
記住我




Mean age of the participants was 36.9 years (SD = 10.8, Range 24.0–74.0). 87.0% of the sample reported to be female (n = 395) while 13.0% reported being male (n = 59). No one reported his gender to be diverse. Regarding the highest degree of education, 0.2% (n = 1) completed a lower secondary degree, 2.8% (n = 13) completed a higher education entrance qualification, 87.9% (n = 399) completed a university degree, 8.4% (n = 38) completed a PhD and 0.7% (n = 3) completed a postdoctoral lecture qualification. Mean number of professional years was 8.9 (SD = 8.6, Range 1.0 – 44.0). The mean number of working hours per week was 30.8 (SD = 9.3, Range 2.0 – 60.0). Of the participants, 59.7% (n = 271) reported working mainly in out-patient settings, while 40.3% (n = 183) reported to work mainly in inpatient settings. A total of 55.3% (n = 248) of the participants reported being employed, while 44.7% (n = 201) reported being mainly self-employed. Of the participants, 68.9% (n = 313) of the participants reported affective disorders (ICD-10: F3) as the most common diagnoses of their patients, followed by neurotic disorders (ICD-10: F4; 14.8%, N = 67), personality disorders (6.2%, n = 28), psychosis (ICD-10: F2; 4.4%, N = 20), substance related disorders (ICD-10: F1; 3.5%, n = 16), and disorders from ICD-10 section F5 (2%, n = 5).
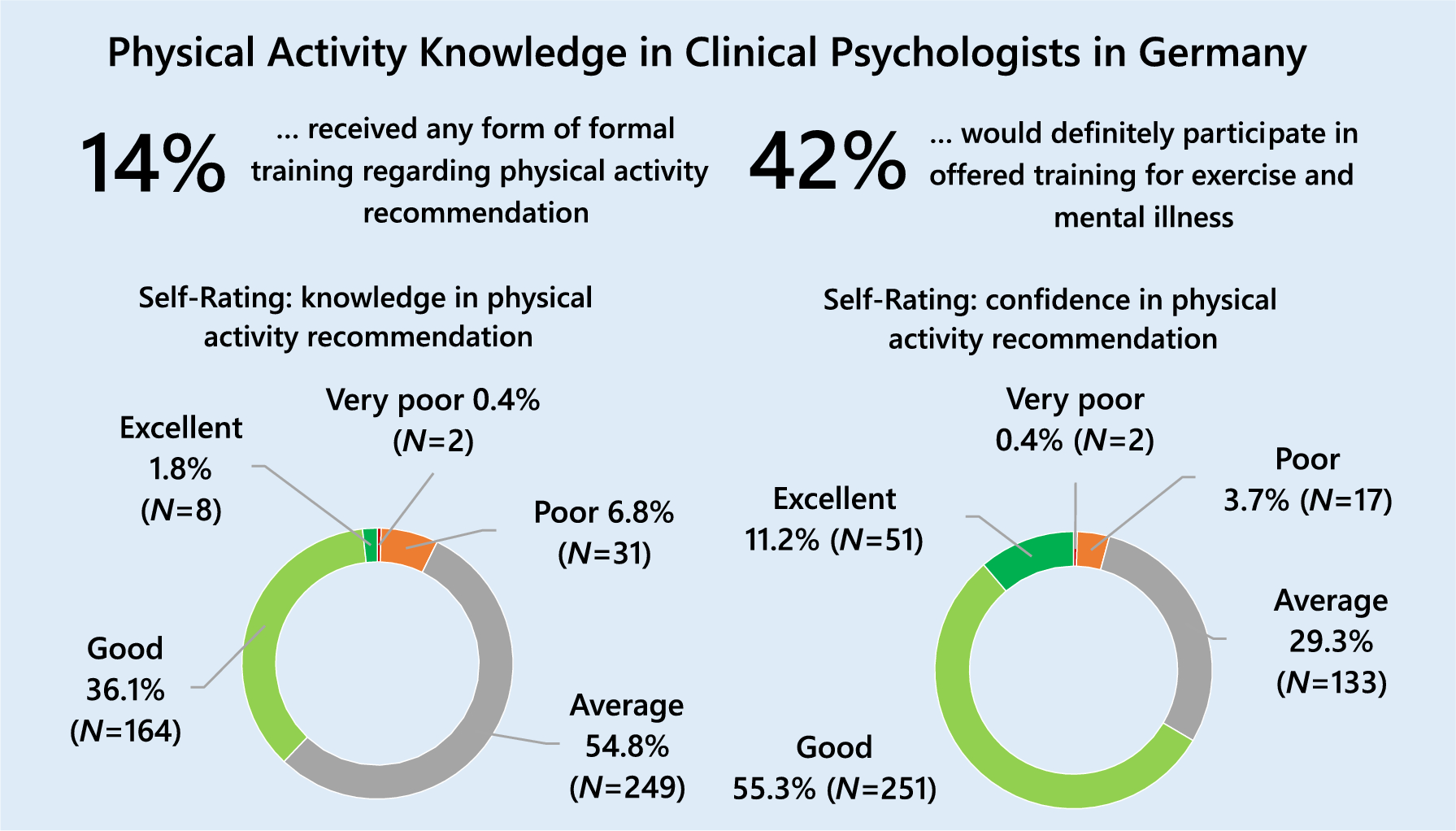
Physical activity knowledgeThe results indicate that 14.1% (n = 64) of the participants reported to have received any kind of formal training in physical activity recommendation, while 85.9% (n = 390) did not. Most participants rated their knowledge in physical activity recommendation to patients with mental illness as average (54.8%) or good (36.1%; see Fig. 1). Most of the participants rated their self-confidence in PA recommendations as good (55.3%, n = 251) or average (29.3%, n = 133; see Fig. 1). A large percentage of all participants knew that physical activity can lower blood pressure (90.6%, n = 411) and prevent chronic diseases (96.7%, n = 439) and depression (85.0%, n = 386), while only 60.6% (n = 275) knew that physical activity is beneficial even when performed in bouts of less than 30 min, and only 38.7% (n = 176) knew that physical activity is preventive against some forms of cancer (see Supplement Table S1).
Fig. 1
