Participants
Participants were recruited from the London area through social media and Gumtree advertisements, school assemblies, posters, flyers, and word of mouth. Participants met criteria at telephone screening of (1) 1–7 days per week of cannabis use, averaged over the past-3-months, (2) either aged 16–17 or 26–29 years, (3) fluent in English, (4) ability to come to the research facility five times over the upcoming year, (5) normal or corrected-to-normal vision, and (6) capacity to give informed consent. Exclusion criteria included (1) history of diagnosed psychotic episode or disorder, (2) illicit drug use (excluding nitrous oxide) > 2 times per month, over the past-3-months, (3) nitrous oxide use > 1 day per week over the past-3-months, (4) receiving of treatment for any mental health condition (including CUD) in the past month, (5) currently daily use of a medication which is commonly psychotropic, (6) any mental or physical health condition deemed problematic by a medical doctor, and (7) age-adjusted body mass index (BMI) < 2nd or > 99.6th percentile. An additional exclusion criterion for the adult group was cannabis use at a frequency of once per week or more (averaged over a 3 month or longer period) before the age of 18.
Age ranges were chosen as the earliest time point at which adolescents do not require parental consent to take part in a research study in the UK (age 16), and for adults after the age at which adolescent brain development is generally complete (> 25 years, [26]). Inclusion criteria for cannabis frequency ensured that the participants were at least weekly users of cannabis. Finally, the criteria for no regular use of cannabis under age 18 in the adult group in CannTeen was chosen to isolate the effects of frequent cannabis use in adolescence (the adolescent group) on relevant outcomes, compared to a group that did not have this exposure (the adult group).
Procedures and measures
At the baseline visit, BMI was confirmed to be within the specified limits, and a valid form of ID was used to confirm participants’ current age. At all sessions, participants confirmed absence from alcohol and cannabis use for the previous 12 h, and other illicit drug use for 48 h via self-report, saliva drug screening, and breathalyser testing. Sessions took place at the Clinical Psychopharmacology Unit, UCL, central London. Testing sessions took place 3 months apart, with participants encouraged to attend as close to this schedule as possible but permitted to attend up to 2 weeks early and 6 weeks late if necessary. The CannTeen study ran from November 2017 to June 2021. Sessions after 23rd March 2020 had to be adapted to virtual data collection during the national COVID-19 lockdown periods in the UK. Virtual research sessions retained as many of the features of in-person data collection as possible. The assessments pertaining to this manuscript were not meaningfully altered by this change in data collection. However, we were unable to objectively determine the absence of recent alcohol, cannabis, or other drug use virtually and, therefore, these eligibility criteria were only fulfilled using self-report.
