This study analyzed the data of 477,524 patients from the ACS-NSQIP database and revealed that an elevated preoperative liver enzyme level is associated with increased postoperative 30-day mortality in patients undergoing nonemergency orthopedic surgery. Moreover, we identified a linear relationship between preoperative SGOT levels and postoperative 30-day mortality. Our data suggest that an elevated preoperative SGOT level is an independent risk factor for 30-day mortality in patients undergoing orthopedic surgery.
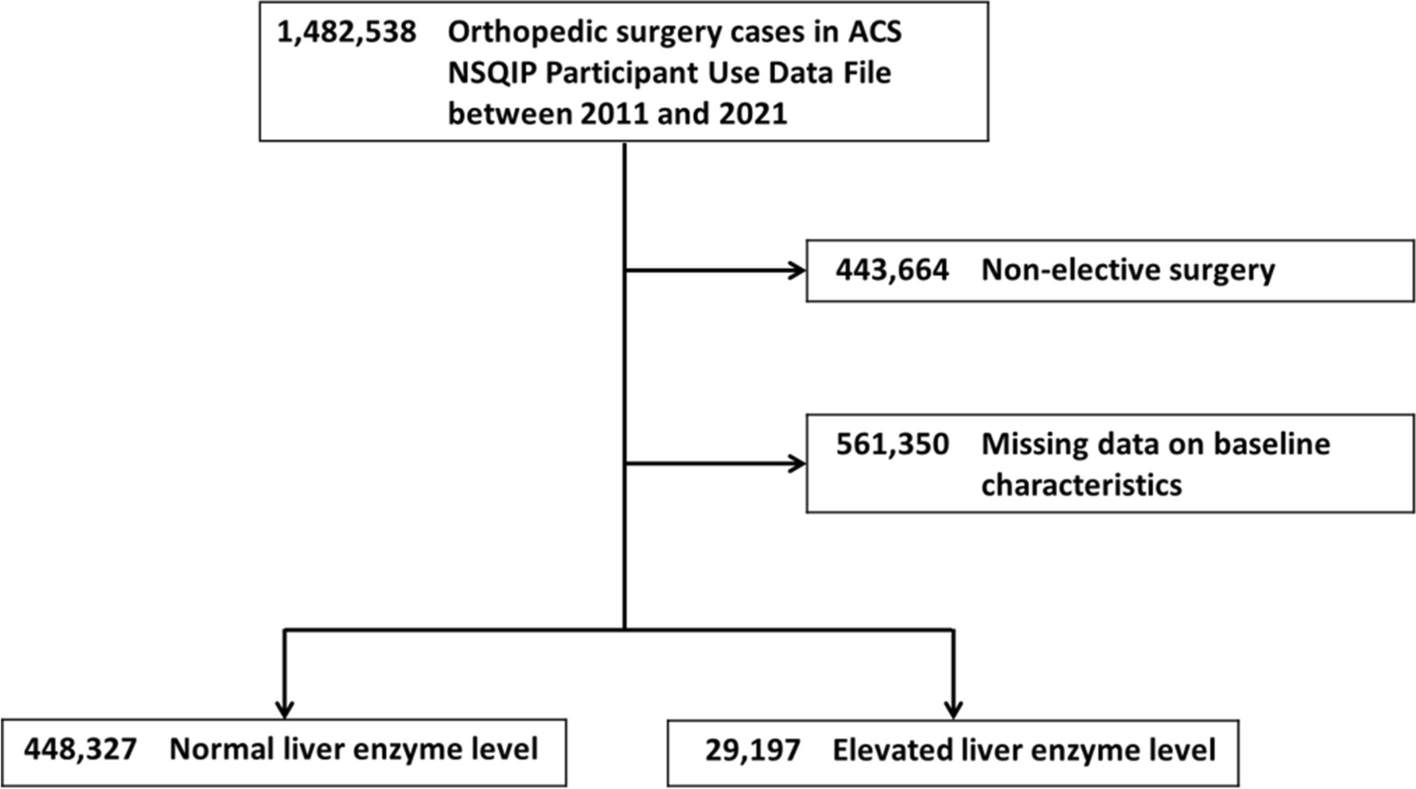
According to our data, 6.1% (29 197) of the patients undergoing orthopedic surgery had elevated preoperative SGOT levels. Similarly, Lobstein et al. reported elevated SGOT levels in 7% of 960 patients without evidence of viral hepatitis who underwent orthopedic surgery (Lobstein et al. 2008). Wiegand et al. investigated two hospital orthopedic surgery cohorts and observed elevated SGOT levels in 11.7% of 1454 patients without hepatitis C (Wiegand et al. 2006). Our findings agree with previous reports that elevated preoperative SGOT levels are common in patients undergoing nonemergency orthopedic surgery. Clinicians should not disregard the negative effect of elevated preoperative SGOT levels on postoperative outcomes.