Education and self-rated knowledge, and self-confidence regarding physical activity recommendation (N = 454)
Participants who received formal training in physical activity recommendation showed significantly higher self-ratings of knowledge (U = 6586.00, Z = -6.83, p < 0.001) and self-confidence (U = 8320.00, Z = -4.77, p < 0.001) regarding the recommendation of physical activity. Knowledge of the benefits of physical activity showed a small positive correlation with age (r = 0.1, p = 0.03), self-rated knowledge (rs = 0.19, p < 0.001), and self-rated confidence (rs = 0.25, p < 0.001).
Beliefs regarding physical activity and mental healthOn average, participants rated the treatment options of pharmacotherapy, social support family therapy, social skills training, and psychotherapy as more effective than physical activity. Contrary to that, electroconvulsive therapy, and bright light therapy were evaluated as less effective than physical activity (see Fig. 2). 17.6% (N = 80) of the participants reported undertaking a formal assessment of the patient’s suitability for exercise prior to prescribing a program, while 82.4% (n = 374) did not.
Fig. 2
Rating of effectiveness of different treatment strategies compared to physical activity (N = 454). Horizontal Axis: Rating on Likert Scale of Item 11 of the EMIQ-G: "Rate how valuable you believe each treatment strategy is compared to exercise"; Rombus indicates arithmetic mean, error bars represent standard deviations
Supplementary table S2 shows the distribution of answers on beliefs regarding physical activity and mental health. The majority of participants (56.6%) believed that their patients do know that physical activity is good for their physical health, while most participants (60.1%) believed that their patients do not know that it is good for their mental health (see supplementary table S2). Of the participants, 58.5% believed that lack of self-efficacy in performing physical activity is a problem for their patients, and 93.4% believed that physical activity is as valuable for inpatients as it is for outpatients (see Supplementary Table S2). Only 2.9% of the participants believed that the benefits of physical activity are not long lasting, and 20.1% believed that patients would not adhere to physical activity recommendations (see Supplementary Table S2).
