



記住我









In adults, aphasia is a common symptom of stroke, affecting approximately 30% of all patients being affected (1, 2). It is more common in patients who had left hemispheric stroke (1), and those with exclusively hemorrhagic etiology have a slightly lower incidence than that of those with ischemic or mixed etiologies (1). In particular, lesions to the superior temporal lobe are associated with persistent aphasia syndromes (3). Data on recovery from aphasia is limited. Typically, aphasia often is a persisting impairment with less than 24% of the affected patients fully recovering within 18 months (1). Although most patients show signs of recovery during the first 6 months after stroke (3), improvement can be observed until much later (3, 4).
After perinatal stroke, language development may be delayed, and compared to healthy controls, children after perinatal stroke often score significantly lower on standardized language tests well into middle childhood (5–7). A large part of this effect, however, can be attributed to epilepsy (5, 8). In children without epilepsy, often only subtle deficits in language function are detected (9, 10), if any (11).
Language development after perinatally acquired left hemispheric lesions is probably the most prominent example of early brain plasticity. Contrary to recovery from aphasia in adults, which heavily relies on the perilesional remainders of the left hemispheric language network (12), language development after perinatal left hemispheric brain lesions is often associated with atypically right hemispheric language representation (11, 13–16). The driving factors for inter- vs. intrahemispheric language representation in this patient group are still subject to research (7, 17). Of note, this compensatory hemispheric reorganization is not always better: in smaller left hemispheric lesions, typical language representation might be associated with better functional outcomes than if atypical language representation ensues (6).
Ischemic stroke occurring after the neonatal period (“childhood stroke”) has an incidence of 1–3 in 100,000 children per year (18, 19). It is therefore rarer than perinatal stroke (4 in 10.000 live births per year (19), despite the neonatal period lasting only 4 weeks. General cognitive functioning after such incidents seems to be less favorable when the stroke happened early as compared to late childhood (20, 21); however, the relationship between age at insult and outcome is probably non-linear (22). In comparison to healthy controls, children after childhood stroke score lower in expressive and receptive language tests (15). Data on aphasia resulting from childhood stroke is limited and is complicated by the fact that even the definition of aphasia in children is not universally agreed upon (23). Although many clinicians would probably agree that aphasia after stroke is less common in children than in adults, the limited data available suggests that, as in adults, about one-third of all childhood stroke incidents seem to result in aphasic symptoms (23). With regard to recovery, however, the natural course in children and adolescents is better (24): 6 months after an acquired brain injury, only a small fraction of children still show severe language problems, much less than in a comparable cohort of young adults (25). Interhemispheric language reorganization does not seem to be a common compensatory mechanism in childhood stroke, since most affected individuals have typical left hemispheric representation (15). Right-sided language representation is significantly associated with younger age at injury (24, 26). Due to small sample sizes, data on the quality of language recovery from aphasia after childhood brain lesions is limited, and the moderating factors remain unclear.
In this retrospective cross-sectional observation study, we explored the long-term language outcome after unilateral brain lesions acquired during childhood and adolescence. Patients with perinatally acquired unilateral brain lesions and typically developing individuals without brain lesions were included as control groups.
Although stroke is often considered less disabling in children than in adults, we hypothesized that individuals with childhood lesions (CHILD) would have worse language function than healthy controls (CONTROL) of the same age (H1). In comparison to the patient control group with perinatal strokes (PERI), we also expected worse language outcome (H2).
Materials and methods SubjectsParticipants were recruited in two large neuropediatric centers in Germany (University Children's Hospital Tübingen and Schön Klinik Vogtareuth) by searching the clinical database, by personal contacts, and during hospitalization, using the same in- and exclusion criteria. Typically developing controls were recruited from the general population through advertisements in the local press and the clinic’s internal information system. After they contacted our study staff members, they were screened using a questionnaire asking for any neurological or psychiatric diagnosis and problems in cognitive or language development. A formal assessment confirming normal development was not used.