Analysis variablesOutcome
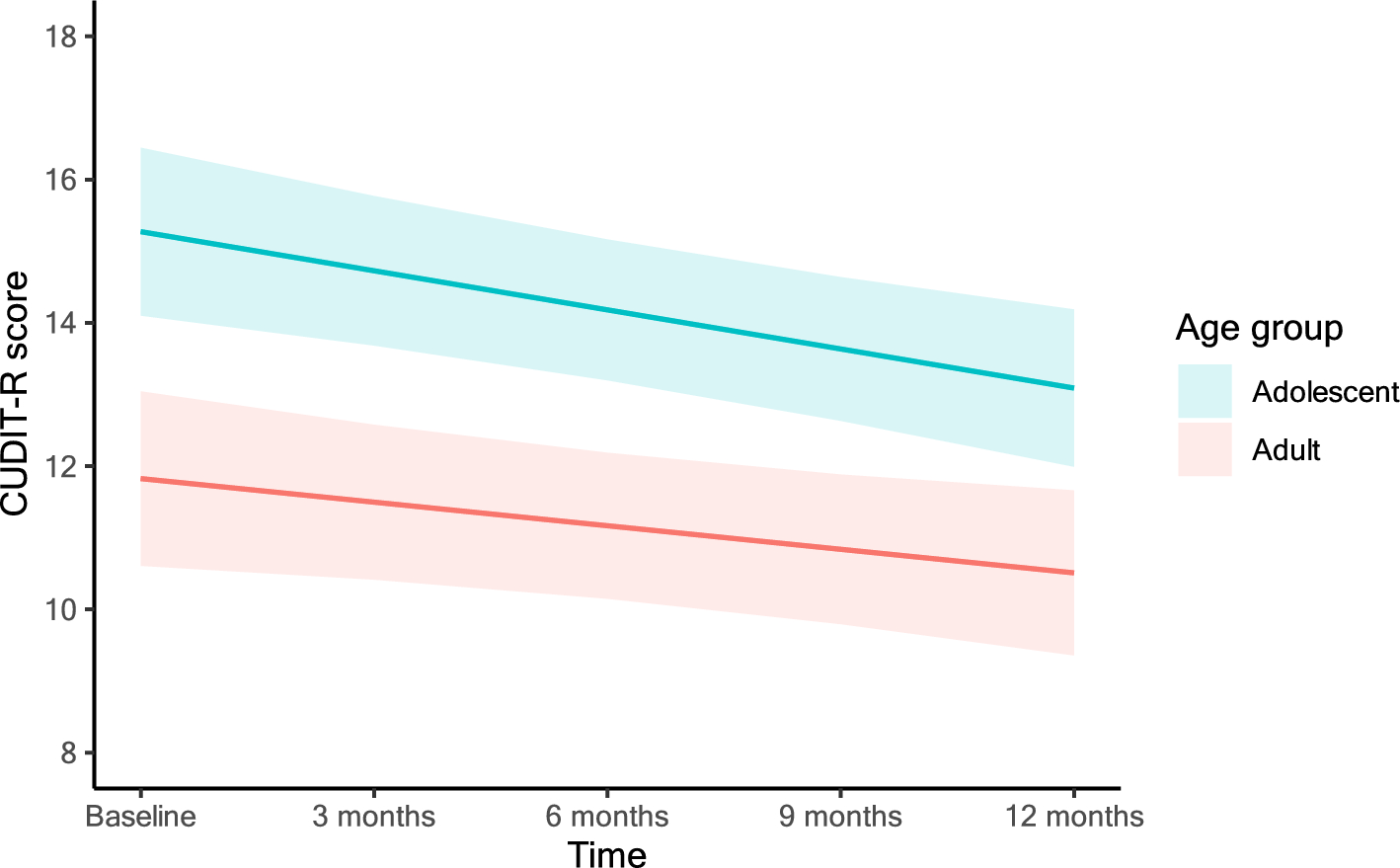
Participants completed the Cannabis Use Disorder Screening Test Revised (CUDIT-R; [27]) at each of the five testing sessions. This self-report measure assessed past-3-month symptoms related to cannabis use, including items related to frequency of use, duration of time spent ‘stoned’ on a typical day, difficulty stopping use, failing to meet obligations due to use, spending a lot of time on cannabis, problems with memory or concentration after using, using in situations that could be physically hazardous, and whether they had thought about stopping or reducing their use. The frequency that each of the 8 symptoms had occurred (never, less than monthly, weekly, daily, or almost daily) was recorded, and a numerical score was assigned to each. The CUDIT-R has good internal consistency and concurrent validity [28]. Total scores for the CUDIT-R range from 0 to 32.
Predictor
The predictor variable in this analysis was age group: adolescent (16–17 years) vs adult (26–29) years.
CovariatesMeasure of cannabis use—standard THC units
The EC-TLFB [21] was used to estimate mean weekly standard THC unit consumption at each time point. Participants provided details on all cannabis types used in the past 3 months (sinsemilla, hash/resin, seeded herbal, other), and all methods used (e.g., joint, bong, pipe, vaporiser, and ingested). They gave estimates of the number of grams of cannabis typically used with each method and indicated how much they would normally use of the method from a scale of 1–10. A 3-month TLFB was then completed with the participant at each session, noting every occasion of each method of cannabis use over the time period.
To approximate potency for the three main cannabis types reported in CannTeen we used estimates from UK seizure data. From the most recent available data [29], the estimates were 14.2% for sinsemilla ‘skunk’ type cannabis; 6.3% for hash/resin, and 3.5% for seeded-herbal cannabis. Some CannTeen participants reported the use of other cannabis types, including shatter/wax, THC oil and trichome powder (‘kief’). For these types, where appropriate, we again used estimates from Potter et al., 2018 (shatter/wax 78%, THC oil 51%, and trichome powder 40.15%). These were based on notably fewer samples than the main cannabis types, reflecting their less common use in the UK population. See Online Resource 1 for more details on how standard THC units were estimated in the presence of missing data.