Physical activity recommendation behaviorMore than 80% of the participants reported to recommend physical activity to patients with mental illness most of the time (43.4%) or always (38.8%; see Fig. 3). Regarding the methods used for physical activity recommendation, personal discussion was the most commonly used (97.4%), followed by referral to exercise professionals (46.5%), and referral to community based programs (35.7%) while only 17.4% used brochures of pamphlets (see Fig. 3). Regarding the type of activity recommended, aerobic activity (90.5%) and relaxation activities (84.8%) were the most commonly recommended activities, while weight or resistance training (31.2%) and combat sports (29.5%) were less likely to be recommended (see Fig. 3). Concerning the recommended intensity, most participants recommended moderate-intensity activities (30.6%, n = 139) or 4) or a level that makes them feel good (27.1%, n = 123). Only 4.0% of the participants (n = 18) recommended low-intensity and 0.4% (N = 2) vigorous-intensity activities. A total of 32.2% (n = 146) reported that they did not recommend any intensity. Regarding the recommended frequency, 33.7 (n = 153) recommended to be active most days of the week, 27.5% (n = 125) 3) once to twice a week, 15.0% (n = 68) 4) as often as they feel they can, 12.3% (n = 56) every day, and 11.5% (n = 52) recommended other frequencies. Regarding duration of single exercise sessions, 38.1% (n = 173) recommended 30 min, 14.5% (n = 66) as long as they can, 12.3% (n = 56) 20 min, 7.0% (n = 32) 10 min, 0.9% (n = 4) 60 min, and 27.1% (n = 123) reported to recommend other durations.
Fig. 3
Physical Activity Recommendation Behavior (N = 454)
Physical activity recommendation behavior was positively associated with knowledge of its benefits (Kruskal Wallis Test: χ2 = 9.92, p = 0.02, average r between the groups from post-hoc tests = 0.13), self-rated knowledge regarding physical activity recommendation (χ2 = 36.43, p < 0.001; average r = 0.22), and self-rated confidence in physical activity recommendation (χ2 = 52.91, p < 0.001, average r = 0.26) and negatively associated with rating of barriers regarding recommendation (χ2 = 72.85 p < 0.001, average r = 0.29) as well as barriers for physical activity participation in patients (χ2 = 20.61,, p < 0.001, average r = 0.12). Supplementary Table S4a–e show post-hoc tests using Bonferroni correction. No significant association were found with minutes of moderate to vigorous physical activity per week performed by the psychologists (χ2 = 5.98, p = 0.11) and age (χ2 = 2.56, p = 0.47).
Barriers to physical activity recommendation and participationConcerning barriers to physical activity recommendation, participants’ consent to different barriers was generally low for most of the barriers, and less than 10% of the participants agreed or strongly agreed (see Supplementary Table S3). The barriers that yielded the most approval were the statements that patients with mental disorders would not adhere to an exercise program (11.0% agreed or strongly agreed), that the mental health of patients would make it difficult for them to participate in exercise (8.1% agreed or strongly agreed), and a lack of knowledge on how to recommend physical activity to patients with mental disorders (8.9% agreed or strongly agreed). Regarding important barriers to exercise participation in their patients, the sample rated the stigma attached to mental disorders (37.6% agreed or strongly agreed), lack of confidence (35.7% agreed or strongly agreed), lack of knowledge (34.3% agreed or strongly agreed), and lack of training partners (28.4% agreed or strongly agreed) as important barriers (see Supplementary Table S4). Barriers to physical activity recommendation score was positively associated with barriers to physical activity participation score (rs = 0.40, p < 0.001) and showed a negative association with knowledge of the benefits of physical activity (rs = -0.13, p < 0.01), self-rated knowledge (rs = -0.17, p < 0.001), and self-confidence (rs = – 0.13, p < 0.01) regarding physical activity recommendation. The score on barriers regarding exercise participation in patients was negatively associated with the knowledge score (rs = – 0.23, p < 0.001), professional years (rs = – 0.13, p < 0.01), self-rated knowledge (rs = – 0.26, p < 0.001), and self-confidence (rs = – 0.37, p < 0.001) regarding the recommendation of physical activity. Participants who had received formal training on physical activity recommendation showed lower barrier to exercise participation scores (rs = – 0.10, p = 0.03).