General inclusion criteria were German as a native language and age ≥ 8 years at study participation. The general exclusion criteria included contraindications for MRI, a previous neurological or psychiatric diagnosis (apart from the brain lesion in the patient groups), and a previous diagnosis of intellectual disability (IQ below 70). Therefore, we relied on the medical history or the self-reported intelligence scores. Additionally, standardized non-verbal IQ scores were acquired during the study procedure from the Test of Non-verbal Intelligence—Fourth Edition (TONI-4), and participants with a non-verbal IQ below 70 were excluded.
The CHILD group included nine patients (three female, median age = 13.5 years, range 8–27 years, six left-sided lesions) with unilateral brain lesions such as ischemic or hemorrhagic infarctions acquired at the age between 29 days and 18 years and at least 1 year before study participation.
The PERI group (patient control group) included 23 patients with perinatally acquired unilateral brain lesions such as ischemic or hemorrhagic infarctions at an age before 29 days (11 female, median age = 12.5 years, range 8–26 years, 16 left-sided lesions).
The CONTROL group included 33 typically developing individuals (15 female, median age = 12.33, range 8–29 years).
The majority of the children in the patient groups attended a regular school. Five children attended a school for children with special needs, while six children attended a regular school with a school escort providing support, mostly due to their motor impairment. Data about school type was missing in two cases.
The study was approved by the local ethics committee at the University Hospital Tübingen (No. 693/2014B01). All adult participants and the parents of underage participants gave their written, informed consent. The study was performed in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki in its latest implementation).
Structural and functional MRIThe participants were examined with a Siemens 1.5 T Avanto (Tübingen) or Symphony (Vogtareuth) MRI scanner. Functional and anatomical images were analyzed with SPM12 (Statistical Parametric Mapping; Wellcome Department of Imaging Neurosciences, UCL, UK), CAT12 (by Christian Gaser and Robert Dahnke, Departments of Psychiatry and Neurology, Jena University Hospital), and Matlab (MathWorks, Natick MA, USA). Lesion size was determined with a semiautomated approach (27).
Language lateralization was determined by fMRI using the vowel identification task (17, 28, 29). More information about the MRI sequences and data processing and analysis steps can be found in (30).
Neuropsychological protocolTo assess language abilities, participants completed two different tests: the German version of the Peabody Picture Vocabulary Test-III (PPVT) and the German version of the Potsdam Illinois Test of Psycholinguistic Abilities (P-ITPA). The PPVT measures the subject's receptive vocabulary ability (31). German standardized age norms cover the range from 13 to 71 years. The P-ITPA (Language Development Score) is a more comprehensive battery containing measurements of verbal intelligence, expressive vocabulary, expressive language skills, phonological awareness, and verbal short-term memory (32). Standardized age norms cover the range from 4;0 to 11;6 years. For participants aged 11;6 years or younger, the appropriate age norms of the P-ITPA were applied, and for participants aged 13;0 years or older, the appropriate age norms of the PPVT were applied. One patient and three controls were out of the age ranges of both tests (11;8–12;10 years old). Here, we used the oldest group of P-ITPA for the two subjects aged <12 years and the youngest group of the PPVT for the two subjects aged >12 years.
For the assessment of non-verbal intelligence, we used the TONI-4, a motor-independent intelligence test that measures the ability for abstract reasoning. Standardized age norms cover the range from 6;0 to 89;11 years (33).
Statistical analysisWithin our sample, the raw scores of P-ITPA and PPVT were highly correlated (r = .845; 95% CI [.756,.903). Since the actuality of standardization was strongly divergent between the tests, we subjected the age-appropriate T-scores (for each participant either P-IPTA or PPVT) and index scores (TONI-4) of the participants to a study-specific z-transformation. The resulting z-score of the age-appropriate language test (either P-ITPA or PPVT) was then transferred to the new variable “language score.”
We then conducted a univariate analysis of covariance (ANCOVA), with the factor group (CHILD vs. PERI vs. CONTROL) and the independent variable “language score” (either P-ITPA or PPVT sample-standardized z-score, according to age). We introduced the covariates “language test” (i.e., the use of P-ITPA or PPVT) and IQ (TONI-4 z-score).
