Research design
This study was approved by the hospital’s medical ethics committee (Scientific Ethics Review No. 18 in 2022). The perioperative data of patients who underwent orthopedic surgery at Shizhu Tujia Autonomous County People’s Hospital, from January 2019 to January 2022, were retrospectively analyzed.
This was a retrospective study; when the data were collected, they were anonymized, i.e., names, hospital ID, and the date of operation were excluded. Therefore, informed consent was not necessary.
Inclusion and exclusion criteria
The inclusion criteria were as follows: (1) age ≥ 65 years and (2) major orthopedic surgery including hip replacement, knee replacement, and spine and limb fracture surgery. The exclusion criteria were as follows: (1) severe combined injury; (2) superficial minor operations, such as debridement and suturing of superficial wounds and mass excision; and (3) incomplete clinical medical records.
Data extraction
Data were extracted from patients’ electronic medical records, anesthesia records, test records, inspection reports, and nursing records.
Observation indicators included (1) patient conditions [age, sex, ASA classification, New York Heart Association (NYHA) classification, education level, hearing level, history of smoking, history of alcoholism, cardiovascular complications (coronary heart disease, hypertension, arrhythmia, etc.), diabetes, preoperative pulmonary diseases (chronic obstructive pulmonary disease (COPD), asthma, silicosis and pulmonary infection), preoperative cognitive impairment, and preoperative biochemical tests, including hemoglobin (Hb), white blood cells (WBC), creatinine (Cr), and neutrophil-to-lymphocyte ratio (NLR)] and (2) surgical and anesthesia factors [surgical site, operation time, anesthesia method, blood loss, fluid volume, blood transfusion, transfer to intensive care unit (ICU) after surgery, postoperative analgesia, and pain score within 48 h after surgery].
Outcomes
The primary outcome was POD, and the secondary outcome was the postoperative length of hospital stay (LOS).
POD is diagnosed using “The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition” (Diagnostic and statistical manual of mental disorders fifth edition [M].Arlington VS:American Psychiatric Association 2013). The diagnosis includes (1) attention and consciousness disorder; (2) short disorder duration (usually hours to days), with fluctuating severity over the course of 1 day; (3) additional cognitive impairment (such as memory deficit, disorientation, visual or language impairment); (4) attention deficit, disorder of consciousness, and cognitive dysfunction that cannot be explained by the primary disease or known cognitive impairment; and (5) medical history, physical examination, or laboratory findings show that the disorder is the result of other physical illnesses, such as substance intoxication or withdrawal, toxin exposure, or multiple factors.
POD usually be diagnosed in the general ward or ICU, sometimes in emergency room, which should be distinguished from emergency agitation. Emergency agitation was defined as a Richmond Agitation–Sedation Scale (RASS) score of + 3 or + 4 or the administration of haloperidol during the PACU stay (Sessler et al. 2002).
Missing values
Data cleaning was performed before the statistical analyses, and variables with more than 10% missing values were not included. For continuous variables with missing values (< 10%), the mean was used instead if the data were normally distributed, or the median was used if the data were nonnormally distributed. Patientes with missing categorical variable data were removed.
Statistical analysis
Categorical variables are represented by the number of cases, and the chi-square test was used to compare 2 groups. Continuous variables are expressed as medians and interquartile ranges (IQRs), and the t tests or rank-sum tests were used to compare 2 groups. Stata MP 14.2 statistical software was used, and a P value < 0.05 was considered statistically significant. Univariate logistic regression was used to screen risk factors, and risk factors with a P value < 0.05 in the univariate logistic regression were included in the multivariate logistic regression analysis. Stepwise regression was also used to screen variables to construct the predictive models. All risk factors were dichotomized, and cutoff values for variables were based on commonly used clinical criteria or references.
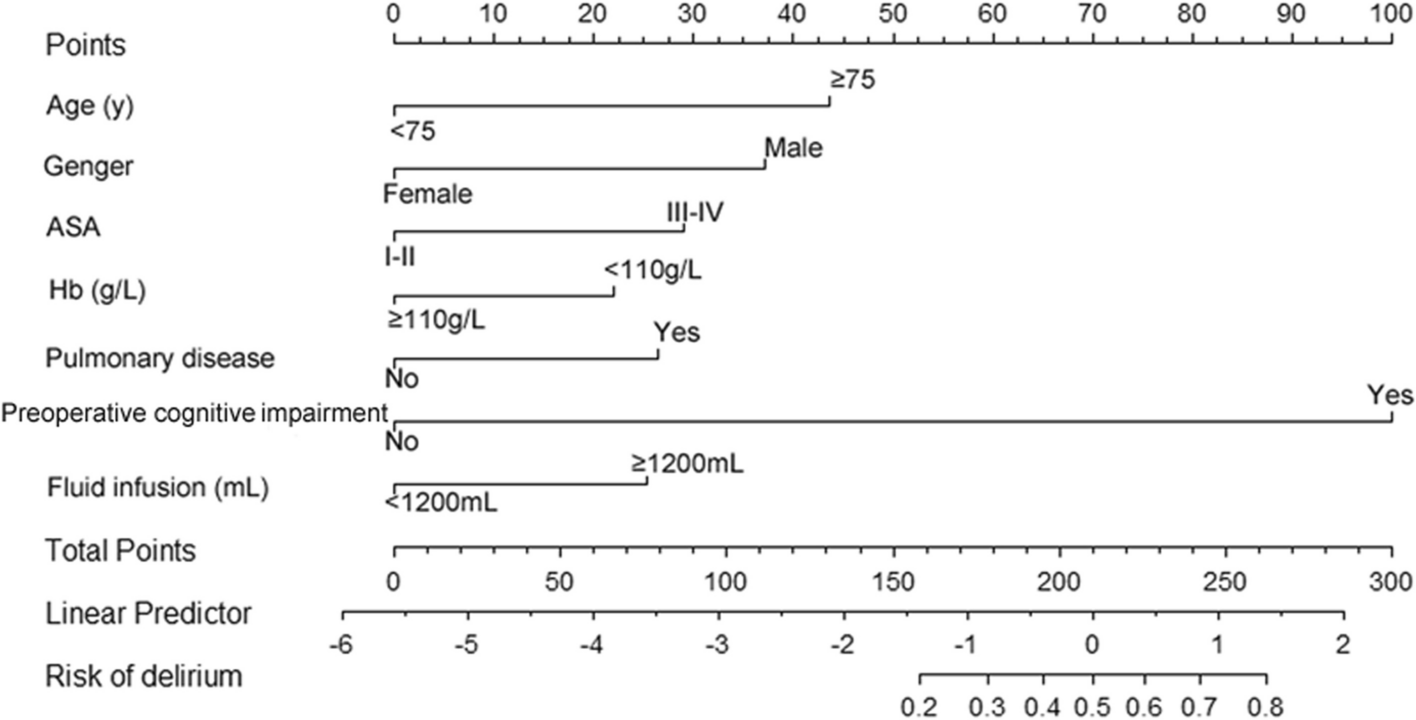
The screened risk factors were introduced into R software version 4.1.2 (R Foundation for Statistical Computing), and the rms package was used to construct a nomogram for predicting the risk of POD in elderly patients undergoing orthopedic surgery. The internal validation of the model adopted the bootstrap method, and repeated sampling was performed 200 times for validation. The area under the receiver operating characteristic (ROC) curve (AUC) was used to evaluate the discrimination of the nomogram, a calibration curve was drawn to test the accuracy of the nomogram, and decision curve analysis (DCA) was used to evaluate the range of clinical validity of the nomogram.







留言 (0)