
記住我



Trichorhinophalangeal syndrome 1 (TRPS1), also termed transcriptional repressor GATA binding 1, is an atypical GATA nuclear transcription factor that mainly acts as a transcriptional repressor protein that can prevent the expression of GATA1-6-regulated genes (summarized1). For example, Runx1 and Sox9, which both are GATA3 regulated and required for cartilage formation, are suppressed by TRPS1.2,3 Multiple germline mutations of the TRPS1 gene were found to cause craniofacial and skeletal malformations.4 TRPS1 can also induce the expression of cancer-related genes, such as, for example, FOXA1, which is a negative regulator of epithelial-mesenchymal transition.5 Functional studies in cancer cells have suggested a tumor-suppressive activity of TRPS1 by preventing epithelial-mesenchymal transition,5,6 as well as a role of TRPS1 in breast cancer angiogenesis7 and in multidrug resistance of breast cancer8 and osteosarcoma.9
In normal tissues, TRPS1 is expressed in numerous cell types but expression is highest in breast epithelial cells (https://www.proteinatlas.org/ENSG00000104447-TRPS1). Because TRPS1 expression is often retained in cells that undergo malignant transformation, TRPS1 immunohistochemistry (IHC) has been suggested to represent a useful tool for the distinction of breast cancer from other cancer types in metastatic tissue.10,11 However, TRPS1 expression has recently also been described in various salivary gland tumors,10,12–14 endometrial carcinoma,15 hepatocellular carcinoma,16 colorectal cancer,17 gastric cancer,18 squamous cell carcinoma of the skin,19 synovial sarcoma,20 and osteosarcoma,21 as well as in lung22 and prostate cancer cell lines.23,24 In carcinomas of the breast,25 colon,17 and stomach,18 as well as in osteosarcoma,21 TRPS1 expression levels were associated with parameters of cancer aggressiveness. Altogether, the available data suggest a diagnostic and prognostic potential of TRPS1 IHC analysis which may be enhanced by a combination with GATA3, another commonly used breast cancer marker.10,26,27 However, many tumor entities have, so far, not been examined for TRPS1 by IHC and a systematic evaluation of different tumor entities for TRPS1 protein expression is so far lacking.
To better understand the prevalence and potential role of TRPS1 protein expression in tumors and to elucidate the potential diagnostic utility of TRPS1 IHC alone and in combination with GATA3, a survey of TRPS1 immunostaining in a broad range of tumor types is needed. In this study, we, therefore, evaluated TRPS1 expression in more than 19,000 tumor samples from 152 tumor types and subtypes for which GATA3 data were available in a tissue microarray (TMA) format.
MATERIALS AND METHODS Tissue MicroarraysOur normal tissue TMA was composed of 8 samples from 8 different donors for each of 76 different normal tissue types (608 samples on one slide). The tumor TMAs contained a total of 19,201 primary tumors from 152 tumor types and subtypes. Detailed histopathological data on grade, pathologic tumor stage, pathologic lymph node status, and molecular data were available from 3173 tumors (1680 invasive breast carcinomas of no special type, 40 endometrioid and 369 serous ovarian carcinomas, 182 endometrioid endometrium carcinomas, and 902 squamous cell carcinomas). Clinical follow-up data were available from 877 invasive breast carcinomas of no special type with a median follow-up time of 49 months (range: 1 to 88 mo). Data on GATA3 were available for 15,964 tumors from an earlier study evaluating a large subset of our TMAs.28 The composition of both normal and tumor TMAs is described in detail in the results section. Samples were from the archives of the Institutes of Pathology, University Hospital of Hamburg, Germany, the Institute of Pathology, Clinical Center Osnabrueck, Germany, and Department of Pathology, Academic Hospital Fuerth, Germany. Tissues were fixed in 4% buffered formalin and then embedded in paraffin. TMA tissue spot diameter was 0.6 mm. The use of archived remnants of diagnostic tissues for manufacturing of TMAs and their analysis for research purposes, as well as patient data analysis, has been approved by local laws (HmbKHG, §12) and by the local ethics committee (Ethics Commission Hamburg, WF-049/09). All work has been carried out in compliance with the Helsinki Declaration.
