A now 14-year-old female of Caucasian descent was diagnosed with metastatic epithelioid mesothelioma at age 13 following initial presentation with deep vein thrombosis and constitutional symptoms. Abdominal ultrasound and MRI imaging showed pelvic peritoneal nodularity, and an initial PET scan showed low-grade increased FDG avidity in the area. Biopsy of the nodules was positive for epithelioid mesothelioma. Subsequent imaging raised concerns for chest deposits, and a biopsy confirmed thoracic involvement. Initial treatment of 6 cycles of cisplatin/pemetrexed showed a partial favorable therapeutic response with decreased metastatic burden but residual thoracic lymphadenopathy, and pleural and peritoneal disease. During her last dose of cisplatin, she developed a severe anaphylactic reaction. Given remaining PET avidity in both her abdomen and chest, additional systemic therapy was initiated with ‘6-weekly’ cycles of Nivolumab on day 1 and Ipilimumab on days 1 and 22 of each cycle.
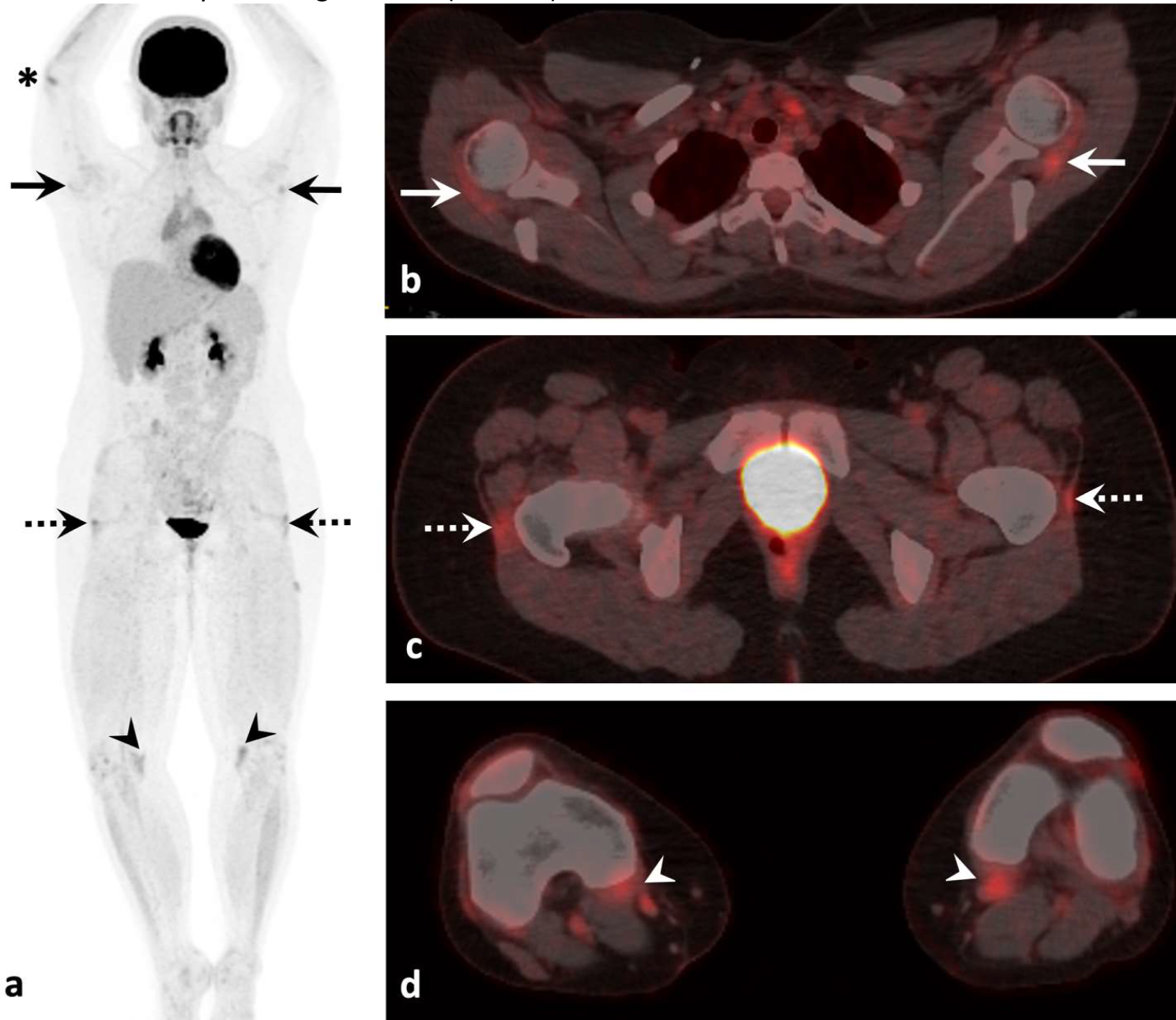
Following her second cycle of Nivolumab and Ipilimumab, she developed joint pain and stiffness, mainly located in her right elbow, bilateral shoulders, second metacarpal-phalangeal joints, proximal interphalangeal joints, knees, and hips. Her hip pain was associated with 15–20 min of morning stiffness without limitation of her range of motion. She had no functional impairment at the time and could continue with her regular activities. Following her 3rd cycle of Nivolumab and Ipilimumab, a repeat PET-CT scan showed a complete response of her mesothelioma. However, it also showed new symmetric increased metabolic activity at multiple entheses in the shoulders, hips, knees, and right elbow, most pronounced involving the supraspinatus, gluteus medius and minimus, and semimembranosus tendons (Fig. 1).
She was subsequently referred to our pediatric rheumatology clinic for assessment of potential irAE secondary to Nivolumab and Ipilimumab. Her initial examinations in the clinic showed bilateral shoulder joint line tenderness, positive FABERs test bilaterally, tenderness over bilateral greater trochanters, and effusions of her bilateral second PIPs of her hands. Her serological profile was notable for positive HLA-B27, positive anti-CCP, negative Rheumatoid Factor, and negative ANA. Her family history was negative for rheumatic conditions, aside from osteoarthritis in her mother. She had no prior joint symptoms to suggest a pre-existing rheumatic condition.
At her initial consultation, she was diagnosed with a grade 1 Rh-irAE with mild pain and clinical arthritis [4]. She was initially treated with Naproxen 10 mg/kg/dose twice daily with good improvement; however, with each subsequent cycle of ICI therapy, her inflammatory arthritis worsened despite escalating naproxen doses up to 12 mg/kg/dose twice daily.
Following her fifth cycle of ICI therapy, her symptoms worsened to a grade 2 Rh-irAE with worsening of her pain and new limitations of her daily activities. She was subsequently started on oral prednisolone 0.5 mg/kg/day, and her Naproxen was changed to Celecoxib due to GI intolerance. She had significant improvement in her pain and function after starting systemic steroids. Her steroids were tapered over a 3-month period without flaring of her inflammatory arthritis. At her last follow-up, she had achieved clinical remission of her mesothelioma following six cycles of Nivolumab and Ipilimumab and had control of her inflammatory arthritis on Celecoxib monotherapy.






留言 (0)