commonly performed neuraxial technique for providing intraoperative and postoperative analgesia to pediatric patients scheduled for lower abdominoperineal surgical interventions [8, 9]. Although the efficacy and safety of EB are fairly high [10], associated complications such as inadvertent dural puncture, unwarranted motor blockade of the lower limbs, and disturbance of bladder function might limit its use [11]. Ultrasound guided quadratus lumborum block (QLB) is a relatively new local anesthetic technique that provides perioperative somatic, perhaps even visceral, analgesia for patients of all ages, including pediatric patients, undergoing abdominal or hip surgery. The assumption is that a local anesthetic injected adjacently into the quadratus lumborum muscle will spread in a medial and cranial direction under the crura and arcuate ligaments of the diaphragm, and then into the thoracic paravertebral space (PVS) [12, 13]. In the current study, we hypothesized that QL block would be comparable to EB as an effective analgesia alternative with fewer side effects.
Patients &methodsThis prospective, randomized, double-blinded comparative study was conducted at Mansoura University Children’s Hospital (MUCH) between 2020 and 2022 after the approval of the Institutional Review Board (IRB) (IRB code number MS.20.06.1159). The study was registered on the Pan African Clinical Trials Registry (PACTR) (ID: PACTR202203906027106; date: 23/03/2022). Informed written consent was obtained from all patients’ parents. This trial was performed according to the ethical principles of the Declaration of Helsinki (2013) and was conduced in harmony with good clinical practice. Patients of both sexes aged between 2 and 7 years with American Society of Anesthesiologists (ASA) physical status I or II scheduled for abdominal surgery were included in the study. Patients with preexisting hepatic diseases, coagulation disorders, infection at the site of needle insertion, known allergies to bupivacaine, or parents’ refusal of consent were excluded from the study. All patients were subjected to preoperative assessment, and CHEOPS (14) was explained to all patients’ parents on the previous day of operation to cooperate with assessors to evaluate the postoperative pain score. CHEOPS includes six categories of pain behavior: cry, facial, verbal, torso, touch, and legs. Each is scored separately (ranging from 0 to 2 or 1–3) and calculated for a pain score ranging from 4 to 13, with a minimum score of 4 points (no pain) and the maximum being 13 points (most awful pain). After application of standard anesthesia monitoring (electrocardiogram, non-invasive blood pressure, oxygen saturation), general anesthesia was induced with propofol (2 mg/kg), fentanyl (1 µg/kg) and atracurium (0.5 mg/kg for intubation and 0.1 mg/kg for maintenance as needed). An endotracheal tube was used to secure the airway. Anesthesia was maintained using 2% sevoflurane in a 50% air-oxygen mixture. The children were randomly allocated to either the epidural group (group E ) or the quadratus lumborum group (group QL). Group E (N = 29 patients) received 0.5 ml/kg of 0.25% bupivacaine for epidural block. Group QL: (N = 29 patients) received 0.5 ml/kg of 0.25% bupivacaine for quadratus lumborum block. Randomization concealment was performed using opaque sealed envelopes. The patient identifiers were attached to the opened envelopes and secured by a dedicated person who was independent of the randomization proceedings. This was a double-blinded study in which both anesthetist responsible for data collection and responsible patients’ parents included in the study were blinded to group allocation. All patients were positioned in the lateral position with the hips fully flexed, sterilized, and covered with sterile sheets. Aseptic precautions were taken by wearing sterile gowns and gloves. A utrasound machine (VINNO Technology Co., Ltd., Suzhou, China) with a high-frequency (6.5–18 MHz) linear transducer (X6–16 L) was used. A uniform dressing for all patients after injection, regardless of the group, was used to maintain the blindness of the type of intervention.