Since epilepsy was present only in the PERI group, we were not able to use epilepsy as a covariate. Thus, we repeated the same analysis with only those PERI patients without epilepsy post hoc.
To identify potential modifiers of language performance in the patient groups, we conducted separate correlation analyses between the variable “language score” and sex (male vs. female), age at injury, intelligence (TONI-4), lesion side (left vs. right), lesion volume (vol), and language lateralization index (LI). The significance threshold was Bonferroni-corrected for multiple tests, resulting in a threshold of p = 0.05/6 = .0083.
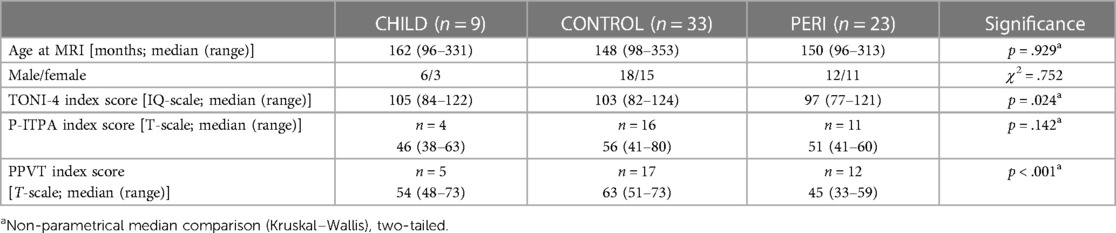
ResultsIndividual patient characterization can be found in Table 1. Group comparisons are shown in Table 2.
Table 1. Patient characteristics.
Table 2. Sample characterization.
CHILD group: Six out of nine patients had a left-sided stroke. Of these, four initially presented with aphasia from which all had recovered at the time of study. No patient in this group had epilepsy. In one child with a left-sided stroke, the functional MRI activation was not strong enough for interpretation of the language lateralization score. The remainder of the group showed a left-sided activation pattern.
PERI group: 8 out of 23 patients had epilepsy (three drug-resistant), and 16/23 patients had a left-sided lesion. Of these, seven had a typical left-sided language representation and eight had an atypical pattern (one patient without interpretable fMRI). Of the nine patients with right-sided lesions, one had an atypical language activation pattern.
Language lateralization differed significantly between the three groups (ANOVA, F2,57 = 18.093, p < .001). Post hoc Scheffé tests revealed that group PERI had significantly less leftward-oriented language than the other two groups (mean LI CHILD = .786, mean LI PERI = .125, mean LI CONTROL = .772; p < .001). Also, non-verbal intelligence differed significantly between the three groups (ANOVA, F2,62 = 3.912, p = .025). Post hoc Scheffé tests revealed that group PERI scored significantly lower than group CONTROL, but not significantly lower than group CHILD (mean TONI-z CHILD = 0.238, mean TONI-z PERI = −0.45, mean TONI-z CONTROL = 0.253, p = .033).
Testing our main hypothesis, the ANCOVA revealed a significant group effect for language score, after correcting for language test version and intelligence (F2,60 = 8.059; p = .001). Both patient groups scored significantly lower than the control group (mean corrected language score CHILD = −0.299, mean corrected language score PERI = −0.378, mean corrected language score CONTROL = 0.410), as depicted in Figure 1.
Figure 1. Group differences in language performance.
After the exclusion of patients with epilepsy from the PERI group, the results remained largely the same: A significant group effect on language score (F2,45 = 6.701; p = .003), with both patient groups scoring significantly lower than the control group (mean corrected language score CHILD = −0.237, mean corrected language score PERI = −0.214, mean corrected language score CONTROL = 0.451).
For group CHILD, none of the potential modifiers lesion side, sex, lesion size, age at the time of injury, or time since the event correlated significantly with language scores (Table 3A). In group PERI, language performance was significantly associated with sex (r = −0.517, p = .012), but not with any of the other variables (Table 3B).
Table 3. Correlation coefficients between potential modifiers and language performance in patients with postneonatal childhood stroke (A) and patients with perinatal stroke (B).