ImmunohistochemistryFreshly cut TMA sections were immunostained on 1 day and in 1 experiment. Slides were deparaffinized with xylol at room temperature for 3×5 minutes, rehydrated through a graded alcohol series, and exposed to heat-induced antigen retrieval for 5 minutes in an autoclave at 121°C in pH 7.8, Dako Target Retrieval Solution (Agilent; #S2367). Endogenous peroxidase activity was blocked with Dako Peroxidase Blocking Solution (Agilent; #52023) for 10 minutes. A primary antibody specific for TRPS1 (rabbit recombinant monoclonal, MSVA-512R, MS Validated Antibodies; 5676-512R) was applied at 37°C for 60 minutes at a dilution of 1:20 for our normal tissue TMA and 1:300 for cancer tissues. For the purpose of validating and comparing antibodies, the normal tissue TMA and a subset of 2214 cancer tissues (666 breast cancers and 1191 non-breast cancers, including 622 non-breast adenocarcinomas) were also analyzed by the rabbit recombinant monoclonal TRPS1 antibody EPR16171 (#ab209664, Abcam) at a dilution of 1:2000 and by the rabbit polyclonal TRPS1 antibody PA5-84874 (Invitrogen/ThermoFisher) at a dilution of 1:100 with an otherwise identical protocol. Bound antibody was then visualized using the EnVision Kit (Agilent; #K5007) according to the manufacturer’s directions. The sections were counterstained with haemalaun. For tumor tissues, the percentage of positive neoplastic cells was estimated, and the staining intensity was semiquantitatively recorded (0, 1+, 2+, and 3+). For statistical analyses, the staining results were categorized into 4 groups. Tumors without any staining were considered negative. Tumors with 1+ staining intensity in ≤70% of tumor cells and 2+ intensity in ≤30% of tumor cells were considered weakly positive. Tumors with 1+ staining intensity in >70% of tumor cells, 2+ intensity in 31% to 70%, or 3+ intensity in ≤30% were considered moderately positive. Tumors with 2+ intensity in >70% or 3+ intensity in >30% of tumor cells were considered strongly positive. This scoring system has been used in numerous TMA studies and led to the identification of numerous known and novel prognostic molecular features in various tumor types.29–32
StatisticsStatistical calculations were performed with JMP 17 software (SAS Institute Inc.). Contingency tables and the χ² test were performed to search for associations between TRPS1 immunostaining and tumor phenotype. Survival curves were calculated according to Kaplan-Meier. The log-rank test was applied to detect significant differences between groups. Sensitivity and specificity for the detection of breast cancers were calculated according to the following formulas: sensitivity=number of true positives divided by the number of true positives plus number of false negatives; specificity=number of true negatives divided by the number of true negatives plus number of false positives.
RESULTS Technical IssuesA total of 16,818 (87.6%) of 19,201 tumor samples were interpretable in our TMA analysis. Noninterpretable samples demonstrated either a lack of unequivocal tumor cells or loss of the tissue spots during technical procedures. At least 4 samples of each normal tissue type were evaluated.
