Delay in diagnosis but no stage migration in 2020
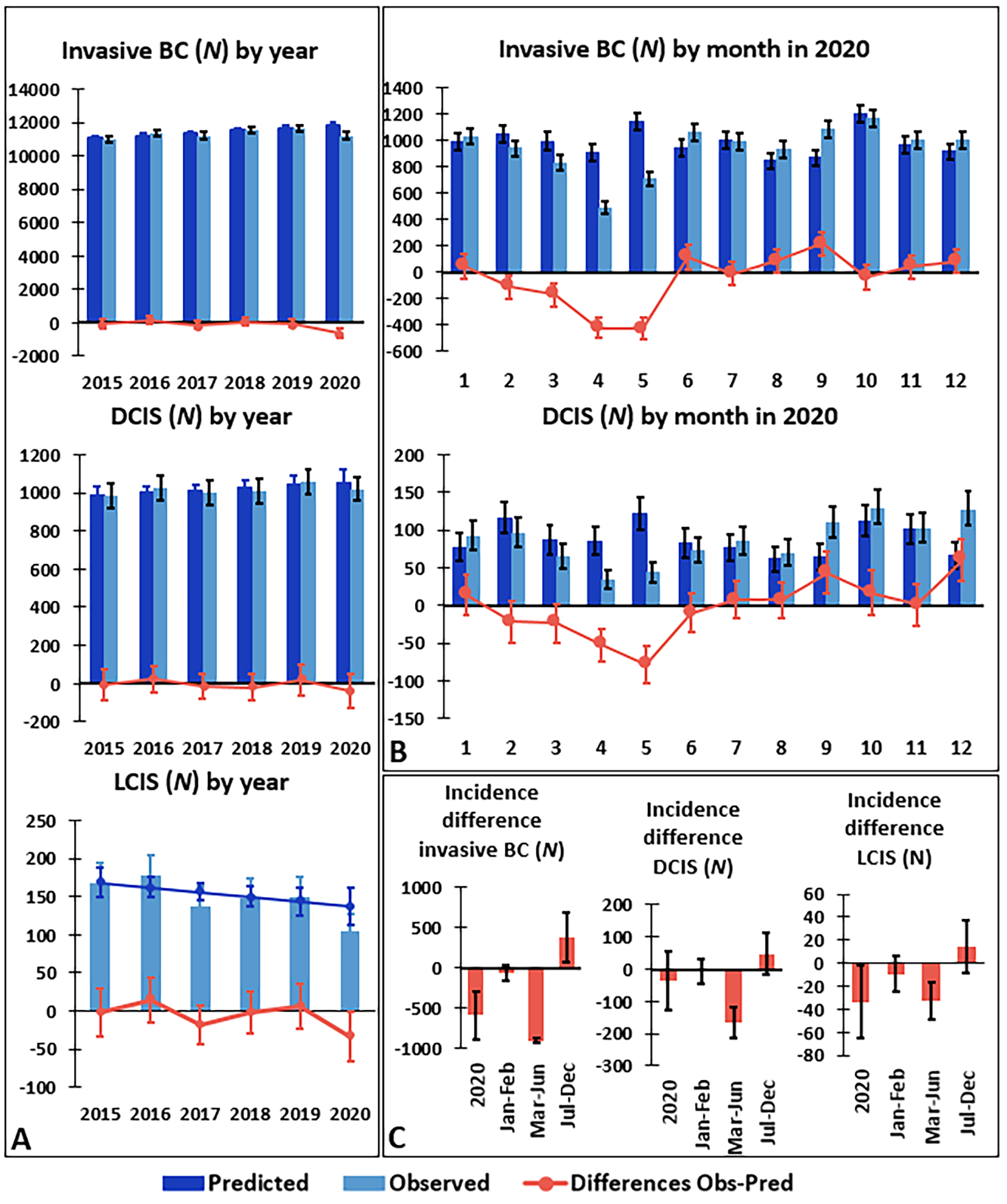
The BC incidence decline during the first wave of the COVID-19 pandemic in Belgium (March-June 2020) was primarily seen in cStage 0 and I, and in patients aged 50 and over. This finding can be explained by the temporary suspension of organized screening programs and non-essential healthcare, and is consistent with results from other countries showing reductions in screening volume and number of diagnosed BC [27,28,29,30,31]. In March-June 2020, we observed a higher proportion of tumors diagnosed with cStage II, however, the absolute number of cStage II tumors observed in 2020 was lower than the expected values. This finding indicates that – despite general healthcare restrictions - cStage II tumors were more likely to be diagnosed than lower stage tumors in 2020. Furthermore, for patients aged 70+, who are not invited for organized screening in Belgium, the decline in diagnosis impacted all tumor stages equally.
