
記住我
To inform the development of the practice model, an explanatory, sequential, mixed-method research study was adopted. The research was conducted in Worcester, Breede Valley sub-district in the Western Cape Province, South Africa. The setting was selected based on designated workplaces being present in Worcester area that represent linkages with various levels, namely local, regional as well as national (retail stores and large commercial food companies).
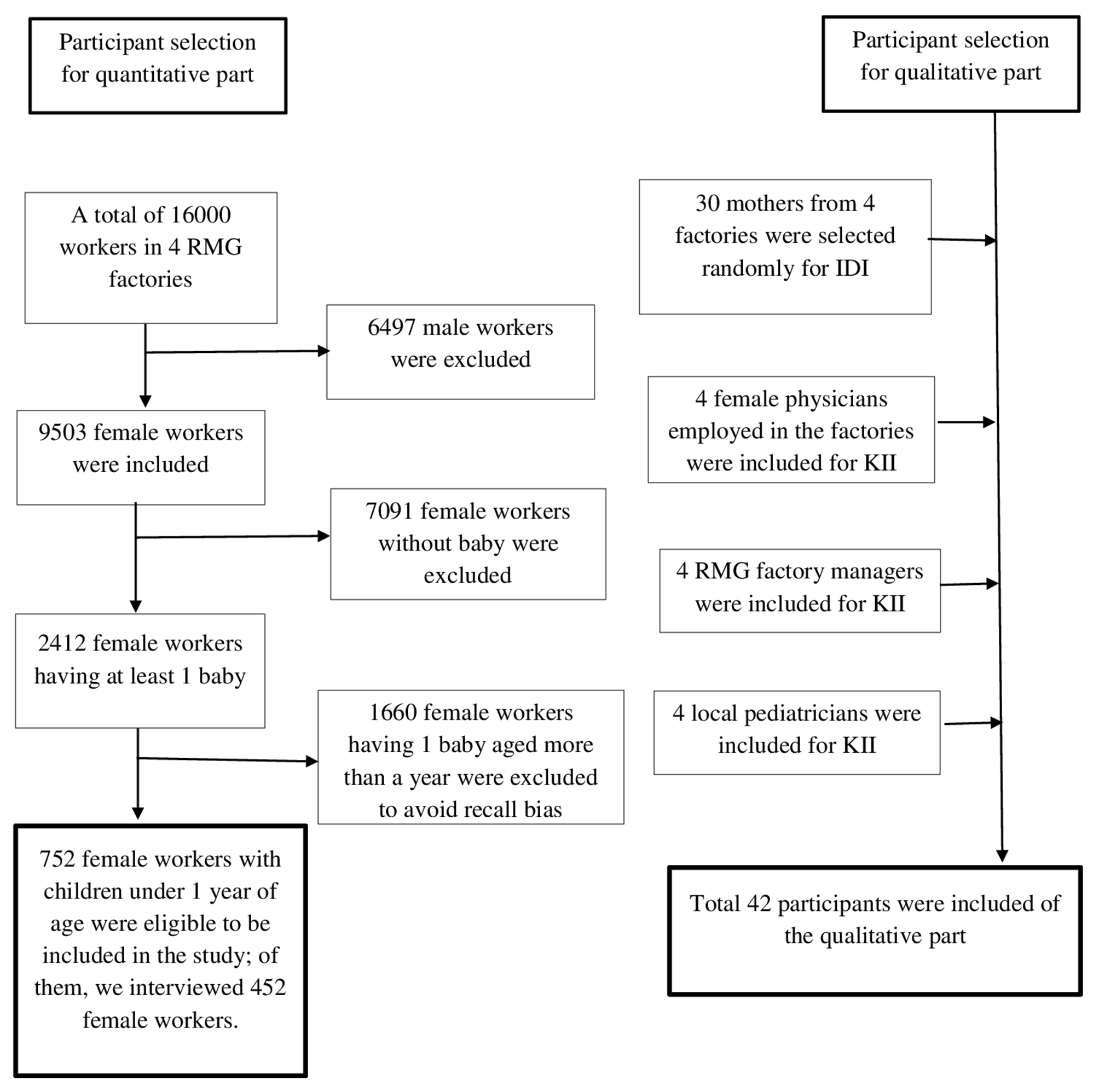
The research was conducted in three distinct phases (Fig. 1). Phase one employed a quantitative, descriptive cross-sectional study design, using an online survey to assess current breastfeeding support practices and has previously been reported [13]. Phase 2 was a qualitative, multiple case study. Data was collected at nine purposively selected workplaces from the manufacturer, retail and public sector, using focus group discussions (FGDs) with employees and in-depth interviews with managers. FGDs were also conducted with employed breastfeeding mothers from designated workplaces who exclusively or predominantly breastfed their children for any period up to six months. This paper will elaborate only on phase three of the study, the model development and face validation phase. The research received ethical approval (S17/04//089) from the Stellenbosch University Health Research Ethics Committee.
