
記住我







Fortunately, dramatic improvements in the care of people with HIV (PWH) continue to occur at an astonishing rate [1,2]. Most PWH on treatment in the United States will live a similar life expectancy compared to people without HIV. Yet many PWH still have HIV-related problems and immune recovery is often suboptimal (see video abstract, https://links.lww.com/QAD/D115) [1]. Most patients have persistent inflammation and clinical consequences. Historically, experienced providers caring for PWH patients were particularly adept at recognizing clinical stumbling blocks common for PWH while in care. These include drug interactions, certain virally associated cancers, and osteoporosis among many other topics. Currently, as HIV care continues to stream-line, minimal monitoring is recommended, specifically, less intense monitoring of the CD4+ cells and CD4+/CD8+ cell ratio than in the past (Table 1). Distinguishing between a virally suppressed patient with an impaired immune system, and one whose immune system is closer to that of a person who never had an HIV infection is less straightforward than it used to be [3]. So interdisciplinary teams of specialists familiar with HIV-specific syndromes are still needed. This may include neurologists familiar with HIV-associated neurologic disease (HAND) [4] and colorectal surgeons familiar with monitoring for anal cancer. Here we present our view on HIV immune dysfunction while on ART and how monitoring the CD4+/CD8+ cell ratio may alter care not only delivered by HIV specialists but also the rest of the care team.
Table 1 - Immune recovery monitoring guidelines for people with HIV on antiretroviral therapy. Publishing organization Immune recovery monitoring recommendations Publication year Access date European AIDS Clinical Society [9] CD4+/CD8+ cell ratio = stronger predictor of serious outcomesA hallmark of HIV early in the pandemic was not just CD4+ cell loss but also an inversion of the CD4+/CD8+ cell ratio [5]. Debate raged over what aspect of the immune alteration was most important. However, once the virus was discovered and determined to have CD4+ as a receptor, the biology seemed clearer [6]. End-stage patients often had general lymphopenia with few T cells and ratio discussions faded. Once viral suppression could be reliably achieved, it became clear that antiretroviral therapy often normalized, or nearly normalized, the CD4+ cell count. However, normalization of the CD4+/CD8+ cell ratio can take longer or is often never achieved [1,7]. The main value of the CD4+ cell count in the past was two-fold:
1. decide when to discontinue prophylaxis for opportunistic infections 2. reassure the patient that their immune system was ‘recovering’.Neither of which is a common need for current patients. Currently, two opposing perspectives can be found within the immune recovery monitoring guidelines (Table 1). Most guidelines recommend limited or no immune monitoring once viral suppression/immune recovery has been achieved on ART. Alternatively, a few guidelines not only recommend continued immune recovery monitoring but also discuss its significance in predicting serious outcomes or immune status. Some recognize that the CD4+/CD8+ cell ratio is more informative than CD4+ cell count alone including the CD4+ cell nadir, which is not always available. One avenue for potential biomarker discovery of virus-related immune injury and inflammatory disease progression currently being assessed is proteomics. This was notably studied in the context of the variety of outcomes in COVID-19 patients [8], At this time, however, proteomics and other ‘omic’ approaches are neither validated in multiple studies, nor available to frontline clinics, whereas the CD4+/CD8+ cell ratio is.
Clinical laboratories use flow cytometers for many things, not only for HIV but also for cancer. Not that long ago multicolor flow cytometry was rare in resource-limited settings but is now more available [20]. Many institutions will run anti-CD3/4 and 8 even if only a CD4+ cell count is ordered simply because it enhances quality control (the number of CD3+/CD4+ cells + the number of CD3+/CD8+ cells should roughly equal the number of CD3+ cells). The cost of anti-CD8+ antibodies is small relative to phlebotomy, technician time, and machine maintenance costs and other factors. Costs in healthcare are notoriously opaque but the care provided to patients should not be.
