Although the white shark (also known as the great white shark) (Carcharodon carcharias) (which may reach lengths of 3.5 to 5.5 m) has a fearsome reputation, Australian data show that tiger shark (Galeocerdo cuvier) attacks are more likely to result in death. Specifically, while 38% of tiger shark and 32% of bull shark (Carcharhinus leucas) bites are fatal, only 25% of those due to white shark bites have resulted in death [11, 16]. Identification of the exact species after an attack may, however, sometimes be contentious [17] although both tooth morphology and calculated jaw shape may be useful [18]. Genetic investigations may also be used now to identify traces of shark DNA in the bite wounds of victims [19].
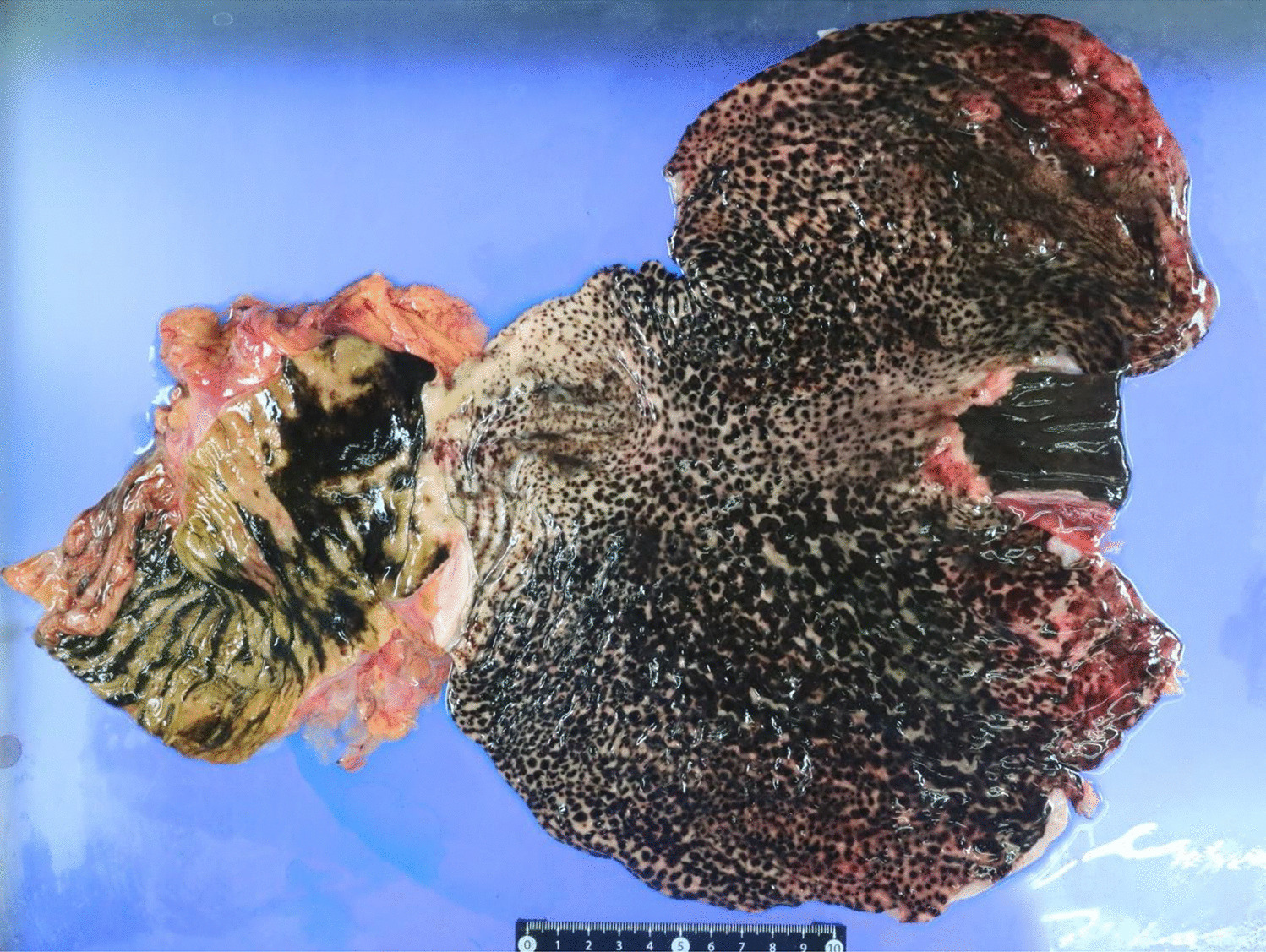
Injuries from shark attacks arise from a variety of mechanisms involving both blunt and sharp force trauma. Crushing and amputations occur due to the massive compressive forces from biting which in some species may reach up to 3300 kg/cm2 [20]. Penetrating and sharp force injuries result from a saw-like motion of the shark mouth with its rows of extremely sharp teeth [21] and a rolling or shaking movement of the head [22]. Problems in the evaluation of cases include failure to recover bodies, the damaging effects of putrefaction and post mortem animal feeding, and differentiating lethal wounds from those due to post mortem shark predation [14, 22,23,24]. In cases where a body has been literally torn apart by several sharks the only tissues available for examination may be aerated lung which has floated to the surface and subsequently been washed up along the shore [15].