Fig. 1
Phases of the research study
Review of the evidence regarding workplace breastfeeding interventions and breastfeeding outcomesA critical review of the literature in the field of workplace breastfeeding support interventions and breastfeeding outcomes were conducted. A search was conducted on PubMed using the following key words: (breastfeeding OR breast feeding OR lactation) AND (work OR workplace OR employment) AND (intervention OR support) AND (duration OR continuation OR exclusive OR rates). The literature consulted included published articles from 2008 through 2019 listed in PubMed. The PubMed search article titles was assessed. Sixteen selected article abstracts, and full text were further screened of which seven were excluded (two was qualitative studies, three was systematic reviews and two were excluded as the main outcomes measured were not breastfeeding duration, continuation and exclusivity). This yielded a total of nine articles included. Amongst the material a review article [14] on worksite lactation accommodation was found. The review article was reviewed, and five similar articles as yielded by the selected PubMed search article was found. From the critical review of the literature, it was concluded that workplace breastfeeding interventions and support services are responsive to breastfeeding outcomes and practices in terms of increased rates of breastfeeding duration, continuation and exclusivity [7, 14,15,16,17,18,19,20]. There is a lack of randomised control trials relating to breastfeeding support in the workplace as most studies extracted reflected cross-sectional surveys. Not all studies consistently found significant associations with all breastfeeding interventions and breastfeeding outcomes assessed. This can be attributed to possible confounding variables that may have been present e.g. lack of family support, cultural and maternal belief of the mother, the mother`s low self – efficacy for breastfeeding.
Identifying main elements from phase one and two for inclusion in the practice modelPhase one and phase two were analysed, interpreted and the main issues arising were identified for inclusion in the model. Phase one analysis involved statistical analysis of the quantitative data. Phase one findings revealed that provision of a private space for breastmilk expression was uncommon [13]. Allowing time for breastfeeding and promoting breastfeeding amongst the employees were also not commonly practiced [13]. The provision of breastfeeding time in South Africa is recommended according to the Basic Conditions of Employment Act, Code of Good Practice on the Protection of Employees during Pregnancy and After the Birth of a Child Sect. 5.13 [21]. Needs identified by managers related to physical space, a regulatory framework, communication, education and information. From phase one of the study, the following pertinent issues raised were taken up in the practice model: provision of breastfeeding time and private space, education and communication.
Phase two analysis of the FGDs with employees and in-depth interviews with the managers involved content analysis using the Atlas ti programme. Phase two findings revealed the absence of private space and time for expressing breastmilk as major challenges for women returning to work. The lack of communication between employers and employees regarding their needs, policies regulating their return from maternity leave, as well as unsupportive attitudes on the part of staff and co-workers were highlighted. The employed mothers who successfully combined breastfeeding and work had a strong belief in the benefits of breastfeeding and this motivated them to continue breastfeeding with work. Therefore, the provision and promotion of breastfeeding time and space as well as communication (conducting a return-to-work consultation after maternity leave) were included in the practice model. Also included in the model were addressing unsupportive attitudes and increasing belief in breastfeeding among employees by enhancing knowledge of the benefits of breastfeeding and the recommended breastfeeding time through education. Conducting a needs assessment amongst women to assist managers with planning and coordination was also taken up in the practice model.