Studies have examined the association between preoperative SGOT levels and surgical outcomes in cardiac surgery, emergency general surgery, and head and neck surgery (Shang et al. 2021; Narueponjirakul et al. 2020; Abt et al. 2018). In adult patients without liver disease who underwent cardiac surgery, a preoperative abnormal SGOT level was an independent risk factor for in-hospital and 90-day mortality (Shang et al. 2021). In octogenarian patients who received emergency general surgery, an elevated preoperative SGOT level increased the risk of in-hospital and 1-year mortality (Narueponjirakul et al. 2020). Moreover, in head and neck surgery, an abnormal preoperative SGOT level increased the risk of surgical-site infection and 30-day postoperative complications but not mortality (Abt et al. 2018). Using the ACS-NSQIP database, Bishop et al. analyzed the data of 815 077 patients with ASA classifications 1 to 3 who received elective surgery between 1992 and 2001 (Bishop et al. 2008). They found that an elevated SGOT level (SGOT > 40 IU/L) was an independent risk factor for 24-h and 30-day postoperative mortality. In contrast to previous studies, our study not only identified SGOT level as an independent risk factor for 30-day postoperative mortality in patients undergoing nonemergency orthopedic surgery but also demonstrated that SGOT levels are proportionately associated with the risk for 30-day postoperative mortality.
Common hepatic etiologies of mildly elevated liver enzyme levels are viral hepatitis, alcoholic liver disease, cirrhosis, steatohepatitis, and medications (toxins). Acetaminophen, nonsteroidal anti-inflammatory drugs, carbamazepine, phenytoin, and trazodone are common analgesics and adjuvants that can cause liver transaminase elevation in patients undergoing orthopedic surgery (Oh et al. 2017). Certain supplements, including shark cartilage and vitamin A, can also result in reversible cases of elevated liver enzyme levels (Giboney 2005). Additional causes of mild liver enzyme elevation include celiac disease, hemolysis, myopathy, hyperthyroidism, strenuous exercise, and macro-aspartate aminotransferase (AST) (Kwo et al. 2017). Clinicians should carefully evaluate surgical patients with elevated liver enzyme levels to identify the possible etiology and correct reversible factors.