Shark attacks vary from unproved to provoked, the latter where a shark may react to being approached in the water [4]. Unprovoked attacks may be so-called ‘bump and bite’ or ‘hit and run’ [25] possibly related to territorial instincts [13]. In the case of ‘bump and bite’ attacks a shark may knock into a victim before attacking which may leave characteristic abrasions from the rough scales (denticles) of the shark’s skin, unless there has been protection from a wet suit [13]. ‘Hit and run’ attacks are the most common, accounting for 80% of episodes and occurring usually in shallow water. This may be due to a swimmer being mistaken for a seal. In a ‘sneak’ attack a shark may attack unexpectedly without warning [25].
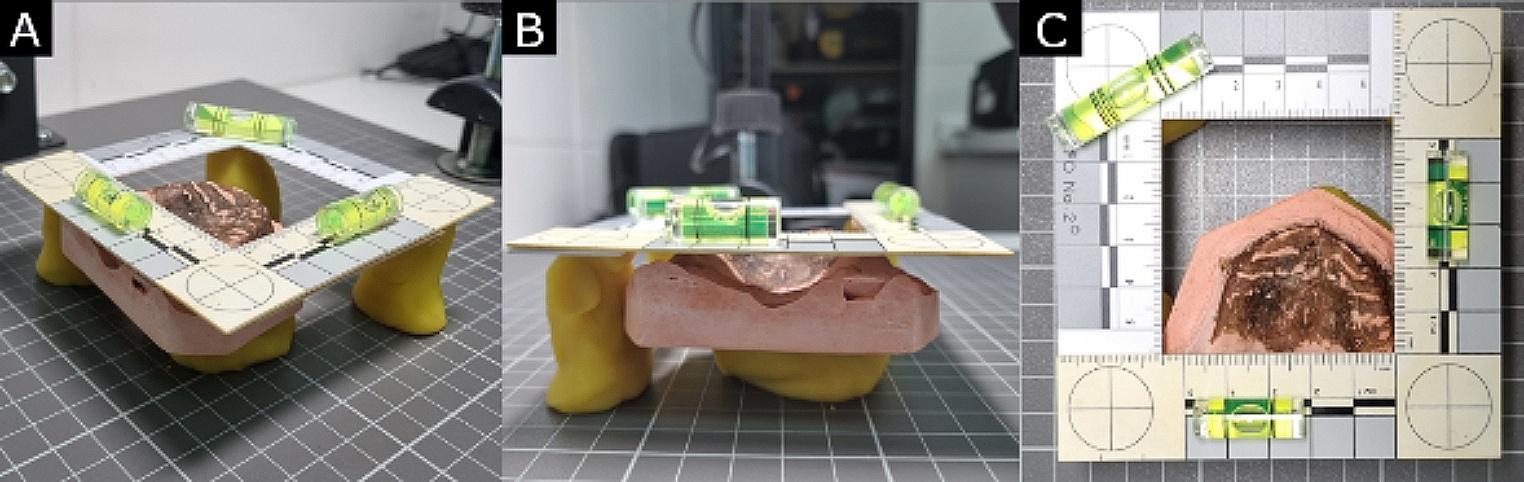
In the reported case, stripping of soft tissues from the right lower extremity below the groin was in keeping with the usual mode of attack with an approach from beneath [13]. It has been noted that 97% of victims have limb injuries [26]. The sharply incised edges of the wound without any abrasions and a triangular wound to the skin were typical of such events [13, 22]. Of interest, the triangular defect of the distal femur also paralleled this type of biting injury. The areas of shaving of the cortical bone demonstrated fine striations resulting from an oblique bite with dragging of the marginal serrations of the teeth of the shark. This enabled silicone castings to be made for permanent autopsy records. While serrations in bite marks may help to identify the species of shark involved, as in the current case, the type of serration is not unique to a particular animal and there are no predictable patterns in either their size or position; i.e. there can be no ‘teeth printing’ to identify a specific predator [16]. Although shark teeth are brittle and may chip or break off during an attack [22,23,24,25] no tooth fragments were identified in the reported case in bone or soft tissues, even with the application of a 3-dimensional volume rendering technique.
This case has demonstrated that high resolution post mortem CT scanning with 3-dimensional volume rendering visualisation in a case of fatal shark attack was able to clearly show the nature and number of the bony injuries. However, as the resolution was not high enough to demonstrate the fine parallel grooves from teeth serrations that were present at two sites, a formal pathological evaluation still complimented post mortem CT screening. While post mortem CT volume rendering technique did not identify fragments of teeth in the current cases it did provide a very useful technique to screen for such material particularly in residual traumatised soft tissues. Casting of bone lesions at autopsy may provide an additional record of a case.



留言 (0)