Integrated programme theory and program logic models to draft the practice modelA programme theory describes how and why a programme is supposed to work [22]. The process of developing a programme theory promotes evidence-based thinking and provides a clear understanding of how change will occur. It also describes the beliefs and assumptions that underlie the choice of activities, thereby making the results more credible [22]. By reviewing the literature, the underlying linkages and secure evidence of the mechanism of change that would lead to improved breastfeeding duration and EBF rates amongst employees could be explained. The process involved moving continually between theory and practice to develop the practice model programme theory. A logic model is a commonly used tool for illustrating an underlying programme theory. The logic model was selected for the mentioned reason and also as the logic model would provide stakeholders with an easy-to-follow clear visual representation and clear specific guidance in terms of what needs to be provided (input and responsibilities) and the potential gains it holds. The following components are included in a programme logic model 1) Inputs: any resource or material used by the programme to enable its activities e.g. private hygienic space with resources 2) Activities: any services or treatments provided by the programme e.g. engage in interpersonal communication a return to work consultation 3) Outputs: amount of activity provided, described in quantifiable terms e.g. number of employees aware of breastfeeding space 4) Outcomes: any characteristics of the participants that, according to the programme theory, are expected to change as a result of the participants’ receiving services e.g. improved staff wellness and better work life integration practice 5) Impact: the ultimate intended change e.g. cost saving in terms of retaining staff [23,24,25].
Delphi roundsA list of experts in the fields of infant feeding, breastfeeding, human resources management (private and public sectors), academia, child health and behavioural and organizational development was developed. The experts met the requirements of having knowledge and experience of breastfeeding, infant feeding, or human resource management in an organization. An email was sent to the experts to invite them to take part in the study as an expert panel member. Sixteen experts were invited and 11 (69%) participated in the two modified Delphi rounds. The Delphi process and rounds allowed the researcher to gather the opinions of a panel of experts without having to bring them together physically, thereby saving time, cost and effort. The process is free from social pressure and individual dominance and conducive to independent thinking and the gradual formulation of judgement. Of the 11 expert members, ten were female and one male. Four of the expert members were from the academic/research sector and three were International Board-Certified Lactation Consultants. The remaining expert members comprised a provincial health department official, a UNICEF nutrition specialist, one human resource practitioner from the private sector and one from a provincial organizational development department, industrial psychologist.
A graphic designer assisted with the drafting and refining of the practice model. The first version of the practice model was supported by an additional one-page information sheet providing guidance as to the inputs and activities that the employer must provide and perform. The Delphi round one questionnaire consisted of open-ended questions relating to the elements in the developed practice model: inputs, activities, outputs, outcomes, linkages/connections between inputs, activities, outputs and outcomes, strengths, weaknesses, achievability/realistic to implement, challenges, design, use of wording and any recommendations and improvements. Content analysis techniques was used to the open-ended input by grouping similar items together and summarizing the comments received. These were discussed by the research team. Thereafter the practice model was amended. Under the inputs, the identification of a breastfeeding champion, including trade unions, lactation consultants and breastfeeding counsellors as well as other international toolkits was added. Two activities were added to the model: one was maternity leave provision, as this was believed to contribute to the achievement of the stated long-term outcome of increased breastfeeding duration. The provision of antenatal education by the employer was removed and changed to the inclusion of time for pregnant employees to participate in antenatal visits/classes/clinics, which was added under the education heading. Granting pregnant women time off to participate in antenatal preparation is included in Sect. 5.12 of the Code of Good Practice on the protection of employees during pregnancy and after the birth of a child [21]. Listed activities linked to legislation was highlighted with the text “legal obligation /recommendation to provide”. Also, additional long-term outcomes were added, and more images included under impact.