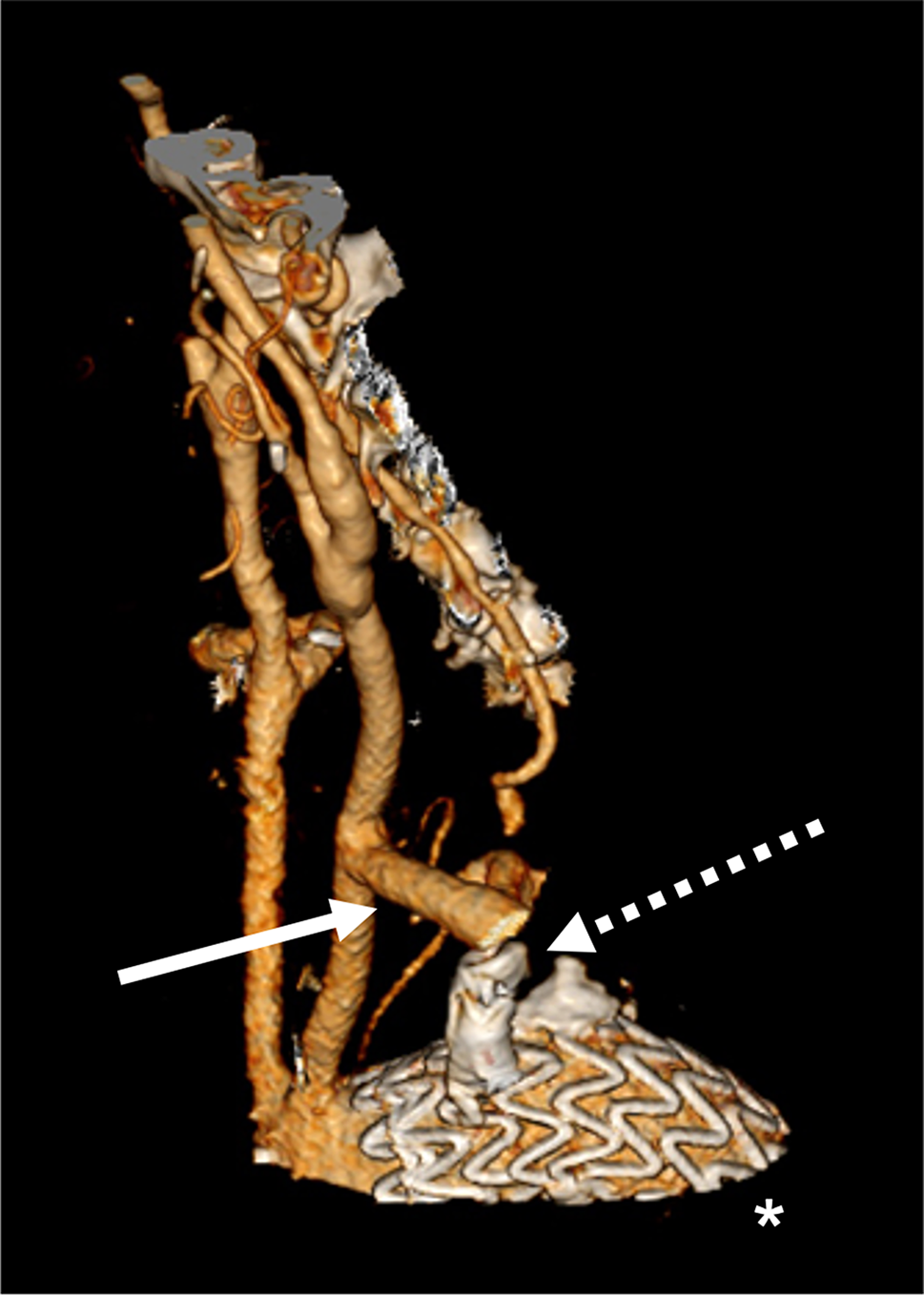
Ultrasound guided epidural block techniqueA high-frequency probe was used to scan from the sacral to the thoracic level and to confirm the target level. After selecting a puncture site (T12-L1), the distance from the skin to the ligamentum flavum was measured in the paramedian view to serve as a reference during needle insertion. Following sterile preparation, the assistant positioned the US probe superior to the puncture site in the paramedian plane to visualize the hyperechoic dura mater and ligamentum flavum, enabling free use of both hands by the operator. The needle was angulated in a cephalad direction to locate the needle tip within the epidural space (Fig. 1). When the needle tip was observed to pass through the ligamentum flavum and enter the epidural space on US images, its position was confirmed by the air-loss of resistance (LOR) technique. After the LOR test, when a small volume of saline or local anesthetic was injected, ventral displacement of the dura mater and widening of the epidural space could be observed on US images. We then injected 0.5 ml/kg bupivacaine 0.25%.
