OBJECTIVES:
To estimate the prevalence of suboptimal fluoroscopy of sacral outlet images due to anatomic and equipment dimensions. Pelvic retroversion is hypothesized to mitigate this issue.
METHODS:
Design:
In silico simulations using retrospectively collected computed tomography (CT) data from human patients.
Setting:
Level I trauma center.
Patient Selection Criteria:
Adults with OTA/AO 61 pelvic ring disruptions treated with posterior pelvic fixation between July and December 2021.
Outcome Measures and Comparisons:
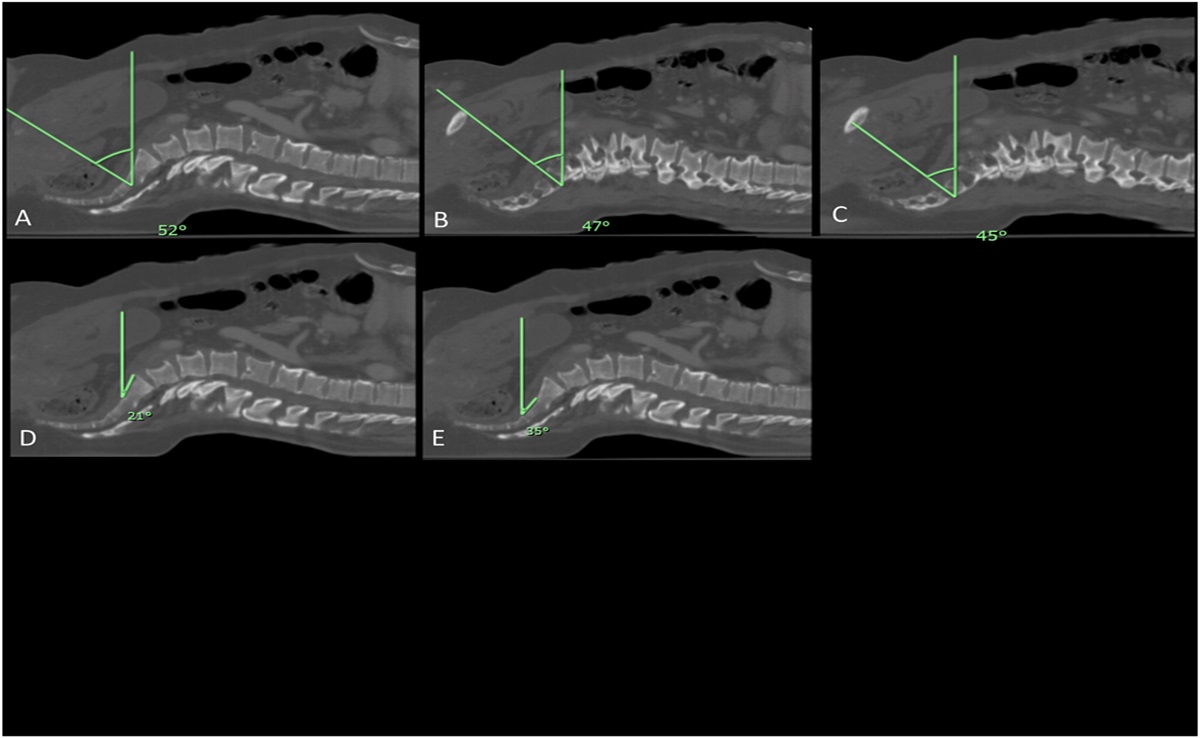
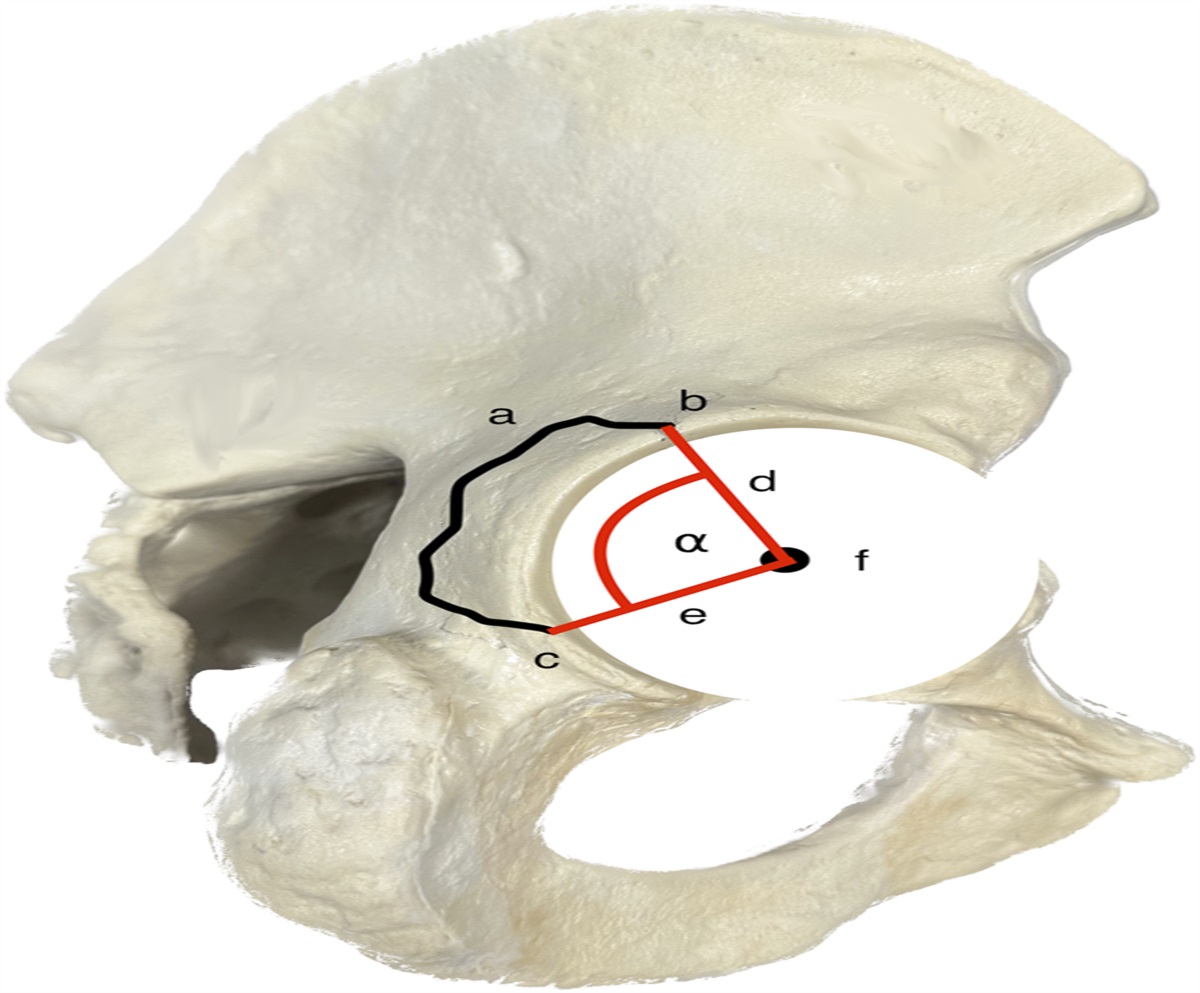
C-arm tilt angles required to obtain 3 optimal fluoroscopic sacral outlet images, defined as vectors from pubic symphysis to S2 and parallel to the first and second sacral neural foramina, were calculated from sagittal CT images. A suboptimal view was defined as collision of the C-arm radiation source or image intensifier with the patient/operating table at the required tilt angle simulated using the dimensions of 5 commercial C-arm models and trigonometric calculations. Incidence of suboptimal outlet views and pelvic retroversion necessary to obtain optimal views without collision, which may be obtained by placement of a sacral bump, was determined for each view for all patients and C-arm models.