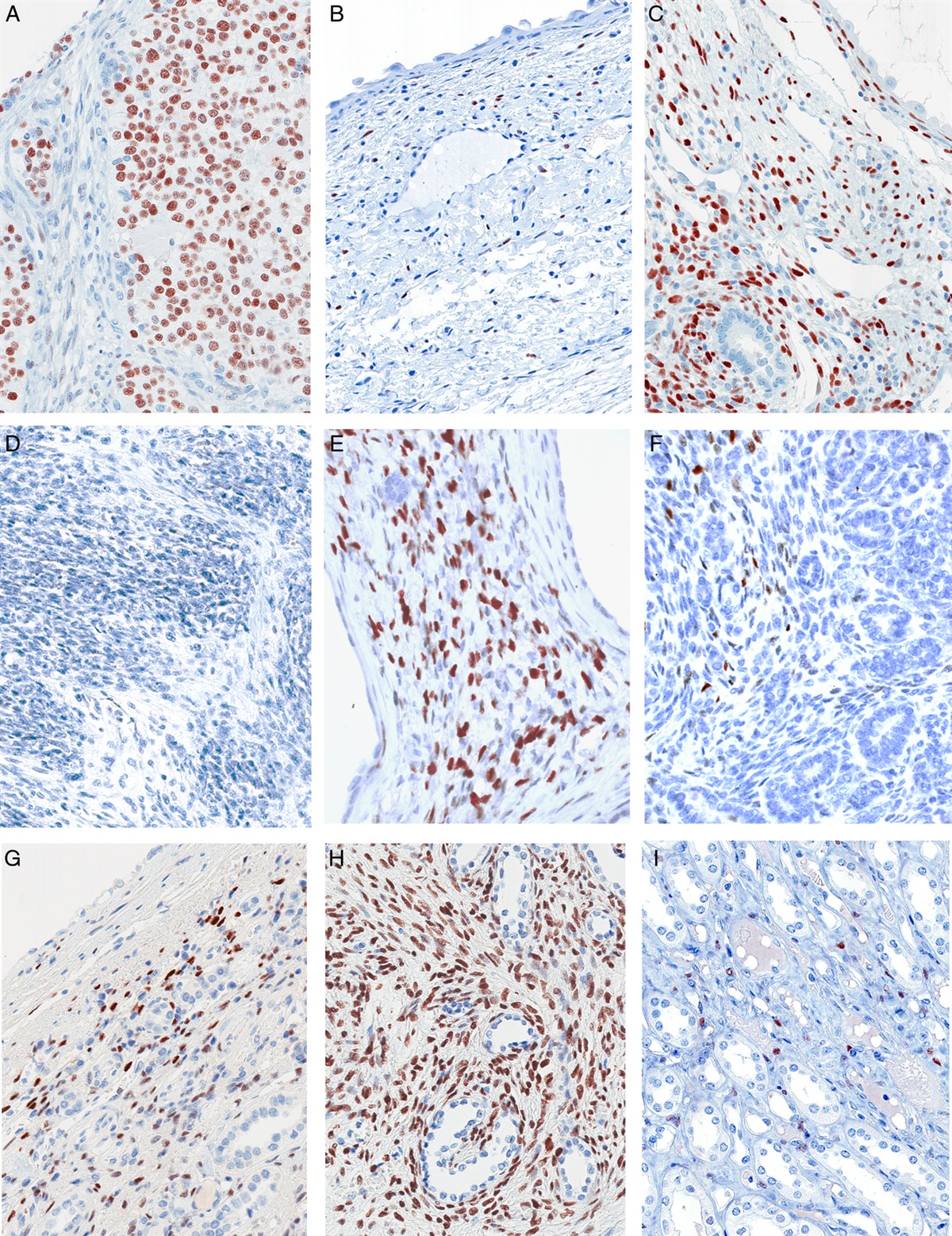
TRPS1 in Normal TissuesTRPS1 staining was always nuclear and strongest in luminal epithelial cells of breast glands. A moderate to strong nuclear staining was also observed in epithelial cells of the endometrium (stroma cells were also positive, but weaker), glial cells of the brain, sebaceous glands, and suprabasal cells of non-keratinizing squamous epithelium. A weak to moderate TRPS1 positivity was observed in various other epithelial (salivary glands, gallbladder, fallopian tube, respiratory epithelium, renal tubuli, amnion, thyroid gland, and parathyroid gland), muscular (smooth muscle and myometrium), neuronal (ganglion cells in the intestine), and germinal (spermatogonia) cell types. In other organs, TRPS1 staining of epithelial cells was only occasionally detected, such as, for example, in atrophic acinar cells of the prostate. A nuclear TRPS1 staining of variable intensity was also regularly seen in stromal cells of various tissues, especially in the case of tissue reparation (probably fibroblasts). Representative images are shown in Figure 1. A similar nuclear staining was observed in all these cell types when the anti-TRPS1 antibody EPR16171 was used (Supplemental Fig. 1, Supplemental Digital Content 1, https://links.lww.com/PAS/B785). As compared with MSVA-512R, EPR16171 resulted in additional cytoplasmic staining in basal cells of several non-keratizing squamous epithelia (Supplemental Fig. 1, Supplemental Digital Content 1, https://links.lww.com/PAS/B785), whereas PA-84874 showed significant additional cytoplasmic staining in many different normal tissues, including, for example, smooth muscle cells, kinocilia of the epididymis, parietal cells of the stomach, and lymphocytes, as well as nuclear staining in Leydig cells of the testis (Supplemental Fig. 2, Supplemental Digital Content 2, https://links.lww.com/PAS/B786). The additional stainings observed with EPR16171 and PA-84874 were considered antibody-specific cross-reactivities.