What is a complete immune recovery?It remains unknown if a specific patient's complete immune recovery from HIV occurs or is even possible [3]. All infections leave a ‘memory’ or ‘scar,’ but the reshaping of the immune system by HIV is particularly profound. Even after ART has achieved sustained viral suppression, the extent of immune recovery is highly variable and often incomplete [1,7]. If a PWH achieves a normal CD4+/CD8+ cell ratio, there are likely persistent alterations in gamma/delta T cells and other innate lymphocyte populations [21]. Although in general, PWH that are virally suppressed can respond to vaccines and have relatively few complications, there remains demonstrable weaker immune responses to some vaccines when the CD4+/CD8+ cell ratio is less than 1.0 (discussed later). A normalized CD4+/CD8+ cell ratio does not mean a PWH has an immune system equivalent to that of a person who never acquired HIV. However, a normalized ratio can indicate that cancer risk and overall immune response are much closer to a person who never acquired HIV compared with a PWH who has a CD4+/CD8+ cell ratio below 1.03. Data suggests that the ratio is also likely a marker for suboptimal adaptive immunity in people without HIV, although longitudinal immune counts are less available in the non-HIV population [22,23]. A low CD4+/CD8+ cell ratio can result from either too few CD4+ cells, to high CD8+ cells or some combination. Each of these scenarios may implicate effect on antigen immune response and/or sustained immune activation. As CD4+ cell count recovers/normalizes, the CD8+ cell count may drive the resultant ratio value [24,25]. The ratio, however, incorporates both factors, is better studied and more commonly used than CD8+ cell counts in isolation. It is important to note that studies in mice suggest the ‘normal role’ of the thymus is to ensure a numerical advantage of CD4+ cells over CD8+ cells [26]. Obviously, some studies use slightly different cut offs (anywhere from 0.4–1.0), but multiple cut offs demonstrable clinical consequences to not achieving a more ‘normal’ CD4+/CD8+ cell ratio.
There is data demonstrating CD4+/CD8+ cell ratio as an imperfect but potential marker of HIV reservoir. This data can be found in a comprehensive, recent review that focuses on how the CD4+/CD8+ cell ratio could factor into research on gut dysbiosis, generalized inflammation, and ART-free remission [27]. Efforts to reduce the HIV reservoir do not yet influence guideline-based standards of care and will not be discussed further here, but are reviewed in Ron et al. in 2023 [27]. Practicing HIV providers realize that viral suppression is not always a consistent ‘once achieved never threatened’ phenomenon. One advantage of the CD4+/CD8+ cell ratio is that demonstration of a decline or a slower recovery can serve as a clue of intermittent inadequate suppression over time [28]. Some feel that monitoring the ratio is not useful as actions to improve the ratio are limited. There is evidence though that exercise improves the ratio [29]. Obviously, most of us would benefit from more exercise, but for select patients, educating them that their immune recovery is suboptimal, and exercise may improve immune recovery could be motivating.
Linkage of CD4+/CD8+ cell ratio and vaccine responsiveness and immune protectionImmune recovery can impact responsiveness to vaccinations. In many studies, PWH can exhibit lower rates of immune response to various vaccinations, which can be further exacerbated by lower CD4+ cells [30–34]. However, these lower rates of immunological responses may not solely be attributed to lower CD4+ cells as other studies have shown that even in the setting of elevated CD4+ cells, immunological response after vaccination can be decreased [35].