Personal physical activity behaviorOn average, participants reported a median of 240 min of moderate-to-vigorous physical activity (MVPA) per week (M = 329.2, SD = 343.6, range 0– 2940.0), with a median of 120 min of moderate activity (M = 179.8, SD = 253.1, range 0–2520.0) and a median of 120 min of vigorous activity (M = 149.3, SD = 173.6, range 0–1680.0) per week.
A total of 67.2% (n = 305) met the WHO recommendation of at least 150 min of moderate activity, 75 min of vigorous activity or a combination of both, while 32.6% (n = 148) did not. Average reported median of sitting minutes per weekday was 480.0 (M = 481.9, SD = 174.7, N = 454, range 0–1380) and 180 min walking per week (M = 315.3, SD = 467.4, N = 454, range 0–6300). Participants who reported higher levels of MVPA per week were more likely to have received formal training regarding physical activity recommendation (rs = 0.12, p = 0.01), and showed higher self-rated knowledge (rs = 0.12, p = 0.01) and self-confidence (rs = 0.16, p < 0.01).
Desire for further trainingMost participants reported to possibly participate in further training for prescribing exercise for mental illness if offered to them (44.1%, n = 200), while 41.6% (n = 189) reported they would definitely participate. 10.6% (n = 48) stated that they would possibly not participate, and 3.7% (n = 17) did definitely not want to participate. Regarding preferred training methods, most participants were interested in face-to-face lectures or seminars (78.0%; N = 354), followed by online courses, in which 33.3% (n = 151) were interested. 18.3% (n = 83) were interested in a webinar and 10.8% (n = 49) in CD / DVD self-paced learning. Concerning the preferred topic of training, most participants were interested in training on “How to get and maintain motivation in people with mental illness” (61.0%, N = 277) followed by “What type of exercise is best?” (45.4%, n = 206), “How to assess the patients suitability for exercise” (37.0%, n = 168) and “Linking patients with community exercise programs” (28.0%, n = 127). Of the participants, 42.7% (n = 194) were interested in all these topics. Participants who reported higher amounts of MVPA per week were more likely to be interested in further training on physical activity recommendation (rs = 0.15, p < 0.01, n = 453), while participants of a higher age (rs = – 0.21, p < 0.001) or more professional years (rs = – 0.25, p < 0.001) showed less interest in further training.
Exploratory AnalysesSupplementary Table S5 shows comparisons of the most relevant variables in subgroups regarding years of professional experience, treatment setting, and level of training of the participants. Supplementary Figure S1 shows comparisons of the ratings of the efficacy of different treatment methods for the different subgroups. The results show no major differences between the ratings. Supplementary Figure S2 shows comparisons of the subgroups regarding formal training, self-rated knowledge and confidence, frequency of recommendation, and type of recommended activities. Overall, the comparisons show no large differences between the subgroups. The results indicate that participants with more years of professional experience, participants working mainly in outpatient settings and participants who already completed psychotherapy training have slightly higher rates of formal training, self-rated knowledge, and confidence but differences were rather small. Regarding recommendation frequency, individuals working in outpatient settings recommended physical activity somewhat less than individuals working in inpatient settings (recommendation most of the time/always 71.2% vs. 83.6%). Compared with psychologists with more professional experience, psychologists with less years of professional experience recommended more often weight or resistance training (37.6% vs. 26.9%) and combat sports (34.6% vs. 25.9%). Weight and resistance training was more often recommended by participants working in inpatient settings (36.1% vs. 29.5%), while participants working in outpatient settings recommended combat sports more often (23.5% vs. 33.6%).
留言 (0)