According to the American College of Gastroenterology’s clinical guidelines for the evaluation of abnormal liver chemistries, patients with mildly elevated liver enzyme levels (2 to 5 × ULN) should first be assessed for medicine-related causes, fatty liver disease, and viral hepatitis. Recommended evaluations include an iron panel; tests for liver function, infection, and hepatitis; and an abdominal ultrasound. In the case of negative results, clinicians should repeat the tests after 3 months and consider a liver biopsy to test for autoimmune-related causes (Kwo et al. 2017). However, surgical patients with mildly elevated liver enzyme levels are often identified only 1 day prior to surgery, and the completion of extensive evaluations is difficult without delaying the originally scheduled surgery. We recommend that clinicians consider other risk factors. A previous retrospective cohort study indicated that patients with disseminated cancer, poor functional status, a high ASA classification (ASA 3 vs. 1), weight loss > 10%, or ascites had a high odds ratio for 30-day postoperative mortality (Bishop et al. 2008). Further preoperative evaluation should be considered for patients with elevated preoperative SGOT levels and the aforementioned risk factors. In addition, anesthesia type may influence postsurgical outcomes. Although a retrospective study of 91 patients did not detect significant changes between preoperative and postoperative liver enzyme levels (Sahin et al. 2007), a retrospective Korean study on the effects of total intravenous anesthesia (TIVA) and inhalation anesthesia on liver enzyme levels had divergent findings (Oh et al. 2020). Specifically, the Korean study included 730 patients with elevated preoperative liver enzyme levels who underwent surgery with propofol-based TIVA or inhalation anesthesia. The results indicated lower postoperative SGOT and SGPT levels in both anesthesia groups, but they revealed a significantly lower change in SGPT levels after TIVA than that observed after inhalation anesthesia. However, postoperative liver chemistry changes do not share a definite correlation with postoperative outcomes. Clinicians should consider the effect of anesthesia type in patients with elevated preoperative liver enzyme levels.
This study has several limitations. First, we could not observe long-term outcomes because the ACS-NSQIP database contains only 30-day postoperative outcomes. Furthermore, according to ACS-NSQIP data variable definition, preoperative lab values are drawn within 90 days prior to the primary procedure. In our study population, the mean interval between the acquisition of SGOT level and the surgery was 19.75 days. This gap between obtaining the SGOT levels and the surgery date may pose challenges in accurately reflecting the patient’s current condition on the day of surgery. Despite the data gap, our results demonstrated a significant association between elevated SGOT levels and postoperative 30-day mortality among patients undergoing elective orthopedic surgery. Clinicians are therefore advised to allocate time for thorough patient evaluation and to seek expert consultation to address the underlying causes of elevated SGOT levels. Second, we excluded nearly 40% of the patients undergoing orthopedic surgery owing to missing data on preoperative SGOT levels. A previous study recommended that researchers examine the pattern of data gaps and evaluate the pros and cons of different methods for addressing missing data (Parsons et al. 2011). This study only analyzed the population with complete data. However, patients without data on preoperative SGOT levels may not receive liver function tests because of their relatively healthy condition. This may be a source of potential selection bias in our study. Third, the impact of increased preoperative liver enzyme levels on patients undergoing different types of anesthesia remains unexplored. Theoretically, patients under regional anesthesia have less medication exposure than those receiving general anesthesia. This difference may influence the effect of elevated liver enzyme levels on patient outcomes. Fourth, this study exclusively focused on elective orthopedic surgery. The generalizability of our findings to other procedures should be approached with caution. According to the surgical risk classification of 2022 ESC Guidelines, more than 95% of the patients in our study underwent low (minor orthopedic surgery) to intermediate (major orthopedic surgery: hip or spine surgery) risk surgeries (Halvorsen et al. 2022). Despite this, our study yielded significant results even within the cohort of patients undergoing low to moderate-risk surgeries. We anticipate that focusing on high-risk surgeries would further underscore the significance of our findings. Fifth, there exist several differences in patient characteristics between the two groups, such as ASA classification, type of surgery, age, and others. Despite our efforts to adjust all patient characteristics for the primary outcome and conduct propensity score matching, it is possible that bias or confounding factors, which were not detected or adequately adjusted for, may still be present. Finally, the ACS-NSQIP database does not include SGPT levels, which constitute a more specific marker of hepatocellular injury than do SGOT levels. On the contrary, SGOT serves as a broader systemic marker, and the elevation of SGOT levels does not necessarily signify liver pathology. Moreover, SGOT and SGPT levels can help determine the etiologies of abnormal liver function tests. Further research is warranted to investigate the implications of other liver enzyme abnormalities in postoperative outcomes.







留言 (0)