DiscussionOur main finding is that unilateral brain lesions acquired in childhood and adolescence can lead to chronic language deficits, regardless of the hemisphere affected. This result is both surprising and of clinical relevance.
Language reorganization after left hemispheric lesions to the developing brain (with, unlike in adults, the right hemisphere has the potential to “take over”) is probably the best-known example of the special compensatory potential of a child's central nervous system (“developmental plasticity”). Many studies have demonstrated that pre- and perinatally acquired left hemispheric brain lesions often lead to atypical right hemispheric language representation (13, 15, 16, 34, 35), a compensatory mechanism that does obviously not belong to the repertoire of a mature brain. Atypical right hemispheric language representation is probably the reason for the relatively good language outcome in these individuals, which is clearly better than the chronic aphasia seen in adults with comparable brain lesions (36). However, there is also broad evidence that a perinatally acquired brain lesion can impair language function when compared to that of individuals with non-lesioned brains (5, 22, 37–39), although the presence of epilepsy may be a decisive factor (8). The fact that we now show here that individuals with a history of unilateral brain lesions acquired in childhood, and without epilepsy, perform below healthy controls in language tests, therefore is unexpected.
Due to the low incidence of childhood stroke, data on language outcome of these patients is only just accumulating. Post-stroke acquired aphasia affects approximately one-third of childhood stroke patients [here defined as “acquired after the age of two years” (23)] and is therefore as common in children and adolescents as it is in adults (1). However, younger individuals seem to fully recover more often from stroke-induced aphasia than older ones (40). Indeed, while a substantial proportion of adults have aphasic symptoms years after the incident, chronic aphasia is extremely rare in children and adolescents. The neurological mechanism underlying this recovery is different from the one following lesions acquired in the neonatal period since successful interhemispheric reorganization of language is uncommon following brain lesions acquired after the age of two to three years (15, 24). This was the rationale for our hypothesis that patients with perinatal stroke would have better language function than patients with postneonatal stroke. However, this was not the case: While both patient groups had significantly lower language scores than healthy controls after correcting for general intelligence, no significant difference was detectable between the two patient groups (PERI and CHILD). Although the absence of significance is not evidence for equality, Figure 1 illustrates a striking overlap between the two groups. After controlling for the effect of epilepsy by excluding patients with epileptic seizures from the perinatal group, the groups converged even more. Thus, our results imply that a complex function such as language depends on an intact central nervous system.
Non-verbal fluid reasoning, however, seems to be more robust. In a previous study focusing on patients with perinatal brain lesions with or without epilepsy, we did not detect a significant difference in verbal function between healthy controls and patients with left hemispheric lesions without epilepsy (8). Our current results seem to contradict this finding, since both our patient groups differed significantly from controls in their language scores. As illustrated in Table 2, the controls' non-verbal intelligence lies within the middle normal range, arguing against a recruitment bias. A reason for the different results could, however, be our approach to language testing. In the previous study, we analyzed raw scores of the P-ITPA test for all participants and corrected for age in the analyses (8). For the current study, we used age-appropriate standard scores for P-ITPA or PPVT. Therefore, while sacrificing the advantage of homogeneous sets of tasks for all participants, we gained the advantage of acquiring age-appropriate standard scores for all participants. In post hoc analyses (available in the Supplementary Material), the significant difference between controls and patients with perinatal brain lesions is driven by the PPVT scores used for individuals older than 12 years. Interestingly, when analyzing the PPVT raw scores in the younger sample, no group effect can be identified, while an analysis of the P-ITPA raw scores for the older sample only reveals a significant group effect, even after excluding the patients with epilepsy. Thus, the older patients with perinatal lesions seem to have more prominent language difficulties than the younger ones, irrespective of the test used. This phenomenon of “growing into deficit” during late childhood and adolescence has been described before for general cognitive abilities in patients with neonatal stroke (41). In the future, systematically assessing older children and adolescents may help correct the picture that no (language or cognitive) deficits ensue following childhood stroke.