In a study focusing on PWH's serological response to the HBV vaccination, a CD4+/CD8+ cell ratio of greater than 0.4 was shown to be a better predictor of immune responsiveness to the HBV vaccine compared with CD4+ cell count alone, despite analyzing various CD4+ cell thresholds [36]. In another study focusing on PWH's immune response to BNT162b2 (BioNTech, Pfizer) COVID-19 vaccine, individuals with a CD4+/CD8+ cell ratio greater than 0.5 had a significantly higher serological immune response (higher anti-S IgG and neutralizing antibodies) after priming compared with individuals with CD4+/CD8+ cell ratio 0.5 or less. Interestingly though, there was no significant difference in immune serologic levels after BNT162b2 priming when comparing persons with CD4+ cell count above and below 500 [37]. This discordance was also shown in a study focusing on Yellow Fever vaccination-induced antibody titers in 34 PWH treated with ART, which exhibited lower antibody titers with lower CD4+/CD8+ cell ratios (P = 0.014) but not with lower CD4+ levels (P = 0.52) [38]. Currently providers often vaccinate newly diagnosed HIV-infected patients with, for example, hepatitis B vaccine as soon as possible after starting ART even if their CD4+ T-cell count is less than 200 [39], but a reasonable interpretation of current data might consider waiting in select individuals a few months until the CD4+/CD8+ cell ratio rises above 0.4 to achieve better immune responsiveness to vaccination [36]. Future studies should eventually address this dilemma in a head-to-head comparison.
Additional evidence that the CD4+/CD8+ cell ratio is related to immunologic competence to protect against infectious disease occurs outside the vaccination arena. A retrospective study in Ethiopia demonstrated that PWH who are on ART but have relatively poor normalization of their CD4+/CD8+ cell ratio have a higher likelihood of acquiring tuberculosis [7]. Additionally, in the Aquitainte Cohort, a ratio less than 0.8 was associated with severe bacterial infections [40]. Historically, we have worried about opportunistic infections in PWH, but in the current era, other outcomes maybe more relevant. Serious non-AIDS events such as cancer, renal disease, cardiovascular, and cerebrovascular events are worth tracking and many may correlate with lower ratios [41].
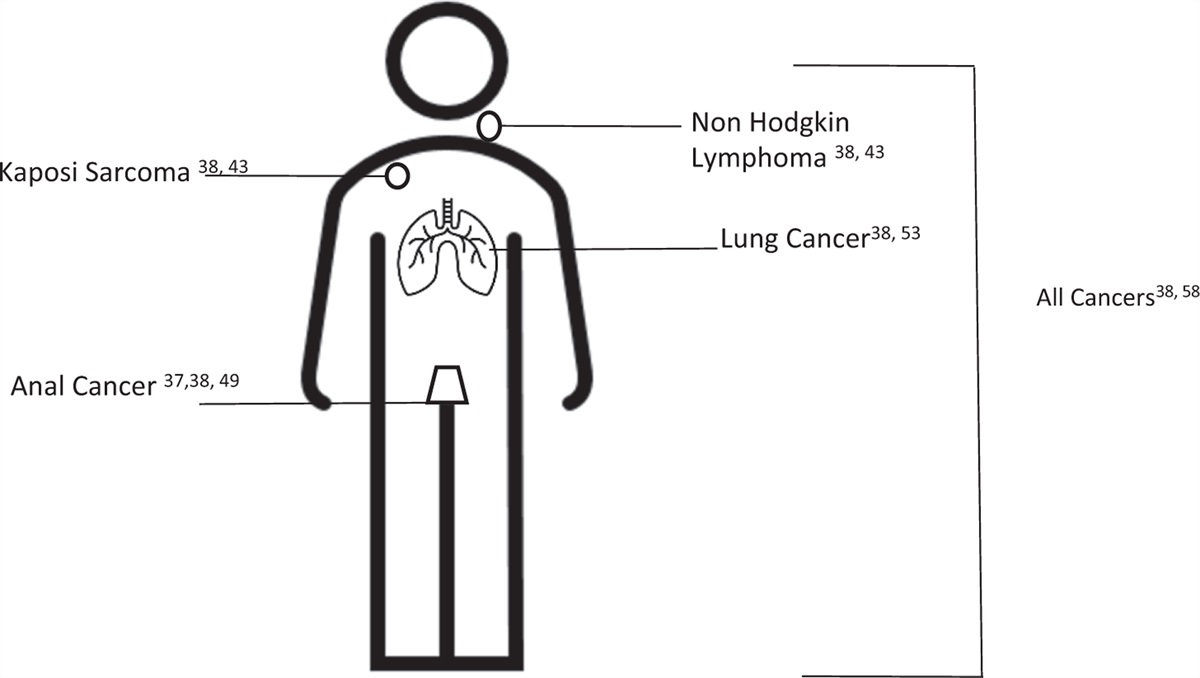
Role of immune recovery in cancer monitoringPerhaps the most important current and clinically relevant reason to monitor the CD4+/CD8+ cell ratio is cancer screening. Although age is the traditional factor in determining cancer screening, several factors such as family history, smoking and other risk factors, perhaps including the CD4+/CD8+ cell ratio should also contribute to the decision particularly in the age of ‘precision medicine’ [42]. All types of cancer are more common in PWH than those without, and it turns out much of this risk is likely assessed by the CD4+/CD8+ cell ratio (see Fig. 1) [43]. Additional markers of cancer in PWH on bulk T cells include ‘exhaustion markers’ such as PD-1 [44]. These markers, however, are not generally available in clinical practice today. Although the cancer susceptibility of low CD4+/CD8+ cell ratio individuals is particularly pronounced in PWH, it is interestingly not unique to PWH. A low CD4+/CD8+ cell ratio in MSM who do not have HIV is associated with increased susceptibility to certain cancers such as anal, virally associated lymphomas, and liver cancer [45].
