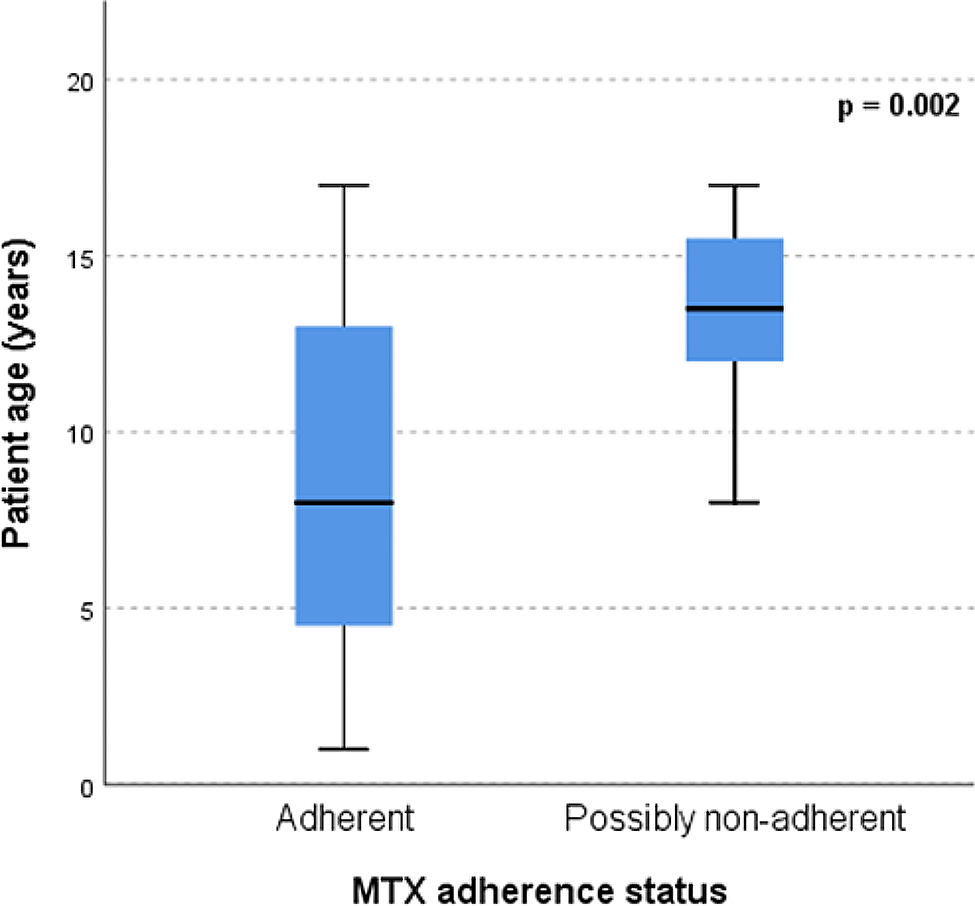
Adherence to weekly MTX therapy in our JIA population was 88% shortly after initiation of MTX therapy and 77% after one year, according to our ultrasensitive LC-MS/MS MTX assay. These findings are in line with adherence percentages described in medical literature [4, 5]. Teenagers were more at risk for non-adherence (p = 0.002, Fig. 1). A negative association between age and adherence was also earlier described [5].
There was no significant association detected between adherence according to the MTX assay and self-reported adherence in the JAMAR questionnaire, nor with the use of concomitant biologics. A potential explanation for this could be the small sample size. Only a relatively small part of children with materials in the Pharmachild biobank had plasma samples available after one year of MTX use. On the other hand, this could reflect a cohort that was relatively tolerable of MTX with less risk of non-adherence issues. MTX intolerance develops mostly within the first year of use and none of the patients in our cohort were tapering MTX or switched the route of administration (as coping mechanism of intolerance) [8, 13]. According to our protocols, JIA patient take MTX as long as it is effective as monotherapy in an as high as tolerable dose. When additional (biological) medication is started, MTX is ideally not tapered, because of its dose-dependent inhibiting effect on the forming of anti-drug antibody against biologicals.