 FIGURE 1:
FIGURE 1: TRPS1 immunostaining of normal tissues. The panels show a strong nuclear staining of breast epithelial cells (A) epithelial cells of the endometrium (B), and glial cells in the brain (C). Variable nuclear staining also occurred in suprabasal cells of esophageal squamous epithelium (D), sebaceous glands of the skin (E), epithelial cells of the fallopian tube (F), atrophic epithelial cells of the prostate (G), some tubular cells of the kidney (H), spermatogonia of the testis (I), epithelial cells of the gallbladder (J), smooth muscle cells of the appendix (K), and amnion cells (L).
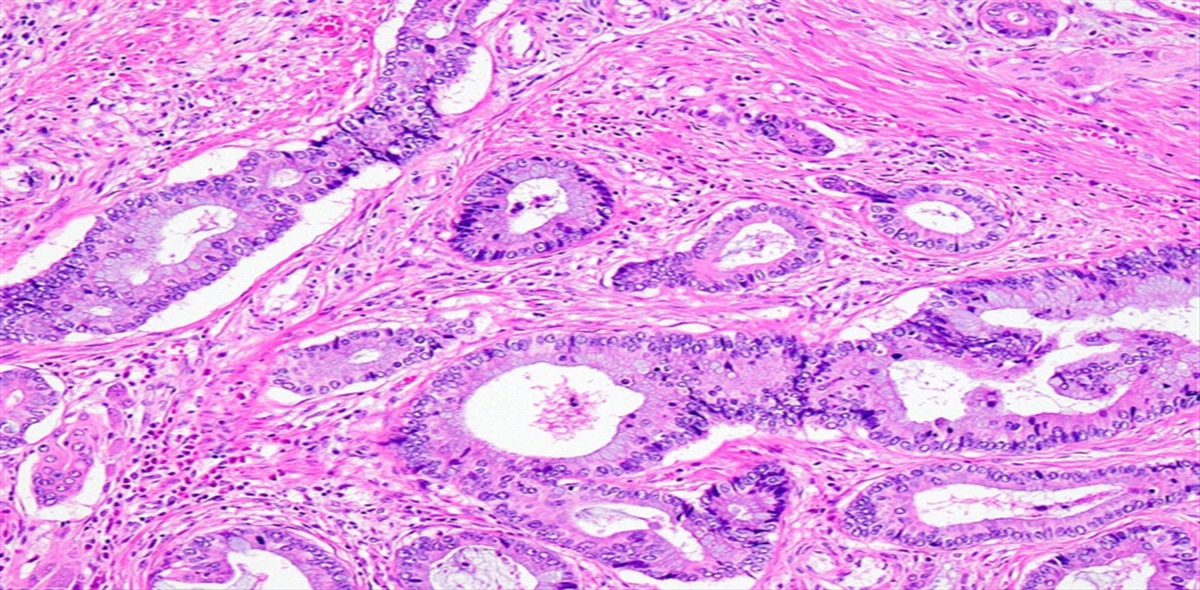
TRPS1 in Tumor TissuesTRPS1 immunostaining was detectable in 2482 (14.8%) of the 16,818 analyzable tumors, including 614 (3.7%) with weak, 800 (4.8%) with moderate, and 1068 (6.4%) with strong immunostaining. Overall, 86 (56.6%) of 152 tumor categories showed TRPS1 positivity with 36 (23.7%) tumor categories including at least one case with strong staining (Table 1). The highest rate of TRPS1 positivity was found in various types of breast cancers (51.4% to 100%), soft tissue tumors (up to 100%), salivary gland tumors (up to 46.2%), squamous cell carcinomas of various sites of origin (up to 34.7%), and in diverse gynecological cancers (up to 40.0%). TRPS1 positivity only occurred in 1.8% of 1083 urothelial neoplasms. Representative images are shown in Figure 2. A ranking order of TRPS1-positive and strongly positive tumors is given in Figure 3. The relationship between TRPS1 expression and clinically important histopathological and molecular tumor features in breast cancer, ovarian cancer, endometrial carcinoma, and squamous cell carcinomas from different sites is shown in Table 2. In invasive breast cancer