 Fig. 1:
Fig. 1: Location of cancers in people with HIV associated with low CD4+/CD8+ cell ratio.
Virally associated cancersChronic infections in addition to HIV (most notably hepatitis B virus and cytomegalovirus) [46] can drive the ratio lower. In the case of hepatitis B, the degree of ratio lowering correlated with hepatitis B viremia [47]. The relationships between cancer and the ratio are complex though as other factors, including liver damage from alcohol can contribute to liver cancer development. Therefore, the CD4+/CD8+ cell ratio may have little meaning in predicting liver cancer. The same lack of association may hold true for head and neck cancer which is often HPV-associated [43]. For cancers associated with Kaposi sarcoma, Herpes virus [43,48] and Epstein–Barr virus-associated lymphoma [49], there does seem to be a relationship between the ratio and virally associated cancer [43].
Anal cancer screeningThe incidence of anal cancer has been increasing for the past decade and disproportionately affects certain at-risk groups, including PWH [50–53]. The results of the recently completed ANCHOR trial demonstrate a nearly 60% reduction in anal cancer in PWH when their anal high-grade squamous intraepithelial lesions (HSIL) were treated compared with monitoring alone [52]. These results highlight a critical need to identify and treat anal dysplasia to prevent progression to anal cancer.
Currently, there are no evidenced-based recommendations to guide anal cancer screening or surveillance, which can be invasive and potentially distressing to patients [51,52,54–57]. Notwithstanding, many experts recommend routine screening in high-risk populations, such as PWH [58]. Screening measures involve some combination of digital rectal examinations, anal cytology with or without HPV testing, and high-resolution anoscopy [50,52,55–57,59]. Each of these screening modalities has limitations. Accordingly, further research into clinically useful, objective markers is needed to increase the precision of risk estimates in identifying anal HSIL, as this has the potential to improve screening algorithms by reducing unneeded burdensome examinations.
The CD4+/CD8+ cell ratio is a promising immunologic marker for stratifying which patients to screen and individualizing surveillance intervals. Lower ratios have been associated with increased rates of anal cancer, which has now been extensively validated in multiple populations [43,51,54]. A shared decision-making approach to anal cancer screenings has been advocated based on risk factors [55]. If such an approach is used, certainly one of the most well validated risk factors is the CD4+/CD8+ cell ratio (both the nadir as well as the nearest ratio value). Many anal cancer screening and surveillance protocols suggest ranges for time intervals between exams/treatments [58,60]. Consequently, anal screening and surveillance should be at more aggressive intervals in PWH with low ratios as both the current ratio, as well as duration below a threshold, indicates increased risk of anal cancer when compared with those with higher ratios [51,61]. Notably, while fully suppressive antiretroviral therapy allows ratio normalization in some, it does not do this universally and immune recovery as assessed by normalized CD4+ cell counts alone, is not associated with decreased risk of anal neoplasia [54,62,63].