An additional conclusion to be drawn from our results is that lesion side does not seem to have a significant impact on language function in the chronic phase of recovery. This is all the more interesting as all patients with acute aphasia had a left hemispheric lesion, implying that the likely bilateral networks necessary to support complex functions such as language require sufficient neural substrate to develop.
The clinical impact of the long-term language impairment in both our patient groups is substantial. Although children and adolescents usually do recover from aphasia, the more subtle language problems we have identified here may significantly impair both the academic and social participation of the individuals, especially if the deficits become more obvious during late childhood. It was previously shown that in school-aged children, language proficiency significantly predicts reading abilities, secondary school achievement, and later occupational attainment (42). Language impairment may therefore critically influence social interaction and participation both in the family setting and, even more, in extrafamilial contexts (43). Thus, rehabilitation of children and adolescents with stroke should always keep an eye on language skills, even after clear aphasic symptoms have long since resolved.
LimitationsThe main limitation of our study remains the small sample size (CHILD, n = 9; PERI, n = 23; CONTROL, n = 33), which reduces statistical power and makes conclusions less generalizable. It must be considered, however, that childhood stroke is a rare event (18). Therefore, the recruitment of these patients is difficult and studies including a sufficiently large number of individuals for fine-grained analyses of modulating factors and interactions are, unfortunately, very difficult to conduct. Our results have therefore been considered as “preliminary.” The long-term language outcome should be investigated further in the future—ideally as multicenter studies and with the aid of more homogenous standardized tests. The need for two different language tests, due to the age of the participants, is another limitation of our study. However, in the absence of a standardized language test suitable for German-speaking individuals between 8 and 30 years, we had to use two different assessments. In our current analyses, we traded test homogeneity for age appropriateness, leading to a different perspective on the group comparisons than in a previous study using a different approach. Another limitation of our study is that there was no additional evaluation of psychiatric components and neurodevelopmental disorders carried out by a child neuropsychiatrist to guarantee the exclusion criteria. However, the existing medical records of the clinical databases were screened for psychiatric and neurological comorbidities for the patient group and, if available, previously performed neuropsychological tests were considered. A further limitation is that we have not collected data on learning disorders. Hence, we cannot exclude that despite average scores in non-verbal cognitive abilities, our patients show deficits in these aspects of cognition. Also, we have not collected data on the sociocultural and family context of our participants and therefore cannot exclude that they differ in the sociocultural and family context.
ConclusionWe demonstrate that in childhood stroke (and similar to perinatally acquired stroke), lesion side does not clearly predict later language impairment, in agreement with previous studies (8, 44). Further, language impairment may only become obvious long after the initial insult, likely reflecting a “growing into deficit” mechanism. We therefore suggest following up language function not only in left hemispheric but also in right hemispheric childhood stroke and to continue to do so even after initial aphasic symptoms have resolved.
Data availability statementThe raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statementThis study involving humans was approved by the University Hospital Tübingen Ethics Committee (Nr. 693/2014B01). This study was conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributionsMH: Data curation, Formal Analysis, Investigation, Writing – original draft, Writing – review & editing. AG: Data curation, Formal Analysis, Investigation, Visualization, Writing – original draft, Writing – review & editing. LS: Formal Analysis, Methodology, Supervision, Writing – review & editing. MS: Conceptualization, Funding acquisition, Resources, Supervision, Writing – review & editing. MW: Methodology, Software, Supervision, Writing – review & editing. KL: Conceptualization, Formal Analysis, Funding acquisition, Methodology, Supervision, Writing – review & editing.
FundingThe authors declare financial support was received for the research, authorship, and/or publication of this article.
Deutsche Forschungsgemeinschaft, Grant/Award Number: DFG LI1925/4-1.
AcknowledgmentsWe are grateful to all study participants and their families, as well as all clinicians at the two centers supporting our study.
