BACKGROUND
Neuraxial labour analgesia can be initiated with epidural (EPL), combined spinal epidural (CSE) or dural puncture epidural (DPE) and maintained with continuous epidural infusion (CEI), patient-controlled epidural analgesia (PCEA) or programmed intermittent epidural bolus (PIEB), but the optimal analgesia modality is still controversial.
OBJECTIVE
To compare the effects of commonly used neuraxial analgesia modalities on the proportion of women needing physician interventions, as defined by the need for physician-administered epidural top-ups for inadequate analgesia in labour.
DESIGN
Bayesian network meta-analysis.
DATA SOURCES
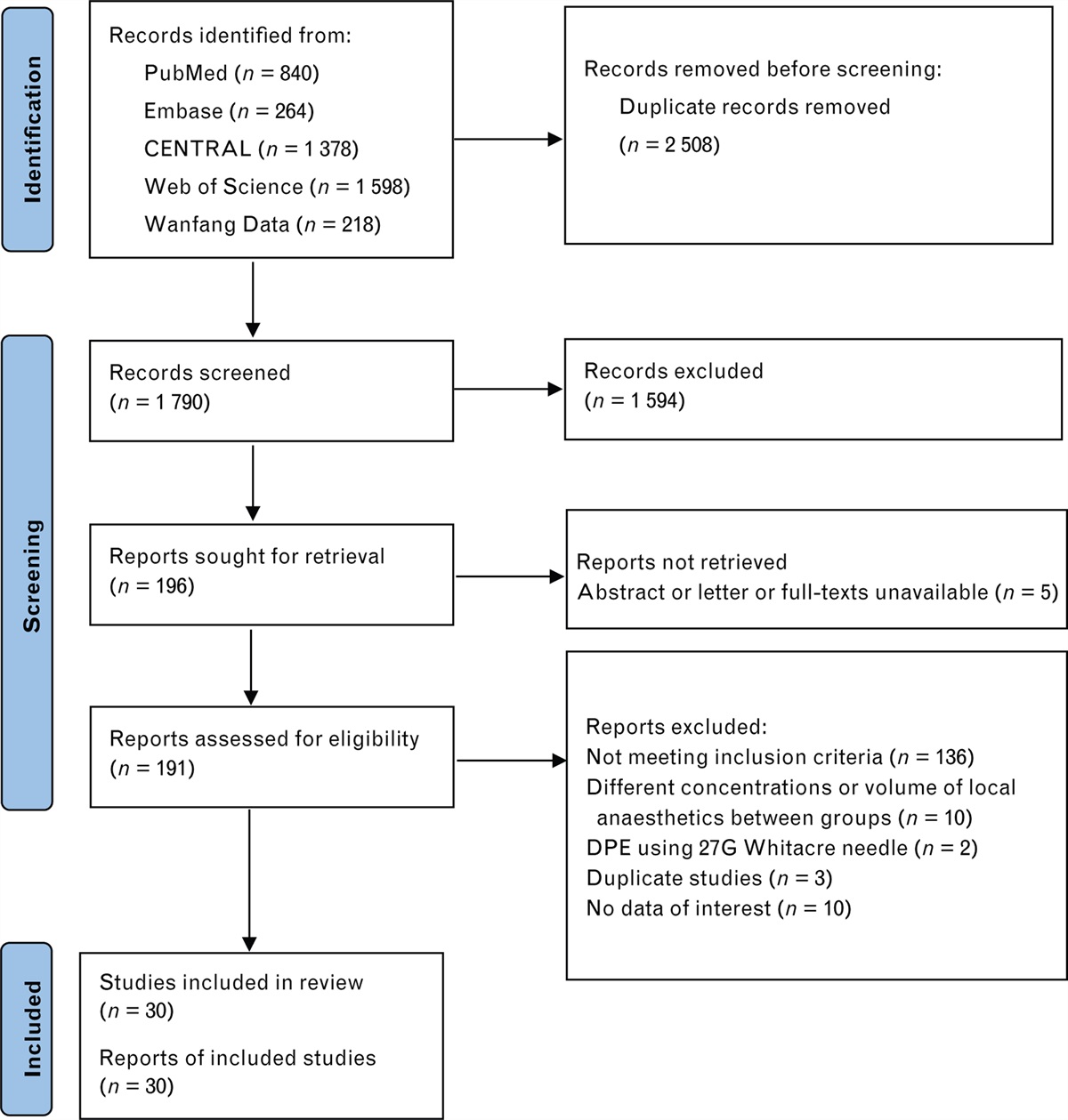
PubMed, Embase, CENTRAL, Web of Science and Wanfang Data were searched from January 1988 to August 2023 without language restriction.
ELIGIBILITY CRITERIA
Randomised controlled trials comparing two or more modalities of the following six neuraxial analgesia modalities in healthy labouring women: EPL+CEI+PCEA, EPL+PIEB+PCEA, CSE+CEI+PCEA, CSE+PIEB+PCEA, DPE+CEI+PCEA and DPE+PIEB+PCEA.
RESULTS
Thirty studies with 8188 women were included. Compared with EPL+CEI+PCEA, EPL+PIEB+PCEA [odds ratio (OR) = 0.44; 95% credible interval (CrI), 0.22 to 0.86], CSE+PIEB+PCEA (OR = 0.29; 95% CrI, 0.12 to 0.71) and DPE+PIEB+PCEA (OR = 0.19; 95% CrI, 0.08 to 0.42) significantly reduced the proportion of women needing physician interventions. DPE+PIEB+PCEA had fewer women needing physician interventions than all other modalities, except for CSE+PIEB+PCEA (OR = 0.63; 95% CrI, 0.25 to 1.62). There were no significant differences in local anaesthetic consumption, maximum pain score, and the incidence of instrumental delivery between the different neuraxial modalities.
CONCLUSIONS
PIEB+PCEA is associated with a lower risk of physician interventions in labour than CEI+PCEA. DPE or CSE and PIEB+PCEA may be associated with a lower likelihood of physician interventions than other neuraxial modalities. Otherwise, the new neuraxial analgesia techniques do not appear to offer significant advantages over traditional techniques. However, these results should be interpreted with caution due to limited data and methodological limitations.
TRIAL REGISTRATION
PROSPERO (CRD42023402540).


留言 (0)