Nonvirally associated cancerThe strongest evidence of the link between cancer risk and CD4+/CD8+ cell ratio comes from a retrospective analysis of the large, longitudinal database North American AIDS Cohort Collaboration on Research and Design (NA-ACCORD) [43] This study examined individuals 18 years and older and established that the CD4+/CD8+ cell ratio association with cancer (all forms) was independent of age, sex, CD4+ cell count, HIV viral load, hepatitis C viral infection and smoking history. For both individual cancers and all cancers, hazard ratios were calculated comparing both a ratio 0.3 or less vs. 0.8 or less, as well as 0.5 or less vs. 0.8 or less. In both cases, lower ratios were associated with increased cancer risk with a P value of less than 0.001. In addition to lung cancer, as an example of nonvirally associated cancer linked to the ratio, colorectal cancer, was also associated with a low ratio but only when the 0.5 cutoff was used [43]
An important question is whether cancer causes the low CD4+/CD8+ cell ratio or the low CD4+/CD8+ cell ratio increases cancer susceptibility. Data suggests a low CD4+/CD8+ cell ratio precedes cancer development by up to 24 months. When the authors broke down which cancers were most likely associated with a low ratio, they found three of the highest mortality and most common cancers in PWH (anal cancer, NHL, and lung cancer) were the most strongly associated with a low ratio [43]. Precancerous anal lesions as well as cancer were found to associated with not just the degree of ratio suppression but also the duration of time below 0.5 [61]. Important to note, this and most data on ratios and PWH is heavily dominated by data from MSM, and it is important to examine data from women as well. However, the data from Ethiopia does suggest similar effects are occurring between men and women, and the effect could be stronger in women as they tend to recover to a higher CD4+/CD8+ cell ratio [7].
Lung cancerInterestingly, some cancers that are not thought to be associated with chronic infections are still associated with low ratios in PWH. The best studied, and in some ways, most surprising is lung cancer. Several studies in both PWH and patients not living with HIV suggest smoking can raise the CD4+/CD8+ cell ratio in some individuals [1,64]. In a large study of 21 666 American veterans living with HIV, a low ratio and pneumonia often preceded the development of lung cancer even after controlling for such factors as smoking and occupational risk [65]. The association of lung cancer with a low ratio is also seen in civilian cohorts [43,66].
In conclusion, care for PWH continues to evolve rapidly. CD4+/CD8+ cell ratios have shown to be a better predictor of immune recovery in regards to vaccine response and immune-mediated cancer susceptibility, compared to CD4+ cell count alone. Certainly, additional studies linking ratios to clinical events are needed particularly in endemic areas such as Africa, in women living with HIV, and in people infected with HIV2 or both HIV1/2. These factors may strengthen the ratio biomarker utility (or not) because of the slower response of CD4+ cells to therapy [67]. Recently the concept of ‘immune resilience’ calculated by both the ratio and numerical criteria for CD4+ cells was found to correlate with clinical outcomes in many non-HIV cohorts [22]. In conclusion, CD4+/CD8+ cell ratios are an important biomarker to help guide patient-specific clinical care in PWH. Lab costs and locoregional policies will likely play a role in specific laboratory monitoring, however, overly strict reliance on guidelines to modify monitoring plans are likely not justified with current and emerging data on the benefits of CD4+/CD8+ risk prediction.
AcknowledgementsThe authors would like to thank Mary Stella Praise for helpful suggestions, and perspective from an experienced HIV provider, as well as the UW Madison Department of Family Medicine LGTBQ fellowship (to M.G.) and T32 surgical oncology fellowship (NIH, NIC T32CA090217) (to A.H.).