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary materialThe Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2024.1338855/full#supplementary-material
References1. Flowers HL, Skoretz SA, Silver FL, Rochon E, Fang J, Flamand-Roze C, et al. Poststroke aphasia frequency, recovery, and outcomes: a systematic review and meta-analysis. Arch Phys Med Rehabil. (2016) 97(12):2188–201. e2188. doi: 10.1016/j.apmr.2016.03.006
PubMed Abstract | Crossref Full Text | Google Scholar
2. Grönberg A, Henriksson I, Stenman M, Lindgren AG. Incidence of aphasia in ischemic stroke. Neuroepidemiology. (2022) 56(3):174–82. doi: 10.1159/000524206
Crossref Full Text | Google Scholar
4. Martin KC, Ketchabaw WT, Turkeltaub PE. Plasticity of the language system in children and adults. Handb Clin Neurol. (2022) 184:397–414. doi: 10.1016/B978-0-12-819410-2.00021-7
PubMed Abstract | Crossref Full Text | Google Scholar
5. Ballantyne AO, Spilkin AM, Hesselink J, Trauner DA. Plasticity in the developing brain: intellectual, language and academic functions in children with ischaemic perinatal stroke. Brain. (2008) 131(Pt 11):2975–85. doi: 10.1093/brain/awn176
PubMed Abstract | Crossref Full Text | Google Scholar
6. Beharelle AR, Dick AS, Josse G, Solodkin A, Huttenlocher PR, Levine SC, et al. Left hemisphere regions are critical for language in the face of early left focal brain injury. Brain. (2010) 133(Pt 6):1707–16. doi: 10.1093/brain/awq104
PubMed Abstract | Crossref Full Text | Google Scholar
7. Ilves N, Männamaa M, Laugesaar R, Ilves N, Loorits D, Vaher U, et al. Language lateralization and outcome in perinatal stroke patients with different vascular types. Brain Lang. (2022) 228:105108. doi: 10.1016/j.bandl.2022.105108
PubMed Abstract | Crossref Full Text | Google Scholar
8. Gschaidmeier A, Heimgärtner M, Schnaufer L, Driever PH, Wilke M, Lidzba K, et al. Cognitive development after perinatal unilateral infarctions: no evidence for preferential sparing of verbal functions. Eur J Paediatr Neurol. (2022) 37:8–11. doi: 10.1016/j.ejpn.2021.12.007
PubMed Abstract | Crossref Full Text | Google Scholar
9. Schwilling E, Krägeloh-Mann I, Konietzko A, Winkler S, Lidzba K. Testing the language of German cerebral palsy patients with right hemispheric language organization after early left hemispheric damage. Clin Linguist Phon. (2012) 26(2):135–47. doi: 10.3109/02699206.2011.595525
PubMed Abstract | Crossref Full Text | Google Scholar
10. Knecht M, Lidzba K. Processing verbal morphology in patients with congenital left-hemispheric brain lesions. Brain Lang. (2016) 157-158:25–34. doi: 10.1016/j.bandl.2016.04.011
PubMed Abstract | Crossref Full Text | Google Scholar
11. Newport EL, Seydell-Greenwald A, Landau B, Turkeltaub PE, Chambers CE, Martin KC, et al. Language and developmental plasticity after perinatal stroke. Proc Natl Acad Sci U S A. (2022) 119(42):e2207293119. doi: 10.1073/pnas.2207293119
PubMed Abstract | Crossref Full Text | Google Scholar
12. Saur D, Lange R, Baumgaertner A, Schraknepper V, Willmes K, Rijntjes M, et al. Dynamics of language reorganization after stroke. Brain. (2006) 129(Pt 6):1371–84. doi: 10.1093/brain/awl090
PubMed Abstract | Crossref Full Text | Google Scholar
13. Rasmussen T, Milner B. The role of early left-brain injury in determining lateralization of cerebral speech functions. Ann N Y Acad Sci. (1977) 299:355–69. doi: 10.1111/j.1749-6632.1977.tb41921.x
PubMed Abstract | Crossref Full Text | Google Scholar
14. Guzzetta A, Pecini C, Biagi L, Tosetti M, Brizzolara D, Chilosi A, et al. Language organisation in left perinatal stroke. Neuropediatrics. (2008) 39(3):157–63. doi: 10.1055/s-0028-1085465
PubMed Abstract | Crossref Full Text | Google Scholar
15. Ilves P, Tomberg T, Kepler J, Laugesaar R, Kaldoja ML, Kepler K, et al. Different plasticity patterns of language function in children with perinatal and childhood stroke. J Child Neurol. (2014) 29(6):756–64. doi: 10.1177/0883073813489350
