
記住我

KEY POINTS Closed loop ventilation automates ventilator settings that are typically manually adjusted by the user during conventional ventilation. This systematic review identified 51 studies regarding six closed loop ventilation modes. Closed loop ventilation is at least as effective in choosing lung protective ventilator settings as ventilation performed by ICU professionals. Closed loop ventilation has the potential to decrease ICU staff workload, and even improve patient outcomes, although these findings are limited by underpowered study designs.
IntroductionMechanical ventilation is a key element of respiratory support in critically ill patients with respiratory failure. In the early years of critical care, the one–single goal of mechanical ventilation was to provide sufficient gas exchange, often targeting physiological levels of arterial partial pressures of oxygen (paO2) and carbon dioxide (paCO2).1 In the last decades, the goals of ventilation shifted towards lung protection, even if this jeopardised the initial ventilatory targets (e.g. by applying permissive hypercapnia, to reduce tidal volume and plateau pressure).2 While so-called lung protective ventilation has become the standard of care,3 its application in clinical practice can be challenging and time consuming; achieving the ventilatory targets requires complex titrations of ventilator settings according to the individual needs of patients, which change over time. There is clearly no ‘one–size–fits–all’, and constant individualisation and titration of ventilatory settings are required mandating the use of sometimes complex bedside calculations. Currently, lung protective ventilation includes a low tidal volume (VT), to prevent volutrauma and barotraumas; low pressures and energy, to avoid energy trauma; and restricted oxygen, to minimise chemotrauma.
Automated, or closed loop modes of ventilation, are increasingly attractive for use in the ICU.4 Ventilator settings that are typically manually adjusted by the user during conventional ventilation can, once the targets are manually set, be controlled by the software during closed loop ventilation. Closed loop ventilation has the potential to optimise ventilator settings, to increase safety of ventilation, and even to improve patient outcomes.5,6 Closed loop ventilation might also reduce ICU nursing and medical staff workload, through immediate reaction to patients’ changing demands.7 This is particularly interesting when faced with increasing challenges due to shortages in ICU nursing staff,8 and especially in extreme situations as seen in the recent coronavirus disease 2019 (COVID-19) pandemic when large numbers of patients required invasive mechanical ventilation.
We present the results of a systematic search of the literature for publications on randomised clinical trials of closed loop ventilation that focused on effectiveness in providing lung protective ventilation and settings, safety, patient outcomes related efficacy and ICU staff workloads (Table 1). We hypothesised that currently available closed loop ventilation modes are effective, well tolerated and efficacious, while reducing the ICU staff workloads.
Table 1 - Definitions used for Outcome parameters Outcome parameters Definition Effectiveness The ability of the closed loop mode to institute appropriate settings as reflected by VT, ΔP, MP or FiO2, and to provide lung protective ventilation Safety Any adverse event, or discontinuation or change in a ventilator setting related to the closed loop mode under investigation because of unacceptable changes in clinical parameters Efficacy The effect of the closed loop mode on patient–related outcomes such as mortality, duration of ventilation, and ICU and hospital lengths of stay Workload The effect on staff workload such as the number of manual interventions to ventilator settings, or the number of alarmsWe conducted a literature search using various combinations of keywords and MeSH terms, including ‘Interactive Ventilatory Support’, ‘Respiration, Artificial’, ‘Automation’, ‘closed loop ventilation’, ‘automated ventilation’, ‘mechanical ventilation’ and ‘explicit computerized protocols’ in PubMed, Embase and the Cochrane Central register of Controlled Trials (CENTRAL). Inclusion criteria were randomised clinical trials that studied the effect of closed loop ventilation modes on ventilator settings, patient outcomes and ICU staff workload. We used no time or language restrictions, and included publications of studies in all patient categories, including paediatric and adult ICU cohorts. The reference lists of studies and systematic reviews identified by the search were used to find additional reports that may have been missed by the original search. The search was registered at PROSPERO with registration number CRD42023446174, and a final search was performed in January 2023.
Publications identified by the search were screened for eligibility by two independent investigators (RLG and LAB-K) by reading the titles and abstracts. If a study was considered potentially eligible, the full text was obtained, and reviewed for using the predefined inclusion and exclusion criteria.
Selection of studiesA publication was eligible if reporting on a randomised clinical trial of closed loop ventilation; in invasively ventilated paediatric or adult ICU patients; and reporting on aspects regarding effectiveness, safety, efficacy or workload.