Written work prepared by employees of the Federal Government as part of their official duties is, under the US Copyright Act, a ‘work of the United States Government’ for which copyright protection under Title 17 of the United States Code is not available. As such, copyright does not extend to the contributions of employees of the Federal Government (C.B.S.). We want to acknowledge UW Madison Department of Family Medicine LGTBQ fellowship (to M.G.) and T32 surgical oncology fellowship (NIH, NIC T32CA090217) (to A.H.).
Conflicts of interestThere are no conflicts of interest.
References 1. Mutoh Y, Nishijima T, Inaba Y, Tanaka N, Kikuchi Y, Gatanaga H, Oka S. Incomplete recovery of CD4 cell count, CD4 percentage, and CD4/CD8 ratio in patients with human immunodeficiency virus infection and suppressed viremia during long-term antiretroviral therapy. Clin Infect Dis 2018; 67:927–933. 2. Bloch M, John M, Smith D, Rasmussen TA, Wright E. Managing HIV-associated inflammation and ageing in the era of modern ART. HIV Med 2020; 21: (Suppl 3): 2–16. 3. Serrano-Villar S, Sainz T, Lee SA, Hunt PW, Sinclair E, Shacklett BL, et al. HIV-infected individuals with low CD4/CD8 ratio despite effective antiretroviral therapy exhibit altered T cell subsets, heightened CD8+ T cell activation, and increased risk of non-AIDS morbidity and mortality. PLoS Pathog 2014; 10:e1004078. 4. Vassallo M, Fabre R, Durant J, Lebrun-Frenay C, Joly H, Ticchioni M, et al. A decreasing CD4/CD8 ratio over time and lower CSF-penetrating antiretroviral regimens are associated with a higher risk of neurocognitive deterioration, independently of viral replication. J Neurovirol 2017; 23:216–225. 5. Bofill M, Janossy G, Lee CA, McDonell-Burns D, Phillips AN, Sabin C, et al. Laboratory control values for CD4 and CD8 T lymphocytes. Implications for HIV-1 diagnosis. Clin Exp Immunol 1992; 88:243–252. 6. Sattentau QJ, Weiss RA. The CD4 antigen: physiological ligand and HIV receptor. Cell 1988; 52:631–633. 7. Wolday D, Kebede Y, Legesse D, Siraj DS, McBride JA, Kirsch MJ, Striker R. Role of CD4/CD8 ratio on the incidence of tuberculosis in HIV-infected patients on antiretroviral therapy followed up for more than a decade. PLoS One 2020; 15:e0233049. 8. Patel H, Ashton NJ, Dobson RJB, Andersson LM, Yilmaz A, Blennow K, et al. Proteomic blood profiling in mild, severe and critical COVID-19 patients. Sci Rep 2021; 11:6357. 9. Ryom L, De Miguel R, Cotter AG, Podlekareva D, Beguelin C, Waalewijn H, et al. EACS Governing Board. Major revision version 11.0 of the European AIDS Clinical Society Guidelines 2021. HIV Med 2022; 23:849–858. 10. AIDS and Hepatitis C Professional Group. Society of Infectious Diseases, Chinese Medical Association & Chinese Center for Disease Control and Prevention [Chinese guidelines for diagnosis and treatment of HIV/AIDS (2021 edition)]. Zhonghua Nei Ke Za Zhi 2021; 60:1106–1128. 11. Thompson MA, Horberg MA, Agwu AL, Colasanti JA, Jain MK, Short WR, et al. Primary care guidance for persons with human immunodeficiency virus: 2020 update by the HIV Medicine Association of the Infectious Diseases Society of America. Clin Infect Dis 2021; 73:e3572–e3605. 12. Antiretroviral Guidelines US DHHS Guidelines with Australian commentary. 13. Primary Care of Veterans with HIV (2019). 14. National Guidelines for Prevention and Management of HIV and STIs. Edition 2016 (2016). 