of no special type, low TRPS1 expression was linked to high grade (P = 0.0547), advanced pathologic tumor stage (P < 0.0001), nodal metastasis (P = 0.0571), loss of estrogen receptor expression (P < 0.0001), loss of progesterone receptor expression (P < 0.0001), and triple-negative status (P < 0.0001) but was unrelated to overall patient survival (P = 0.8016; Supplemental Fig 4, Supplemental Digital Content 3, https://links.lww.com/PAS/B787). A combined analysis of 677 squamous cell carcinomas from 11 different sites did not reveal associations between TRPS1 expression and tumor phenotype. TRPS1 expression was also unrelated to human papillomavirus infection status (P = 0.1159; Supplemental Table 1, Supplemental Digital Content 4, https://links.lww.com/PAS/B788). In our prostate cancers, the rate of TRPS1 positivity increased from Gleason grade 3+3 (0%) to Gleason grade 5+5 (3.8%) and recurrent adenocarcinomas under therapy (7.6%; P = 0.0164). TRPS1 immunostaining was unrelated to the histopathological tumor phenotype in ovarian and endometrial cancer.
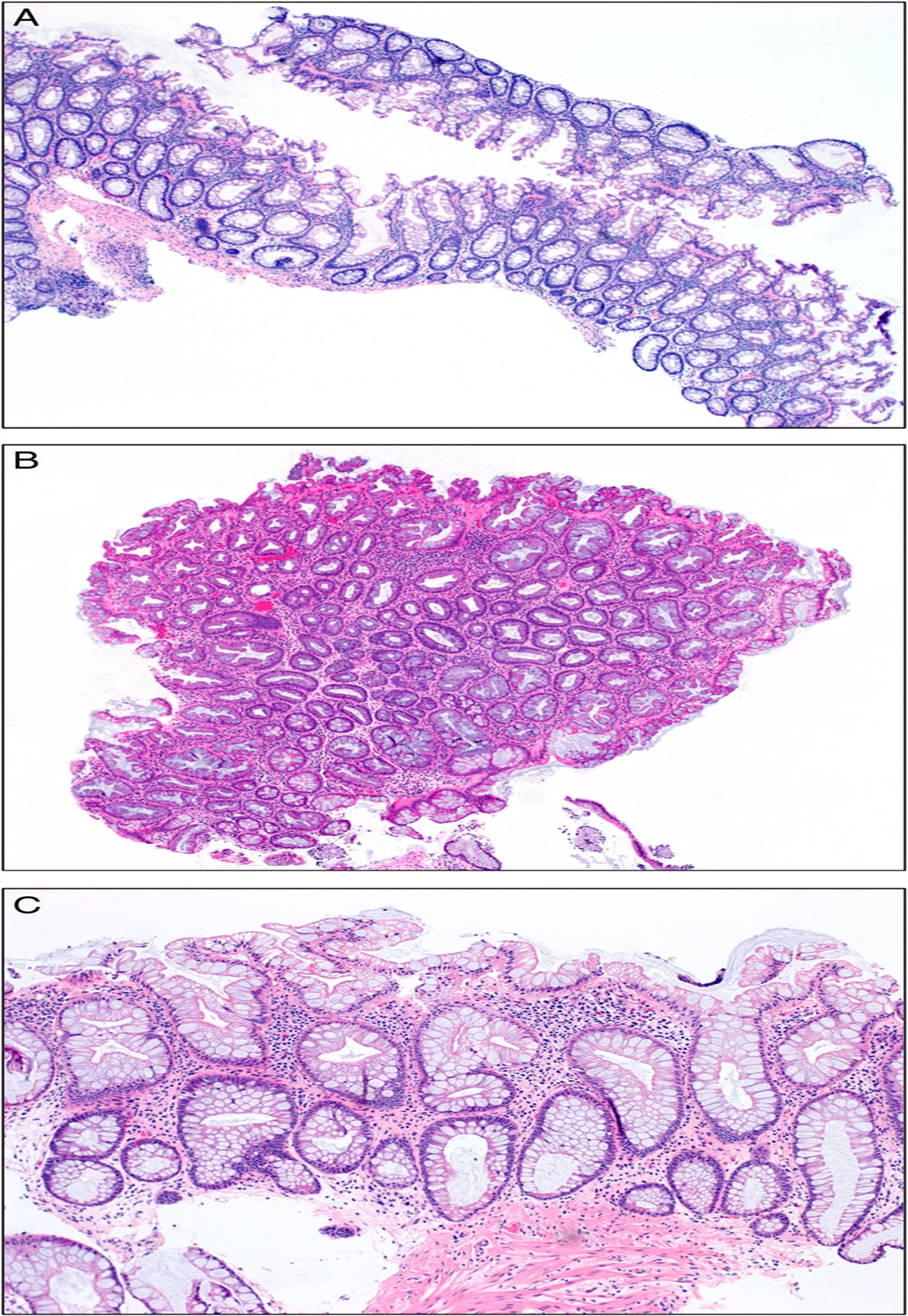
TABLE 1 - TRPS1 Immunostaining in Human Tumors TRPS1 immunostaining result Tumor entity On TMA (n) Analyzable (n) Negative (%) Weak (%) Moderate (%) Strong (%) Tumors of the skin Pilomatricoma 35 21 61.9 23.8 4.8 9.5 Basal cell carcinoma of the skin 89 54 96.3 1.9 1.9 0.0 Benign nevus 29 26 100.0 0.0 0.0 0.0 Squamous cell carcinoma of the skin 145 127 84.3 14.2 0.0 1.6 Malignant melanoma 65 59 98.3 1.7 0.0 0.0 Malignant melanoma Lymph node metastasis 86 72 100.0 0.0 0.0 0.0 Merkel cell carcinoma 48 28 100.0 0.0 0.0 0.0 Tumors of the head and neck Squamous cell carcinoma of the larynx 109 93 90.3 9.7 0.0 0.0 Squamous cell carcinoma of the pharynx 60 