We selected studies that tested either SmartCare (Dräger, Lübeck, Germany), Adaptive Support Ventilation (ASV) or INTELLiVENT–ASV (Hamilton Medical, Bonaduz, Switzerland), Neurally Adjusted Ventilatory Assist (NAVA) (Getinge, Goteborg, Sweden), Proportional Assist Ventilation Plus (PAV+) (Puritan Bennett, Minneapolis, USA) and Avea–CLiO2 (CareFusion, Yorba Linda, California, USA). For details on these closed loop modes, see Fig. 2.
We excluded reports on studies of noninvasive ventilation, and ventilation in another setting than the ICU, that is ventilation in an emergency department or in an operating room.
Extracted dataFrom each study, we collected the following data: patient characteristics, duration of ventilation or study intervention, and the investigated mode of closed loop and conventional ventilation. Data regarding effectiveness included ventilator settings and ventilation parameters such as tidal volume (VT), driving pressure (ΔP), mechanical power (MP) or fraction of inspired oxygen (FiO2). The rationale for choosing these effectiveness parameters in the light of closed loop ventilation and the current challenges in lung protective ventilation can be found in the Supplement, https://links.lww.com/EJA/A926. Data regarding safety included any adverse event, or discontinuation or change in a ventilator setting related to the closed loop mode under investigation because of unacceptable change in clinical parameters. Efficacy data included patient-related outcomes, such as duration of ventilation, length of stay in ICU or mortality rates. Data regarding workload included the number of manual interventions at the ventilator, or the number of alarms.
Risk of bias and study qualityFor each study, information was collected for the assessment of the risk of bias. The Cochrane Collaboration's tool for assessing risk of bias was used to assess the risk of bias for the included studies.9
We also calculated the fragility index for studies having a statistically significant dichotomous primary outcome,10,11 and compared them with the number of patients lost to follow-up for that endpoint in order to assess the robustness of the study results; the fragility index calculates the number of patients required to lose statistical significance.12