PubMed Abstract | Crossref Full Text | Google Scholar
16. Szaflarski JP, Allendorfer JB, Byars AW, Vannest J, Dietz A, Hernando KA, et al. Age at stroke determines post-stroke language lateralization. Restor Neurol Neurosci. (2014) 32(6):733–42. doi: 10.3233/RNN-140402
PubMed Abstract | Crossref Full Text | Google Scholar
17. Lidzba K, de Haan B, Wilke M, Krageloh-Mann I, Staudt M. Lesion characteristics driving right-hemispheric language reorganization in congenital left-hemispheric brain damage. Brain Lang. (2017a) 173:1–9. doi: 10.1016/j.bandl.2017.04.006
PubMed Abstract | Crossref Full Text | Google Scholar
18. deVeber G, Roach ES, Riela AR, Wiznitzer M. Stroke in children: recognition, treatment, and future directions. Semin Pediatr Neurol. (2000) 7(4):309–17. doi: 10.1053/spen.2000.20074
PubMed Abstract | Crossref Full Text | Google Scholar
19. Gao L, Lim M, Nguyen D, Bowe S, MacKay MT, Stojanovski B, et al. The incidence of pediatric ischemic stroke: a systematic review and meta-analysis. Int J Stroke. (2023) 18(7):765–72. doi: 10.1177/17474930231155336
PubMed Abstract | Crossref Full Text | Google Scholar
20. Westmacott R, Askalan R, Macgregor D, Anderson P, Deveber G. Cognitive outcome following unilateral arterial ischaemic stroke in childhood: effects of age at stroke and lesion location. Dev Med Child Neurol. (2010) 52(4):386–93. doi: 10.1111/j.1469-8749.2009.03403.x
PubMed Abstract | Crossref Full Text | Google Scholar
21. Studer M, Boltshauser E, Capone Mori A, Datta A, Fluss J, Mercati D, et al. Factors affecting cognitive outcome in early pediatric stroke. Neurology. (2014) 82(9):784–92. doi: 10.1212/WNL.0000000000000162
PubMed Abstract | Crossref Full Text | Google Scholar
22. Fuentes A, Deotto A, Desrocher M, deVeber G, Westmacott R. Determinants of cognitive outcomes of perinatal and childhood stroke: a review. Child Neuropsychol. (2016) 22(1):1–38. doi: 10.1080/09297049.2014.969694
PubMed Abstract | Crossref Full Text | Google Scholar
23. Gilardone G, Viganò M, Cassinelli D, Fumagalli FM, Calvo I, Gilardone M, et al. Post-stroke acquired childhood aphasia. A scoping review. Child Neuropsychol. (2023) 29(8):1268–93. doi: 10.1080/09297049.2022.2156992
PubMed Abstract | Crossref Full Text | Google Scholar
24. Lidzba K, Küpper H, Kluger G, Staudt M. The time window for successful right-hemispheric language reorganization in children. Eur J Paediatr Neurol. (2017b) 21(5):715–21. doi: 10.1016/j.ejpn.2017.06.001
PubMed Abstract | Crossref Full Text | Google Scholar
25. Goeggel Simonetti B, Cavelti A, Arnold M, Bigi S, Regényi M, Mattle HP, et al. Long-term outcome after arterial ischemic stroke in children and young adults. Neurology. (2015) 84(19):1941–7. doi: 10.1212/WNL.0000000000001555
PubMed Abstract | Crossref Full Text | Google Scholar
26. Lidzba K, Bürki SE, Staudt M. Predicting language outcome after left hemispherotomy: a systematic literature review. Neurol Clin Pract. (2021) 11(2):158–66. doi: 10.1212/CPJ.0000000000000852
PubMed Abstract | Crossref Full Text | Google Scholar
28. Wilke M, Lidzba K, Staudt M, Buchenau K, Grodd W, Krageloh-Mann I. An fMRI task battery for assessing hemispheric language dominance in children. Neuroimage. (2006) 32(1):400–10. doi: 10.1016/j.neuroimage.2006.03.012
PubMed Abstract | Crossref Full Text | Google Scholar
29. Meinhold T, Hofer W, Pieper T, Kudernatsch M, Staudt M. Presurgical language fMRI in children, adolescents and young adults. Clin Neuroradiol. (2020) 30(4):691–704. doi: 10.1007/s00062-019-00852-7
PubMed Abstract | Crossref Full Text | Google Scholar
30. Schnaufer L, Gschaidmeier A, Heimgärtner M, Driever PH, Hauser T-K, Wilke M, et al. Atypical language organization following perinatal infarctions of the left hemisphere is associated with structural changes in right-hemispheric grey matter. Dev Med Child Neurol. (2024a) 66(3):353–61. doi: 10.1111/dmcn.15751