49 65.3 30.6 4.1 0.0 Oral squamous cell carcinoma (floor of the mouth) 130 107 75.7 22.4 0.9 0.9 Pleomorphic adenoma of the parotid gland 50 47 40.4 14.9 38.3 6.4 Warthin tumor of the parotid gland 104 98 100.0 0.0 0.0 0.0 Adenocarcinoma, NOS (papillary cystadenocarcinoma) 14 10 70.0 30.0 0.0 0.0 Salivary duct carcinoma 15 12 75.0 16.7 8.3 0.0 Acinic cell carcinoma of the salivary gland 181 146 97.9 0.7 0.7 0.7 Adenocarcinoma NOS of the salivary gland 109 87 89.7 3.4 3.4 3.4 Adenoid cystic carcinoma of the salivary gland 180 106 59.4 18.9 18.9 2.8 Basal cell adenocarcinoma of the salivary gland 25 21 81.0 14.3 0.0 4.8 Basal cell adenoma of the salivary gland 101 86 87.2 10.5 2.3 0.0 Epithelial-myoepithelial carcinoma of the salivary gland 53 51 58.8 9.8 23.5 7.8 Mucoepidermoid carcinoma of the salivary gland 343 295 92.9 3.7 3.1 0.3 Myoepithelial carcinoma of the salivary gland 21 18 61.1 16.7 16.7 5.6 Myoepithelioma of the salivary gland 11 9 66.7 0.0 33.3 0.0 Oncocytic carcinoma of the salivary gland 12 11 90.9 0.0 9.1 0.0 Polymorphous adenocarcinoma, low grade, of the salivary gland 41 26 53.8 19.2 19.2 7.7 Pleomorphic adenoma of the salivary gland 53 36 80.6 11.1 8.3 0.0 Tumors of the lung, pleura and thymus Adenocarcinoma of the lung 196 189 97.4 2.1 0.0 0.5 Squamous cell carcinoma of the lung 80 74 90.5 8.1 1.4 0.0 Small cell carcinoma of the lung 16 11 100.0 0.0 0.0 0.0 Mesothelioma, epithelioid 40 27 92.6 7.4 0.0 0.0 Mesothelioma, biphasic 77 48 91.7 4.2 4.2 0.0 Thymoma 29 28 96.4 3.6 0.0 0.0 Lung (NET) 29 28 96.4 0.0 3.6 0.0 Tumors of the female genital tract Squamous cell carcinoma of the vagina 78 61 90.2 3.3 3.3 3.3 Squamous cell carcinoma of the vulva 157 140 87.1 12.9 0.0 0.0 Squamous cell carcinoma of the cervix 136 124 96.8 