During the rebound period July-December 2020, even when considering annual increasing trends in incidence, higher than predicted absolute incidence numbers were observed indicating that missed diagnoses were partially recovered in the latter half of 2020. A similar rebound in missed diagnoses was not observed in population-based studies from The Netherlands or Scotland suggesting that Belgium was particularly successful in prioritizing oncologic care and restarting BC screening programs [30, 32]. Since both mentioned studies compared 2020 data to average values in previous years without accounting for increasing trends in BC incidence, the results in these reports should be interpreted with care.
There was no evidence for a general shift to a more advanced cStage of tumors diagnosed in July-December 2020. Contrarily, more cStage 0 tumors than predicted were diagnosed in this period, particularly in the screening age group, suggesting that much of the diagnostic recovery was due to effective resumption of the screening programs in Belgium [2]. However, 6% of female BC incidence was still outstanding at the end of 2020, which underlines the need to continue the monitoring of BC incidence and stage distributions in the subsequent years.
Adaptations in care
The COVID-19 pandemic forced healthcare systems worldwide to implement priority-setting mechanisms in the management of cancer [33, 34]. For BC, the European Society for Medical Oncology (ESMO), among others, published specific recommendations including offering selected patients with luminal-like BC NAHT to avoid harm due to surgical delay [9,10,11,12,13, 35]. In Belgium, the overall proportion of patients receiving surgery (with/without NAT) did not change in 2020. In line with reports from numerous other countries and centers, our results showed a small shift from primary surgery to NAHT for patients diagnosed with early-stage BC [14, 29, 36,37,38]. Also, our findings showed no change in average pathological tumor diameter or nodal involvement between 2019 and 2020, both in the primary surgery population and in the NAT population separately. We therefore have the impression that patients were appropriately selected for this adapted approach. It is reassuring that on average the patients receiving primary surgery suffered no increased time to treatment, and the patients receiving NAT had a shorter time from incidence to start of NAT and to surgery, compared with previous years. In other countries, for example in The Netherlands, treatment delays were documented in the early weeks of the pandemic [29].
The recommendation to offer hypofractionated adjuvant radiotherapy to selected patients with BC to reduce hospital visits was documented for 8% of the patients in Belgium in 2020 [12, 13, 39].
Still missing or postponed diagnoses
At the end of 2020 an estimated 660 BC (in situ/invasive) were still undiagnosed in Belgium [8]. These diagnoses were largely expected in the 70 + age group, a population not reached through organized screening programs in Belgium, and are predicted to mainly be cStage I tumors, which are less likely to progress rapidly [40]. Nevertheless, continuation of monitoring of the missed diagnoses and possible influence on stage at presentation during the next years is mandatory.
Strengths and limitations of this study
Our study, unlike most studies that evaluated the impact of COVID-19 on BC incidence and stage in 2020, computes predicted values for 2020 based on the trends in incidence and stage over the previous 5 years to allow a reliable assessment of the impact of the pandemic [30, 32, 41,42,43,44,45,46]. In our opinion, the integration of these trends in the assessment of incidence, stage, and treatment of cancer during the pandemic in 2020 is of utmost relevance, knowing that cancer incidence is continuously evolving because of differences in age distribution, lifestyle, environmental factors, socioeconomic status, healthcare quality, screening programs etc [47].
Furthermore, our study used data from a highly complete population-based cancer registry combined with data from the national healthcare organizations covering all Belgian residents. The findings refer to the total BC population in Belgium and avoid possible bias introduced by changes in hospital choice or physician referral patterns in reaction to the COVID-19 pandemic.
Besides a thorough evaluation of possible changes in cStage of BC in 2020, our study also investigated the exact pathological tumor dimensions and nodal involvement through manual review of pathology records. Therefore, the clinical findings (cStage) were supplemented with pathological results.
Our study lacked valuable information such as the molecular subtype of BC, that plays an essential role in the priority-setting for management (e.g. patient selection for NAHT to safely postpone breast surgery), and the deprivation status of the patient, for which it was shown that the COVID-19 burden was higher in more deprived areas in Belgium [9,10,11,12,13, 35, 48]. Our study didn’t assess screening participation in detail, which other studies did document on and reported different associations between deprivation status, BC incidence and stage, and screening participation [30, 49,50,51,52]. Finally, regarding the completeness of the reimbursement data, details of adjuvant treatment and breast reconstruction were incompletely available for our study and remain to be assessed as more reimbursement data become available.



留言 (0)