15. The Korean Society for AIDS. Summary of 2021 Clinical Guidelines for the Diagnosis and Treatment of HIV/AIDS in HIV-infected Koreans. Infect Chemother 2021; 53:592–616. 16. 2019 ART Clinical Guidelines for the Management of HIV in Adults, Pregnancy, Adolescents, Children, Infants and Neonates (2019). 17. National Guidelines for HIV Care and Treatment 2021 (2021). 18. National Guidelines for HIV Prevention, Treatment and Care (2020). 19. National Guidelines for Comprehensive HIV Prevention, Care and Treatment (2017). 20. Marinucci F, Medina-Moreno S, Paterniti AD, Wattleworth M, Redfield RR. Decentralization of CD4 testing in resource-limited settings: 7 years of experience in six African countries. Cytometry A 2011; 79A:368–374. 21. Pauza CD, Poonia B, Li H, Cairo C, Chaudhry S. γδ T cells in HIV disease: past, present, and future. Front Immunol 2015; 5:687. 22. Ahuja SK, Manoharan MS, Lee GC, McKinnon LR, Meunier JA, Steri M, et al. Immune resilience despite inflammatory stress promotes longevity and favorable health outcomes including resistance to infection. Nat Commun 2023; 14:3286. 23. Idiopathic CD4 Lymphocytopenia at 30, Years. N Engl J Med 2023; 389:674–676. 24. Helleberg M, Kronborg G, Ullum H, Ryder LP, Obel N, Gerstoft J. Course and clinical significance of CD8+ T-cell counts in a large cohort of HIV-infected individuals. J Infect Dis 2015; 211:1726–1734. 25. Chammartin F, Darling K, Abela IA, Battegay M, Furrer H, Calmy A, et al. CD4:CD8 ratio and CD8 cell count and their prognostic relevance for coronary heart disease events and stroke in antiretroviral treated individuals: the Swiss HIV Cohort Study. J Acquir Immune Defic Syndr 1999 2022; 91:508–515. 26. Sinclair C, Bains I, Yates AJ, Seddon B. Asymmetric thymocyte death underlies the CD4:CD8 T-cell ratio in the adaptive immune system. Proc Natl Acad Sci USA 2013; 110:E2905–E2914. 27. Ron R, Moreno E, Martínez-Sanz J, Brañas F, Sainz T, Moreno S, Serrano-Villar S. CD4/CD8 ratio during human immunodeficiency virus (HIV) treatment: time for routine monitoring?. Clin Infect Dis 2023; 76:1688–1696. 28. Belaunzarán-Zamudio PF, Naranjo L, Caro-Vega Y, Castillo-Mancilla JR, Camiro-Zuñiga A, Fuentes-García R, et al. Incomplete antiretroviral therapy adherence is associated with lower CD4-CD8 ratio in virally suppressed patients with HIV infection in Mexico. AIDS Res Hum Retroviruses 2023; 39:136–144. 29. Bernal E, Bernal E, Martinez M, Campillo JA, Puche G, Baguena C, et al. Moderate to intense physical activity is associated with improved clinical, CD4/CD8 ratio, and immune activation status in HIV-infected patients on ART. Open Forum Infect Dis 2022; 9:ofab654. 30. French N, Gordon SB, Mwalukomo T, White SA, Mwafulirwa G, Longwe H, et al. A trial of 7-valent pneumococcal conjugate vaccine in HIV-infected adults. N Engl J Med 2010; 362:812–822. 31. Fonseca MO, Pang LW, de Paula Cavalheiro N, Barone AA, Heloisa Lopes M. Randomized trial of recombinant hepatitis B vaccine in HIV-infected adult patients comparing a standard dose to a double dose. Vaccine 2005; 23:2902–2908. 32. Wallace MR, Brandt CJ, Earhart KC, Kuter BJ, Grosso AD, Lakkis H, Tasker SA. Safety and immunogenicity of an inactivated hepatitis A vaccine among HIV-infected subjects. Clin Infect Dis 2004; 39:1207–1213. 