ReportingData were reported as medians with interquartile ranges or means with standard deviations. For each study that reported a dichotomous primary endpoint, the fragility index and the number of patients lost to follow-up were reported. We did not perform a meta-analysis of the studies identified by the search, because the studies used various outcome measures, and had different study designs and durations.
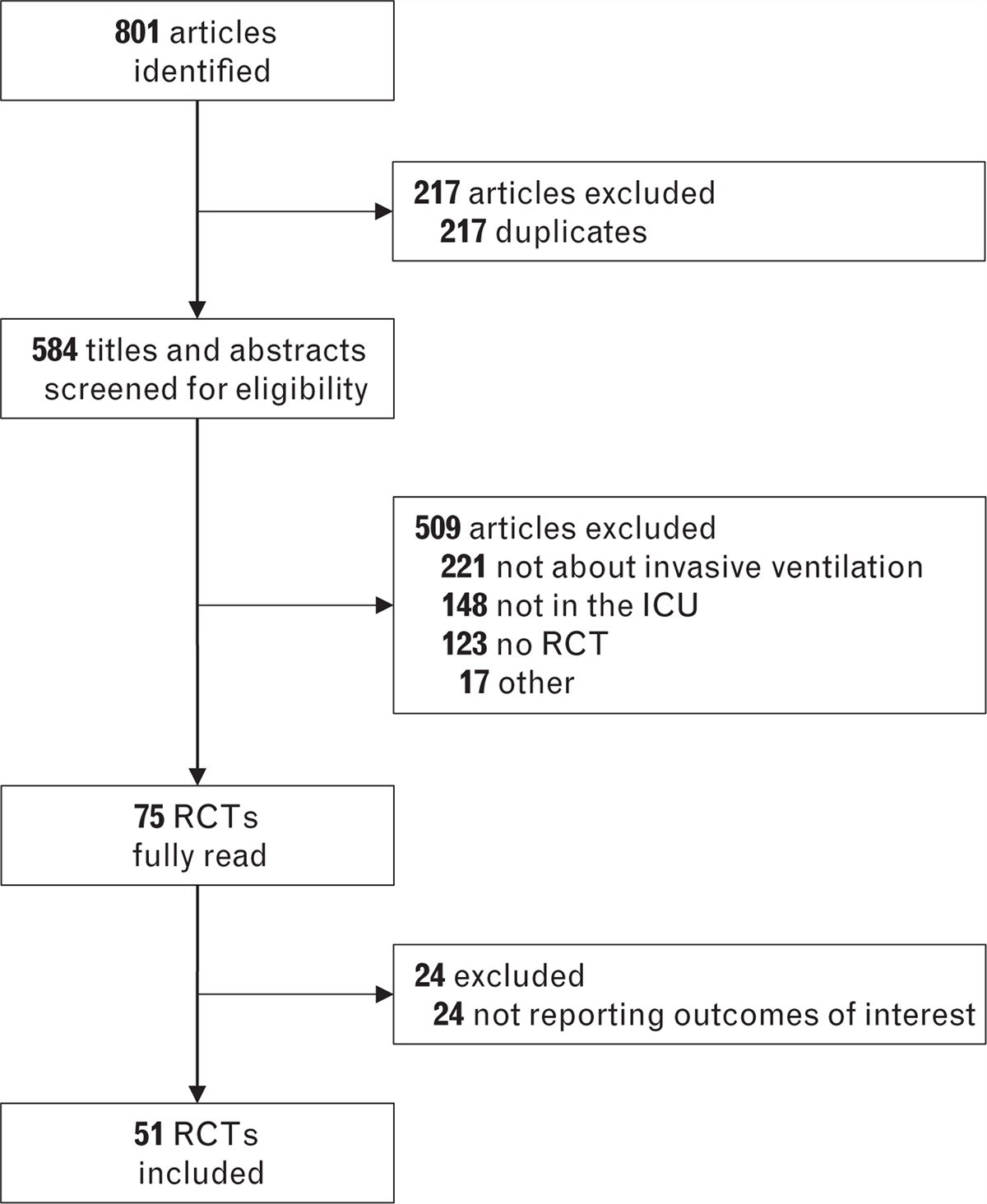
Results Search results and risk of biasThe search identified a total of 801 studies; after removal of duplicates and screening for eligibility, 45 studies in adult13–57 and six studies in paediatric patients58–63 were considered for this analysis (Fig. 1 and eTable S1, https://links.lww.com/EJA/A926). Thirty-five studies had a parallel randomised design13–19,21,23,25–31,33,34,36,38–40,43–57,62,63; 12 had a crossover randomised design.20,22,24,32,35,37,41,42,58–61 Only five studies were multicentre investigations.23,33,36,38,39 Most studies were performed in critically ill patients with respiratory failure15,16,18,22,24,26,27,29–31,33,35,36,39,41,46,47,54,62; twelve studies in patients after cardiac surgery13,17,25,28,34,48–51,57 or general surgery,20,23,43 four in difficult to wean patients,19,32,38,40,56 four in COPD patients14,21,44,45 and four in ARDS patients.37,42,53,55 Nine studies tested SmartCare,14,15,18,19,23,32,47,54,63 fourteen studies ASV,13,17,21,42,43,45,46,48–53,55 eight studies INTELLiVENT–ASV,22,24,25,27,28,30,34,35 eight studies NAVA,20,36–41,62 six studies PAV+,16,26,29,31,33,44 three studies Avea–CLiO258–60 and one closed loop FiO2 titrations during ASV.61 Observation duration differed substantially between studies (eTable S1, https://links.lww.com/EJA/A926).
 Fig. 1:
Fig. 1: Search results.
As blinding of personnel was not possible due to the nature of the intervention, risk of performance bias was high in all studies (eFigure S1, https://links.lww.com/EJA/A926). In most studies, it was unclear how detection bias was avoided. Allocation concealment was used in 24 studies to reduce the risk of selection bias. The fragility index could be calculated in five studies and varied between 0 and 18 (eTable S2, https://links.lww.com/EJA/A926,).
 Fig. 2:
Fig. 2: Closed loop ventilation modes.