1.6 0.8 0.8 Adenocarcinoma of the cervix 23 19 100.0 0.0 0.0 0.0 Endometrioid endometrial carcinoma 338 269 85.5 9.7 3.3 1.5 Endometrial serous carcinoma 86 60 83.3 15.0 1.7 0.0 Carcinosarcoma of the uterus 57 47 76.6 17.0 6.4 0.0 Endometrial carcinoma, high grade, G3 13 10 60.0 30.0 0.0 10.0 Endometrial clear cell carcinoma 9 8 100.0 0.0 0.0 0.0 Endometrioid carcinoma of the ovary 130 119 76.5 9.2 12.6 1.7 Serous carcinoma of the ovary 580 537 76.2 14.5 8.4 0.9 Mucinous carcinoma of the ovary 101 88 96.6 1.1 2.3 0.0 Clear cell carcinoma of the ovary 51 48 93.8 2.1 4.2 0.0 Carcinosarcoma of the ovary 47 46 71.7 21.7 6.5 0.0 Granulosa cell tumor of the ovary 44 37 100.0 0.0 0.0 0.0 Leydig cell tumor of the ovary 4 4 100.0 0.0 0.0 0.0 Sertoli cell tumor of the ovary 1 1 100.0 0.0 0.0 0.0 Sertoli Leydig cell tumor of the ovary 3 3 100.0 0.0 0.0 0.0 Steroid cell tumor of the ovary 3 3 100.0 0.0 0.0 0.0 Brenner tumor 41 38 100.0 0.0 0.0 0.0 Tumors of the breast Invasive breast carcinoma of no special type 1764 1533 11.1 7.1 29.5 52.3 Lobular carcinoma of the breast 363 304 8.9 6.6 30.9 53.6 Medullary carcinoma of the breast 34 27 14.8 25.9 33.3 25.9 Tubular carcinoma of the breast 29 18 0.0 5.6 44.4 50.0 Mucinous carcinoma of the breast 65 38 10.5 13.2 39.5 36.8 Phyllodes tumor of the breast 50 35 48.6 8.6 25.7 17.1 Tumors of the digestive system Adenomatous polyp, low-grade dysplasia 50 50 100.0 0.0 0.0 0.0 Adenomatous polyp, high-grade dysplasia 50 50 100.0 0.0 0.0 0.0 Adenocarcinoma of the colon 2483 2247 99.9 0.1 0.0 0.0 Gastric adenocarcinoma, diffuse type 215 198 99.5 0.0 0.5 0.0 Gastric adenocarcinoma, intestinal type 215 202 98.0 1.5 0.5 0.0 Gastric adenocarcinoma, mixed type 62 62 100.0 0.0 0.0 0.0 Adenocarcinoma of the esophagus 83
留言 (0)