A potential limitation of the use of MTX in plasma for adherence assessment is that it only reflects short term adherence. MTX has a relatively short half-life and there is a risk of ‘white coat compliance’ with a patient taking MTX shortly before a doctor’s appointment. In our study, however, patients were not aware of MTX adherence monitoring at the time of blood sampling. Moreover, quantification of 7-OH-MTX can provide additional information about the moment of medication intake and metabolism, regarding for instance the MTX: metabolite ratio. With our ultrasensitive MTX assay, we were able to detect the metabolite 7-OH-MTX during the entire dosing interval. This in contrast with other published assays [11, 12]. No discrepancies were seen in 7-OH-MTX formation in our study population.
A method in favour of long-term adherence monitoring is measurement of intracellular methotrexate polyglutamate (MTXPG). MTXPG concentrations have been demonstrated to be a potential surrogate biomarker of adherence to long-term therapy in children with JIA and juvenile dermatomyositis [14]. However, analysis of MTXPG in red blood cells is complicated and expensive and therefore, less suitable for routine clinical monitoring. Moreover, information on adherence can only be assessed regarding changes or fluctuations in MTXPG concentrations over time. This makes quantification of MTX concentrations in plasma the most feasible method for physicians to assess adherence to low-dose MTX, even with one-time sampling. Besides, lack of adherence to MTX is not unique for JIA patients. It is also a major issue in childhood acute lymphatic leukemia, now enabling us to monitor MTX adherence in this population as well [15].
A second caveat is that the MTX pharmacokinetics may differ between children and adults. Children seem to tolerate higher doses than adults, caused by a reverse age-dependant elimination of MTX [16, 17]. Dose-normalised concentrations for MTX are also lower in children than in adults [17]. Therefore, the applied adherence limits established in adult RA patients might be not fully applicable for the use in children. Regarding these limits, Bluett et al. suggested an adherence limit of 0.1 nM to be sufficient to detect adherence at 7 days for a weekly dose of ≥ 5 mg [11]. Nonetheless, Skoglund et al. also showed a 7-day MTX level of > 0,1 nM in 94% (16 out of 17) children with acute ALL on low-dose MTX maintenance therapy [12]. No patients had concentrations < 0.5 nM at 48 h after the last dose. Therefore, we considered the defined adherence limits of Bluett in adult RA patients suitable in children as well.
Noteworthy, a MTX concentration below the adherence limit may still be caused by alterations in a patient’s MTX pharmacokinetics, such as malabsorption or a faster metabolism. The bioavailability of MTX is highly variable (range 28–94%) and this may be influenced by food to some extent [18,19,20,21]. Therefore, non-adherence cannot be stated with certainty in patients with detectable MTX concentrations below the corresponding adherence limits. However, we believe that the influence of variability in absorption, due to food for instance, on the interpretation of the results in our study is minimal. The adherence limits (Table 1) are not dependent on (time to) peak concentrations (first limits are < 36 h and 48 h) and were defined to detect adherence in > 80% of compliant patients. Therefore, measurement of MTX concentrations in plasma is a suitable and objective method to further explore a case of existing suspicion of non-adherence. For instance, due to an unexplained, inadequate response to MTX despite stated adherence. Undetectable MTX plasma concentrations could give rise to the suspicion of non-adherence and could be a reason for the physician to address a patients’ adherence to therapy in order to improve it [9, 11, 15].
A last point of discussion is that the day of MTX administration was unknown in 60% of our patients, due to the retrospective nature of the data. In this case, we used the adherence limit of t = 168 h, which may have overestimated adherence. This was confirmed by the performed sub-analysis in the 40% of patients with a known day of administration. These results suggest that true adherence percentages ranged between 83% and 88% at baseline and were between 59% and 77% after one year of use. For optimal interpretation of MTX concentrations in clinical practice, it is important to know the dose and exact day of MTX administration.
To address most of the abovementioned limitations and caveats, a prospective study would provide a solution. However, this would give also rise to the risk of ‘white coat compliance’ with a patient taking MTX shortly before a doctor’s appointment or not even wanting to participate when it is known that plasma MTX concentrations will be checked in the study. A strength of our retrospective point of view was that patients were not aware of MTX adherence monitoring at the time of blood sampling.






留言 (0)