EffectivenessWith SmartCare, VT decreased in difficult to wean patients32 but was not affected in critically ill patients47 compared with conventional ventilation (Table 2, Fig. 3 and eTable S3, https://links.lww.com/EJA/A926). With ASV, VT increased in cardiac surgery patients17 and in ARDS patients.42 ASV decreased VT in ARDS patients,55 but did not affect VT in cardiac surgery48,51 and COPD patients.21,47 INTELLiVENT-ASV led to a lower VT22,25,34 in cardiac surgery and unselected ICU patients, but VT increased24 or was unaffected in general ICU patients.27,30,35 With NAVA, VT decreased in ARDS patients.37 NAVA did not affect VT in abdominal surgery patients.20 PAV+ did not affect VT in a general ICU population.16,29,31
Table 2 - Effectiveness, safety, efficacy and workload with closed loop ventilation Author Year Ref Patients Closed loop mode tested Effectiveness Safety Efficacy Workload Jiang et al. 2006 14 38 COPD patients SmartCare – – ↑ ↑ Stahl et al. 2009 18 60 patients needed ventilation >24 h SmartCare – = ↑ = Ma et al. 2010 19 62 difficult to wean patients SmartCare ↑ – ↑ ↑ Rose et al. 2008 15 102 patients needed ventilation >24 h SmartCare – – = – Schädler et al. 2012 23 300 surgical patients needed ventilation >9 h SmartCare – – = – Burns et al. 2013 54 92 critically ill patients SmartCare – = ↑ – Jouvet et al. 2013 63 30 unselected paediatric patients SmartCare – = ↑ – Liu et al 2013 56 39 difficult to wean patients SmartCare – = ↑ – Taniguchi et al. 2015 47 70 critically ill patients SmartCare = = ↓ – Grieco et al. 2018 32 30 difficult to wean patients SmartCare ↑ – – – Sulzer et al. 2001 57 36 cardiac surgery patients Adaptive Support Ventilation – – ↑ – Petter et al. 2003 13 30 cardiac surgery patients Adaptive Support Ventilation – = = ↑ Dongelmans et al. 2009 17 128 cardiac surgery patients Adaptive Support Ventilation = – = – Kirakli et al. 2011 21 97 COPD patients Adaptive Support Ventilation = – ↑ – Agarwal et al. 2013 55 48 ARDS patients Adaptive Support Ventilation ↑ – = – Celli et al. 2014 43 20 abdominal surgery patients Adaptive Support Ventilation – – ↑ ↑ Mohamed et al. 2014 45 50 COPD patients Adaptive Support Ventilation – = ↑ – Kirakli et al. 2015 46 229 critically ill patients Adaptive Support Ventilation – – = ↑ Zhu et al. 2015 48 53 cardiac surgery patients Adaptive Support Ventilation = = ↑ – Yazdannik et al. 2016 49 64 cardiac surgery patients Adaptive Support Ventilation – – ↑ – Moradian et al. 2017 50 115 cardiac surgery patients Adaptive Support Ventilation – ↑ ↑ – Eremenko et al. 2020 51 78 cardiac surgery patients Adaptive Support Ventilation = = = ↑ Baedorf Kassis et al. 2022 42 20 ARDS patients Adaptive Support Ventilation = = – – Sehgal et al. 2022 52 48 envenomation patients Adaptive Support Ventilation – – = – Soydan et al. 2022 61 30 critically ill paediatric patients Adaptive Support Ventilation with closed–loop FiO2 titration ↑ ↑ – ↑ Zhang et al. 2022 53 100 ARDS patients Adaptive Support Ventilation – – ↑ – Arnal et al. 2012 22 50 critically ill patients INTELLiVENT–ASV ↑ = = – Clavieras et al. 2013 24 14 critically ill patients INTELLiVENT–ASV = – = – Lellouche et al. 2013 25 60 cardiac surgery patients INTELLiVENT–ASV ↑ – = ↑ Bialais et al. 2016 27 80 critically ill patients INTELLiVENT–ASV ↑ – = ↑ Fot et al. 2017 28 40 cardiac surgery patients INTELLiVENT–ASV = – = ↑ Arnal et al. 2018 30 60 critically ill patients INTELLiVENT–ASV = – = ↑ De Bie et al. 2020 34 220 cardiac surgery patients INTELLiVENT–ASV ↑ ↑ = – Chelly et al. 2022 35 265 critically ill patients INTELLiVENT–ASV = ↑ = ↑ Coisel et al. 2010 20 15 abdominal surgery patients Neurally–adjusted Ventilatory Assist ↑ ↓ – – Demoule et al. 2016 36 128 patients with ARF Neurally–adjusted Ventilatory Assist – – = – Diniz–Silva et al. 2020 37 20 ARDS patients Neurally–adjusted Ventilatory Assist = – – – Hadfield et al. 2020 38 72 difficult to wean patients Neurally–adjusted Ventilatory Assist – – ↑ – Liu et al. 2020 40 47 difficult to wean patients Neurally–adjusted Ventilatory Assist – – ↑ – Kacmarek et al. 2020 39 306 patients with ARF Neurally–adjusted Ventilatory Assist – ↑ ↑ – Cammarota et al. 2022 41 16 patients with AHRF Neurally–adjusted Ventilatory Assist = – – – Xirouchaki et al. 2008 16 208 critically ill patients Proportional Assist Ventilation+ = = – – Elganady et al. 2014 44 60 COPD patients Proportional Assist Ventilation+ – – ↑ – Kallio et al. 2015 62 170 critically ill paediatric patients Proportional Assist Ventilation+ – = = – Teixeira et al. 2015 26 160 patients needed controlled ventilation >24 h Proportional Assist Ventilation+ – – = – Bosma et al. 2016 29 50 patients needed ventilation >36 h Proportional Assist Ventilation+ = =
留言 (0)