33. Kroon FP, van Dissel JT, Labadie J, van Loon AM, van Furth R. Antibody response to diphtheria, tetanus, and poliomyelitis vaccines in relation to the number of CD4+ T lymphocytes in adults infected with human immunodeficiency virus. Clin Infect Dis 1995; 21:1197–1203. 34. Kojic EM, Kang M, Cespedes MS, Umbleja T, Godfrey C, Allen RT, et al. Immunogenicity and safety of the quadrivalent human papillomavirus vaccine in HIV-1-infected women. Clin Infect Dis 2014; 59:127–135. 35. Crum-Cianflone NF, Wallace MR. Vaccination in HIV-infected adults. AIDS Patient Care STDs 2014; 28:397–410. 36. Fuster F, Vargas JI, Jensen D, Sarmiento V, Acuña P, Peirano F, et al. Core-HIV Study Group. CD4/CD8 ratio as a predictor of the response to HBV vaccination in HIV-positive patients: A prospective cohort study. Vaccine 2016; 34:1889–1895. 37. Jedicke N, Stankov MV, Cossmann A, Dopfer-Jablonka A, Knuth C, Ahrenstorf G, et al. Humoral immune response following prime and boost BNT162b2 vaccination in people living with HIV on antiretroviral therapy. HIV Med 2022; 23:558–563. 38. Avelino-Silva VI, Miyaji KT, Mathias A, Costa DA, de Carvalho Dias JZ, Lima SB, et al. CD4/CD8 ratio predicts yellow fever vaccine-induced antibody titers in virologically suppressed HIV-infected patients. JAIDS J Acquir Immune Defic Syndr 2016; 71:189–195. 39. Catherine F-X, Piroth L. Hepatitis B virus vaccination in HIV-infected people: A review. Hum Vaccines Immunother 2017; 13:1304–1313. 40. Collin A, Le Marec F, Vandenhende MA, Lazaro E, Duffau P, Cazanave C, et al. ANRS CO3 Aquitaine Cohort Study Group. Incidence and risk factors for severe bacterial infections in people living with HIV. ANRS CO3 Aquitaine Cohort, 2000-2012. PLoS One 2016; 11:e0152970. 41. Martínez-Sanz J, Díaz-Álvarez J, Cancio-Suarez MR, Ron R, Iribarren JA, Bernal E, et al. Expanding HIV clinical monitoring: the role of CD4, CD8, and CD4/CD8 ratio in predicting non-AIDS events. EBioMedicine 2023; 95:104773. 42. Shieh Y, Eklund M, Madlensky L, Sawyer SD, Thompson CK, Stover Fiscalini A, et al. Athena Breast Health Network Investigators. Breast cancer screening in the precision medicine era: risk-based screening in a population-based trial. J Natl Cancer Inst 2017; 109: 43. Castilho JL, Bian A, Jenkins CA, Shepherd BE, Sigel K, Gill MJ, et al. North American AIDS Cohort Collaboration on Research and Design (NA-ACCORD) of the International Epidemiology Databases to Evaluate AIDS (IeDEA). CD4/CD8 Ratio and Cancer Risk Among Adults With HIV. J Natl Cancer Inst 2022; 114:854–862. 44. Chaudhary O, Trotta D, Wang K, Wang X, Chu X, Bradley C, et al. Patients with HIV-associated cancers have evidence of increased T cell dysfunction and exhaustion prior to cancer diagnosis. J Immunother Cancer 2022; 10:e004564. 45. Verboeket SO, Wit FW, Verheij E, van Zoest RA, Kootstra NA, van der Valk M, et al. AGEhIV Study Group. Human immunodeficiency virus (HIV)-negative men who have sex with men have higher CD8+ T-cell counts and lower CD4+/CD8+ T-cell ratios compared with HIV-negative heterosexual men. J Infect Dis 2020; 224:1187–1197. 46. Poizot-Martin I, Allavena C, Duvivier C, Cano CE, Guillouet de Salvador F, Rey D, et al. Dat’AIDS Study Group. CMV+ serostatus associates negatively with CD4:CD8 ratio normalization in controlled HIV-infected patients on cART. PLoS One 2016; 11:e0165774.
留言 (0)