Clinically relevant endpoints are important for the evaluation of outcomes of patients treated for chronic GVHD. The primary endpoint, treatment success at 6 months was observed for 55.9% of the study patients with 6 more patients (17.6%) receiving secondary treatment between months 6 and month 12. For comparison, in the randomized phase II/III study evaluating efficacy of prednisone (PDN) and sirolimus (SRL) vs. PDN, SRL, and CNI in 138 patients with cGVHD [20] the primary endpoint was the proportion of patients being alive with CR or PR and without relapse or secondary therapy at month 6. In that study, which included about 20% patients with mild cGVHD, rate of treatment success was 48.6% (PDN/SRL) and 50.0% (PDN/SRL/CNI) at month 6. Like in our study, about 20–30% of patients receiving PDN/SRL and 11–24% receiving PDN/SRL/CNI received secondary treatment between month 6 and month 12. Recently, a prospective randomized trial reported a 6-months overall response and CR rates of 53 and 32% for patients treated with itacinib (400 mg qd) + steroids compared to 35 and 18% for steroids alone. The improvement in response rate, however, came at the expense of a higher risk of relapse of underlying malignancy and overall mortality [7].
In another study, Inamoto et al. used a novel composite endpoint, i.e., FFS which was defined as absence of second-line treatment, non-relapse mortality, and recurrent malignancy. This endpoint differs from the primary endpoint defined in our study, as it did not directly address treatment response (CR/PR) and furthermore, there was no direct predefined procedure to handle disease progression, in terms of second-line treatment initiation. The FFS rate was 68% after 6 months and 54% after 12 months, respectively [21].
Another study included a cohort of 328 patients that were enrolled within 3 months after diagnosis of cGVHD [22]. Patients received initial treatment for cGVHD including PRD with or without CNI (58%), PRD with or without CNI and other agents (29%), and other agents without PRD (13%). The study aimed to narrow down an endpoint that is associated with clinical benefit after initial treatment of cGVHD. They found that CR or PR at 1 year without secondary systemic treatment provides clinical benefit in patients with cGVHD. However, success as defined by that novel endpoint was reported to be currently observed for less than 20% of patients with cGVHD. Furthermore, conclusions made from results obtained at 6 months were found in that study to be less striking, especially as about 45–55% of the patients in that study received secondary systemic treatment between 6 months and 1 year [22].
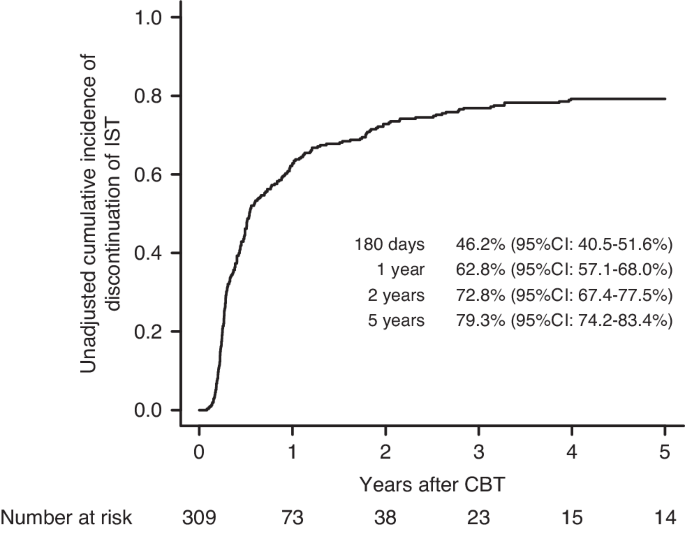
Thus, the significance of the primary endpoint in this study might also be limited by the time point (month 6) for assessing treatment success. However, one of the secondary endpoints of this study was to access the time to treatment failure. At 1 year, treatment failure was observed in 63% of the patients indicating a treatment success rate of 37%, which appears to be higher than reported by Martin et al. (less than 20%).
Concerning the overall survival (OS) rate of patients treated with PDN and everolimus in our study, 78% of the patients were alive at 2 years. For comparison, Carpenter et al. observed OS rates at 2 years of 81.5% for PRD/SRL and 74% with PRD/SRL/CNI, respectively [20]. Similar rates were also observed by Martin et al., who reported survival rates of 87% of the patients in the control arm and 74% in the MMF arm, respectively [6].
Regarding relapse rate of underlying malignancies, 5.9% of the patients in our study experienced a relapse until study completion. These values are similar to results observed in other studies in which values of about 10–20% (81/400 and 32/328) of patients with recurrent diseases after 12 months were observed [7, 21, 22].
Regarding other safety aspects, incidence rates of the predefined safety endpoints TMA, NIP, and avascular osteonecrosis were low. In our study none of the patients experienced TMA. This is quite similar to low proportions observed in other studies that range from about 1% to about 5% [11, 20]. Likewise, no patients developed NIP. NIP is a known side effect of SRL and everolimus and values reported in literature show broad range of about 1% up to about 17% probably depending on target serum level and concomitant medication e.g., with CNI [20, 23,24,25,26].
Corticosteroids are considered a risk factor for the development of avascular osteonecrosis (AVN). None of the patients in this study showed AVN. Incidence rates reported in literature range from about 2 to 10% [27, 28]. The study published by McAvoy et al. investigated the corticosteroid dose dependent risk for avascular osteonecrosis risk; it revealed a 4.0 to 8.6 fold cumulative prednisone dose-dependent increased risk for patients receiving PDN [28]. Of note, in that study the median time from HCT to AVN was 15 (4–41) to 21 (1–80) months. Thus, significance of values observed in our study might be limited by the shorter time of observation.
Overall, despite the differences in the concrete definition of endpoints and the time point for assessing the (primary) endpoint(s) between the various studies, our data do not demonstrate beneficial effects from addition of everolimus to the first-line prednisone treatment regimen in terms of improvement of the primary endpoint (treatment success at 6 months). Addition of everolimus to prednisolone did not increase risk of relapse of underlying malignancy and was not associated with an increased risk of other side effects such as TMA and NIP or AVN. Notably the rate of treatment failure at 1 year was 63%, meaning 37% rate of treatment success, which appears higher than previously reported rates [22]. This is of particular importance because this endpoint is associated with clinical benefit [22]. Everolimus has a shorter terminal half-life of 28 h compared to 62 h for sirolimus and less toxic effects when combined with CNIs [29]. Furthermore, everolimus seems more effective in inhibiting class-I-stimulated mTORC2 [30], it is however unknown, whether this would have impact on treatment of GVHD. Larger randomized studies with even longer follow-up may help ascertain the role of everolimus in first-line treatment of cGVHD.






留言 (0)