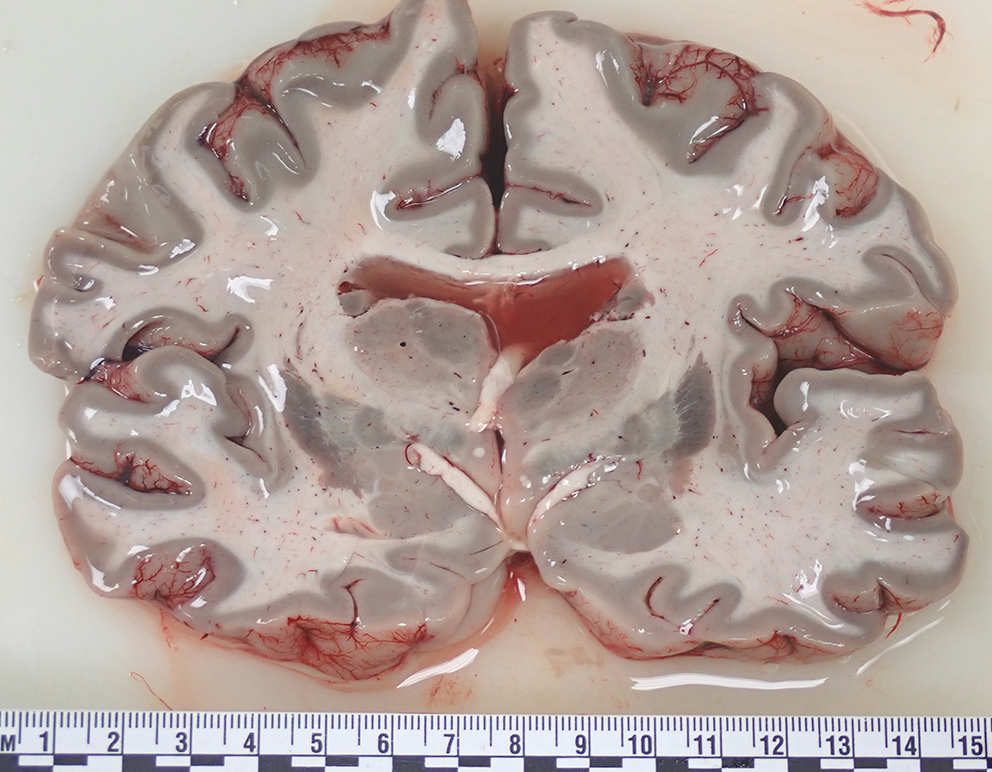
APS is an autoimmune condition that affects multiple endocrine organs concurrently resulting in progressive impairment of function over an often insidious course [1]. It was first described in 1926 by Schmidt, a German pathologist, in a patient with hypothyroidism and adrenal insufficiency with biopsies showing lymphocytic infiltration of the thyroid and adrenal glands [2]. In the reported case typical florid lymphocytic infiltration of the thyroid gland was present (Fig. 4).
APS has been divided into three types: APS type 1, APS type 2 and X-linked immunodysregulation, polyendocrinopathy, and enteropathy (IPEX), the features of which are summarized in Table 1 [1], The underlying mechanisms for APS remain unclear [3].
Table 1 Summary of the characteristics of different subtypes of APS. (Adapted from Husebye, Anderson, and Kämpe, 2018 [1]
The current case was an example of APS type 2 which may be characterized by at least two of three autoimmune conditions – Type 1 diabetes mellitus, autoimmune thyroid disease and Addison disease [4]. Similar to most autoimmune conditions, it occurs more commonly in females and may be associated with other autoimmune conditions such as celiac disease or autoimmune primary hypogonadism [1].
Given the number of organ systems that may be involved in this syndrome, APS type 2 can manifest in a myriad of ways, although pericarditis is a rare complication. Review of the literature reveals 13 affected patients who ranged in age from 21 to 54 years (mean 36.8 years) [3, 5,6,7,8,9,10,11,12,13,14]; there were no fatalities. Despite APS type 2 being more common in females, this particular manifestation seems to predominate in males with a ~ 2:1 ratio (8 males, 5 females), although the numbers are small.
In the reported cases treatment was undertaken with pericardiocentesis draining volumes of fluid ranging from 190-400mL [3, 5,6,7,8,9,10,11,12,13,14]. While these amounts may not necessarily cause hemodynamic instability [3], particularly if accumulation occurs slowly over time, the reported case had Addison disease with the likelihood of an impaired stress response [3]. In addition, a constrictive component has been described in pericardial efffusions in APS type 2 which may contribute to compromise of underlying myocardial function [13].
The reported patients all had autoimmune thyroid disease and adrenal insufficiency with two having evidence of autoimmune primary hypogonadism (both males) [7, 12]. None of the patients had T1DM although three (all male) had antibodies against glutamic acid decarboxylase-65 (GAD) [3, 8, 13]. One case had possible systemic lupus erythematosus (SLE) [10], and one had transglutaminase and endomysial antibodies, although with no biopsy-proven celiac disease [7].
In conclusion, a case of pericarditis with lethal cardiac tamponade secondary to APS type 2 is presented. The mechanism resulting in compromise of cardiac function involved space-occupying fluid within the pericardial sac impeding venous return to the heart and compressing cardiac chambers. A possible restrictive component may have been present against a background of Addison disease. Such cases should prompt careful evaluation of endocrine organs at autopsy.







留言 (0)