COVID-19 time-period indicator
To adjust for the CannTeen study running during the COVID-19 pandemic and subsequent lockdown periods, a binary variable indicating whether each session occurred before 23rd March 2020 (the date of the first nationwide lockdown in the UK) as (0) or after (1) was entered into adjusted models as a covariate.
Gender
Participant gender was added as a covariate in adjusted models due to evidence indicating gender differences in the risk of CUD [30]. Participants were asked to report their gender at screening (“male”, “female”, “other”), participants only reported gender categories of “male” and female”.
Mental health
At each testing session, symptoms of anxiety and depression were assessed using the Beck Anxiety Inventory and Beck Depression Inventory, respectively. Total scores range from 0 to 63 on both measures. Exploratory analyses include these as time-varying covariates.
Other drug use
Detailed assessments of drug use were conducted using TLFB methodology. In line with other CannTeen investigations [7], exploratory analyses adjusted for daily cigarette smoking, alcohol use on two or more days per week, and other illicit drug use on 1 or more days per month.
Statistical analysis
Before analysing the data, we pre-registered the predictor, covariate, and outcome variables for this analysis on the Open Science Framework (https://osf.io/v2afh). The effect of age group (adolescent vs adult) on CUDIT-R score over time was analysed using linear mixed-effects models, using the “lme4” package in R. Multi-level modelling of longitudinal data allows for adjustment of within-person variation due to repeated measurements from the same individual not being independent. These models also allow for the exploration of the effect of predictors on the outcome, accounting for the clustering of data across the repeated measurements. The outcome variable in all models was the CUDIT-R score, and all models included a random intercept of participant. Fixed effects included age group, time, and age*time interaction. The interaction term was included based on the assumption that cannabis use would continue over the year period and to assess whether this would involve a worsening of CUD symptoms in the adolescents compared to the adults. A quadratic fixed effect of time was assessed and did not improve model fit, so was not retained in subsequent models. Age group was a binary variable, coded using Helmert coding, thus the regression coefficient can be interpreted as the mean difference in CUDIT-R scores between adult and adolescent groups. Adjusted versions of the model included a time-invariant fixed effect of gender (0 = male, 1 = female), and time-varying fixed effects of the COVID-19 pandemic indicator and weekly standard THC units. Additional exploratory sensitivity analysis included all previous covariates as well as adding mental health, tobacco, alcohol, and other drug use as time-varying covariates. Model fit was compared using the Akaike information criterion (AIC), Bayesian information criterion (BIC), and −2 log likelihood (-2LL).
Mean weekly standard THC unit data were winsorized at 95% and 5% quantiles, using the R package “Winzorise”, to minimise bias from outlying or implausible estimates. This method involves replacing values that lie above or below the 95% and 5% percentiles (respectively) with the values at these percentile limits. Sensitivity analyses indicated that model estimates were very similar when using standard THC unit data with and without winsorizing (see Online Resource, Table 6). A power calculation was conducted to detect cross-sectional differences in CUD by age group (reported in [7]), based on previous studies indicating an odds ratio of 3 [9,10,11]. This indicated 148 participants were required, split evenly by age group.
As mixed effects models use maximum likelihood estimation, all participants were included in the analysis, despite participants contributing a different amount of data due to dropout or missing sessions (see Online Resource, Table 2). Therefore, there was no need to use multiple imputation or other accounting for missing data in this analysis. However, there was some very minimal (n = 3) missing data in the exploratory sensitivity analysis. Participants with complete CUDIT-R data did not differ from those missing any CUDIT-R data on gender (p = 0.722), CUDIT-R baseline total scores (p = 0.346), depression (p = 0.142), anxiety (p = 0.751), daily smoking (p = 0.540), > 2 weekly alcohol use (p = 0.263), or > 1 per month other drug use at baseline (p = 0.600). Age groups did not differ on mean number of sessions with available CUDIT-R data (adolescents: 4.20, adults: 4.00, p = 0.384). See Online Resource, Tables 2 and 3 for further details. We therefore did not have concerns about bias related to missing data influencing our model outcomes (Online Resource, Tables 1, 2).
Table 1 Baseline sample characteristics. Data shown are frequencies and means (standard deviations) as appropriateTable 2 Mean standard THC units at each time point, by age group 




留言 (0)