PubMed Abstract | Crossref Full Text | Google Scholar
31. Dunn LM, Dunn DM. PPVT-4: Peabody picture vocabulary test, Pearson Assessments (2007).
32. Esser Gn, Wyschkon A. (2010). P-IPTA deutsche Fassung des Illinois test of psycholinguistic abilities, 3rd ed (ITPA-3) von D.D. Hammill, N. Mather & R. Roberts: Manual.
33. Brown L, Sherbenou RJ, Johnsen SK. Test of nonverbal intelligence: TONI-4, Pro-ed Austin. TX. (2010).
34. Staudt M, Lidzba K, Grodd W, Wildgruber D, Erb M, Krageloh-Mann I. Right-hemispheric organization of language following early left-sided brain lesions: functional MRI topography. Neuroimage. (2002) 16(4):954–67. doi: 10.1006/nimg.2002.1108
PubMed Abstract | Crossref Full Text | Google Scholar
36. Tsouli S, Kyritsis AP, Tsagalis G, Virvidaki E, Vemmos KN. Significance of aphasia after first-ever acute stroke: impact on early and late outcomes. Neuroepidemiology. (2009) 33(2):96–102. doi: 10.1159/000222091
PubMed Abstract | Crossref Full Text | Google Scholar
38. Lõo S, Ilves P, Männamaa M, Laugesaar R, Loorits D, Tomberg T, et al. Long-term neurodevelopmental outcome after perinatal arterial ischemic stroke and periventricular venous infarction. Eur J Paediatr Neurol. (2018) 22(6):1006–15. doi: 10.1016/j.ejpn.2018.07.005
Crossref Full Text | Google Scholar
40. O'Hare A. Management of developmental speech and language disorders. Part 2: acquired conditions. Arch Dis Child. (2016) 101(3):278–83. doi: 10.1136/archdischild-2014-306153
Crossref Full Text | Google Scholar
41. Westmacott R, MacGregor D, Askalan R, deVeber G. Late emergence of cognitive deficits after unilateral neonatal stroke. Stroke. (2009) 40(6):2012–9. doi: 10.1161/STROKEAHA.108.533976
PubMed Abstract | Crossref Full Text | Google Scholar
42. Guglielmi RS. Native language proficiency, English literacy, academic achievement, and occupational attainment in limited-English-proficient students: a latent growth modeling perspective. J Educ Psychol. (2008) 100(2):322–42. doi: 10.1037/0022-0663.100.2.322
Crossref Full Text | Google Scholar
43. Sylvestre A, Brisson J, Lepage C, Nadeau L, Deaudelin I. Social participation of children age 8–12 with SLI. Disabil Rehabil. (2016) 38(12):1146–56. doi: 10.3109/09638288.2015.1074730
PubMed Abstract | Crossref Full Text | Google Scholar
44. van Buuren LM, van der Aa NE, Dekker HC, Vermeulen RJ, van Nieuwenhuizen O, van Schooneveld MM, et al. Cognitive outcome in childhood after unilateral perinatal brain injury. Dev Med Child Neurol. (2013) 55(10):934–40. doi: 10.1111/dmcn.12187
留言 (0)