Fig. 1
Ultrasound guided epidural block. *: site of injection
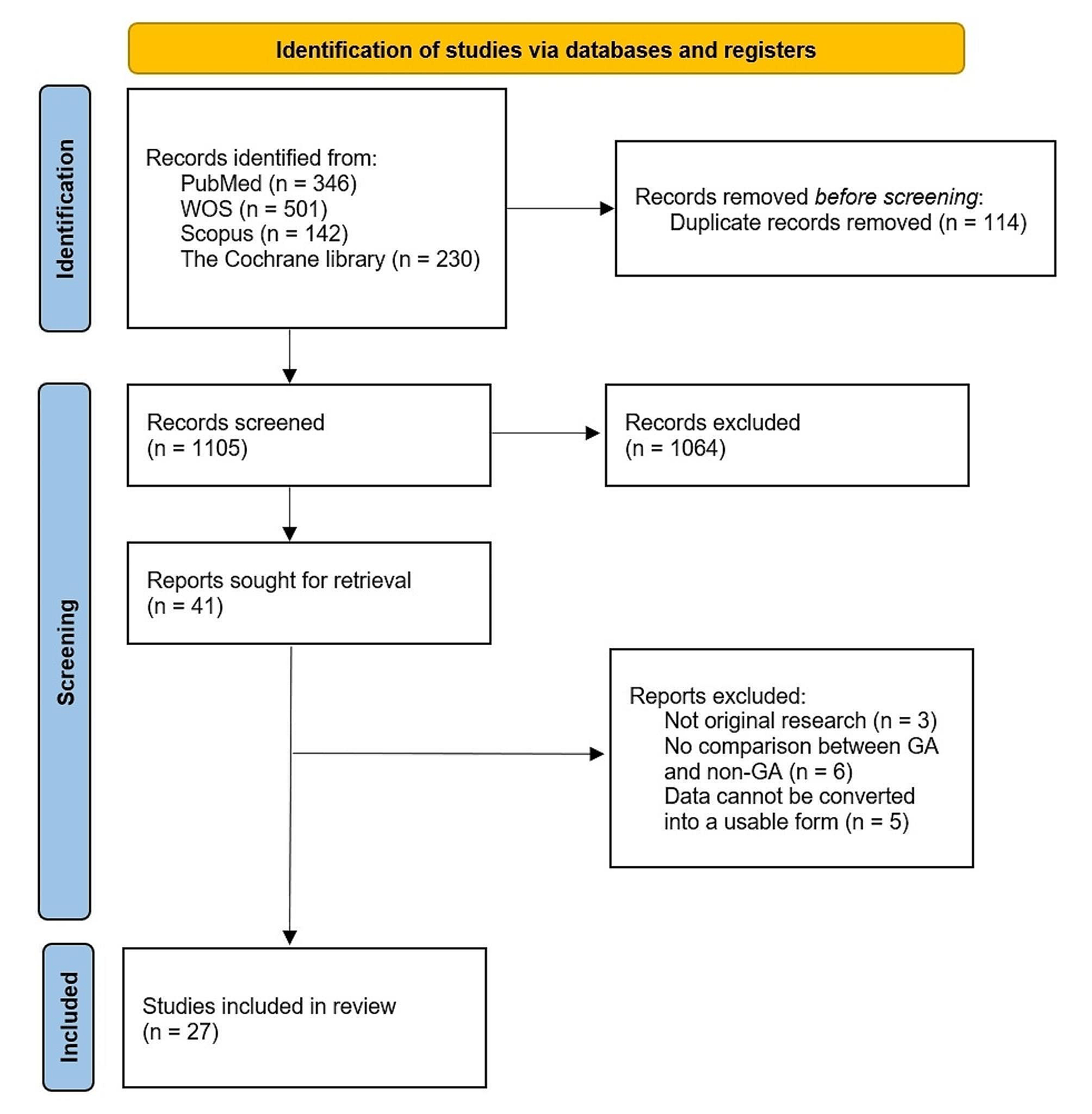
Ultrasound guided quadratus lumborum block techniqueThe probe was placed in the mid-axillary line cranially to the iliac crest to identify the three muscles of the anterior abdominal wall (transversus abdominis, internal oblique, and external oblique), then scanned dorsally, keeping the transverse orientation, until it was observed that the transversus abdominis muscle became aponeurotic. This aponeurosis was followed until the QL muscle was clearly visualized with its attachment to the lateral edge of the transverse process of L4 and psoas muscle. The needle was inserted in-plane from anterior to posterior, and its tip was advanced toward the anterior border of the QL muscle. Between the QL and psoas muscles, a 1 ml test dose of saline was injected to confirm the correct needle-tip position, and then this was followed by an injection of 0.5 ml/kg of 0.25% bupivacaine (Fig. 2). Bilateral injection was performed for midline incisions and unilateral injection for paramedian incisions. At the end of surgery, inhalational anesthesia was discontinued, and neuromuscular block was reversed with neostigmine (0.04 mg/kg) and atropine (0.02 mg/kg). Extubation was performed when patients had fulfilled the required criteria, and then patients were transferred to the post-anesthesia care unit (PACU). All patients received postoperative paracetamol intravenously (i.v.) as routine analgesia (10 mg/kg/8 h) considering the first dose at the end of surgery. Fentanyl i.v. (1 µg/kg/dose) was given as rescue analgesia for patients in the two study groups if the CHEOPS pain score ≥ 5. Assessment of the postoperative total fentanyl consumption was the primary outcome, while the secondary outcomes were the assessment of postoperative pain by the Children’s Hospital of Eastern Ontario Pain Scale (CHEOPS) 0 (immediate postoperative), 6, 12, 18, and 24 h post-operatively., the time of the first analgesic request, the occurrence of complications such as nausea, vomiting, and dural puncture, and the patient’s parents’ satisfaction regarding the analgesia.