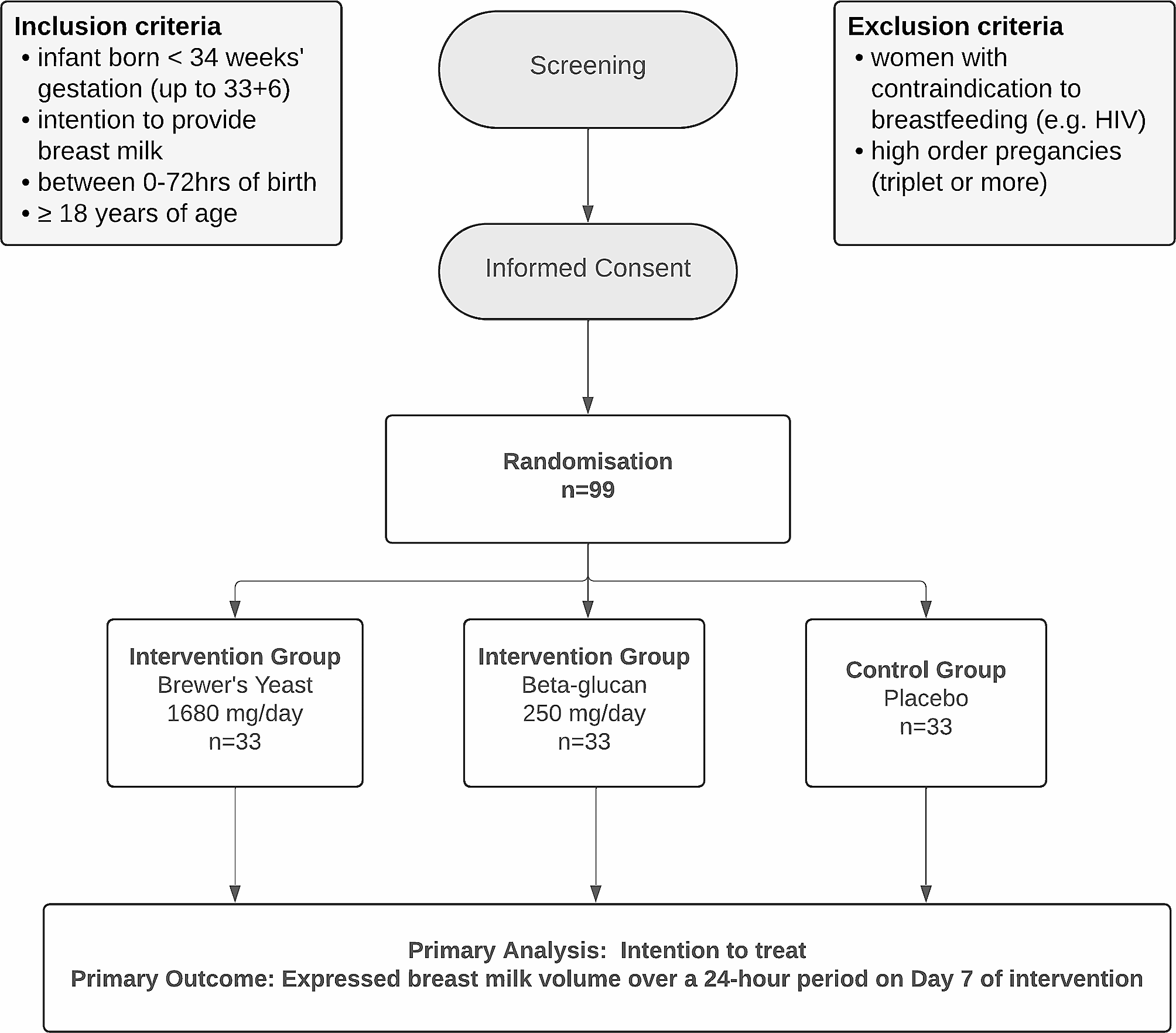
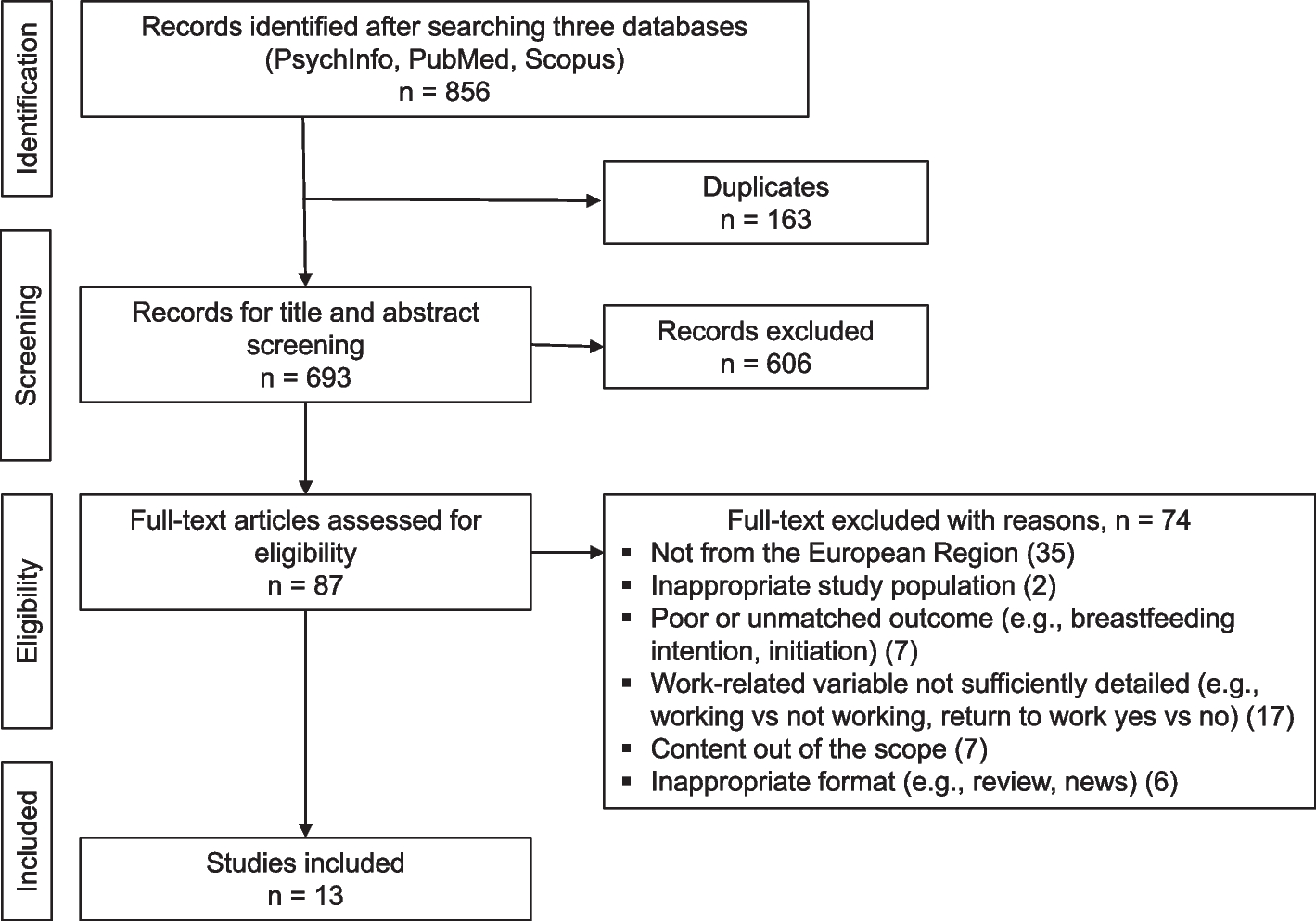
The improved, second version of the model was sent to the experts. A set of questions mostly using scoring/ranking techniques was used to gain consensus on the amended practice model inputs, activities and outcomes and the connections between them. The round two questionnaire consisted of ten questions relating to the importance of the input and activities used in the model on a one-to-five rating scale of 1 = least importance and 5 = high importance. Also, ten four-point Likert-scale statements and four four-point rated (poor, fair, good, excellent) questions relating to the overall design. To determine the importance of the inputs, a mean score and mean percentage score for each stated input were calculated (Fig. 2). Inputs and activities were judged less valid if there was less consensus on their importance. For the input and activity variables, a mean score of 70% (3.5 out of 5) was deemed to be valid for inclusion in the practice model. Therefore, funding for a lactation consultant was removed and a written breastfeeding policy statement as well as the provision of maternity leave benefits were both added to the model, as both scored an overall percentage of 93% (4.65/5).
Fig. 2
Score percentage rating for the inputs and activities in the practice model
After the input from the Delphi round two, the final amendments to the model were made. Following on, the practice model face validity was tested by presenting it to the to the nine workplaces that participated in phase two, during four focus group discussions and one in-depth interview. These participants (n = 16) included human resource practitioners (n = 5), occupational health nurses (n = 2), social workers (n = 2) managers (n = 6) and personal assistant (n = 1). The majority of the participants was from the public sector (n = 8), manufacturing sector (n = 5) and retail sector (n = 3). The Atlas ti programme was used to analyse the qualitative data. The analysis was mainly deductive (having a pre-prepared structure), but also partly inductive, in terms of which emerging themes were built and developed.
留言 (0)