RESULTS:
CT data from 72 adults were used. Collision between patient and C-arm would occur at the optimal tilt angle for 17% of simulations and at least 1 view in 68% of patients. Greater body mass index was associated with greater odds of suboptimal imaging (standard outlet: odds ratio [OR] 0.84, confidence interval [CI] 0.79–0.89, P < 0.001; S1: OR 0.91, CI 0.87–0.97, P = 0.002; S2: OR 0.85, CI 0.80–0.91, P < 0.001). S1 anterior sacral slope was associated with suboptimal S1 outlet views (OR 1.12, Cl 1.07–1.17, P < 0.001). S2 anterior sacral slope was associated with suboptimal standard outlet (OR 1.07, Cl 1.02–1.13, P = 0.004) and S2 outlet (OR 1.16, Cl 1.09–1.23, P < 0.001) views. Retroversion of the pelvis 15–20 degrees made optimal outlet views possible without collision in 95%–99% of all simulations, respectively.
CONCLUSIONS:
Suboptimal outlet imaging of the sacrum is associated with greater body mass index and sacral slope at S1 and S2. Retroversion of the pelvis by 15–20 degrees with a bump under the distal sacrum may offer a low-tech solution to ensure optimal fluoroscopic imaging for percutaneous fixation of the posterior pelvic ring.
LEVEL OF EVIDENCE:
Prognostic Level III. See Instructions for Authors for a complete description of levels of evidence.



留言 (0)