Fig. 2
Ultrasound guided quadratus lumborum block. *****: site of injection. QL: quadratus lumborum; EO: externak oblique; IO: internal oblique; TA: transversus abdominis; LD: latismus dorsi
Sample size calculation and statistical analysisSample size was calculated using G*Power software version 3.1.9.7, using the results published by Ipek et al. (15) comparing the rescue analgesia requirement dosage in pediatric patients receiving either caudal epidural block or quadratus lumborum block for lower abdominal surgery under general anesthesia as the primary outcome. A sample size of 23 patients in each group was needed to achieve 90% power using a two-sided, two-sample equal-variance t-test with a significance level of (α 0.05). The total number was increased to 30 patients per group to compensate for possible dropouts. IBM’s SPSS statistics (Statistical Package for the Social Sciences) for Windows (version 22) were used for statistical analysis of the collected data. The Shapiro-Wilk test was used to check the normality of the data distribution. Normally distributed continuous variables were expressed as mean ± SD, while categorical variables and the non-normally distributed continuous ones were expressed as median and range, or number and percentage (as appropriate). The Student t test and Mann-Whitney were used for normally and non-normally distributed continuous data, respectively. The chi square test was used for categorical data using the crosstabs analysis. All tests were conducted with a 95% confidence interval. A P (probability) value < 0.05 was considered statistically significant.
留言 (0)