This study is the first to evaluate the effects of US-LSP in the treatment of large-volume BPH with asymptomatic urethral stricture after urethral stricture surgery. According to our research results, US-LSP was a safe and effective procedure that significantly improves LUTS in large-volume BPH. Meanwhile, US-LSP could reduce the risk of SUI in patients with a history of posterior urethral surgery. These results were in line with previous studies [4, 9, 13].
Surgical methods for BPH mainly include transurethral resection of the prostate (TURP), transurethral laser enucleation of the prostate, transurethral laser vaporization of the prostate, OP, and minimal invasive simple prostatectomy (MISP). Prostate volume is a critical factor influencing the choice of surgical methods [6]. According to updated EAU guidelines on the management of non-neurogenic male LUTS, OP and endoscopic enucleation of the prostate (EEP) remain standard treatments for patients with larger prostatic glands [6]. Because simple prostatectomy avoids the transurethral procedure of EEP, the technique is particularly suitable for large-volume BPH patients with concomitant asymptomatic urethral stricture. Compared to OP, MISP including LSP and RASP has the advantage of decreased perioperative complications and as a minimally invasive treatment method has been unanimously recognized for its safety and effectiveness in the treatment of large-volume BPH [14,15,16]. Therefore, in this study, for large-volume BPH with asymptomatic urethral stricture, MISP was employed as the treatment method.
Despite recent technical innovations of MISP, several postoperative problems are still unresolved. Among them, retrograde ejaculation is one of the most frequent problems, which has a major impact on the quality of life in BPH patients, especially in young and sexually active men [17, 18]. To decrease postoperative retrograde ejaculation rates, Quan et al. described, for the first time, US-LSP, which involves the preservation of the prostate urethra and bladder neck, to maintain anterograde ejaculation in the treatment of large-volume BPH following urethral-sparing OP, as described by Dixon et al. in 1990 [10, 19].
In current study, US-LSP could maintain ejaculatory function in a high percentage of patients. The exact mechanism of postoperative retrograde ejaculation remains unclear. It has been suggested that retrograde ejaculation may be caused by the impaired closure mechanism of the bladder neck [20]. Indeed, complete preservation of the bladder neck, together with the parafollicular area, is critical and advocated when attempting an ejaculation function-sparing technique endoscopically [20, 21]. Porpiglia et al. found that the absence of urethral infraction was a predictor of ejaculation recovery, which can be explained by the fact that the urethra underwent a remodeling process that can potentially cause edema or alter the physiological contractions of the urethra during ejaculation in the first months postoperatively [16]. Thus, the low rate of retrograde ejaculation (12%) observed in the current study can be attributed to US-LSP, which preserves the urethra and bladder neck.
Preservation of the prostate urethra not only can improve the rate of antegrade ejaculation postoperatively, but also minimize surgical trauma and perioperative complications [20]. Meanwhile, urethral preservation can reduce the rate of postoperative bladder irrigation, leading to shorter catheterization time, and possibly decreasing the risk of symptomatic urethral stricture [14, 20]. In current study, continuous bladder irrigation was avoided in 33 (84.6%) patients, and no patient reported aggravated urethral stricture and postoperative complications occurred in only 5 (12.8%) patients, including 4 cases with Clavien-Dindo grade 1 and grade 2 and 1 case with grade 3a, which was attributed to the urethral preservation in the US-LSP. Meanwhile, the incidence of postoperative complications was lower than that reported in previous literature on LSP and EEP [22,23,24].
We should realize that BPH patients with a history of posterior urethroplasty have an altered anatomy and urinary continence is tenuous because the external sphincter function was usually compromised by the urethroplasty [1]. The primary continence is maintained by the internal sphincter located at the bladder neck. Therefore, traditional endoscopic surgery carries a high risk of urinary incontinence because of the destruction of the internal sphincter mechanism in BPH patients with a history of posterior urethroplasty [25, 26]. For this reason, experts recommend treating these patients with medical therapy unless BPH surgical treatment is absolutely indicated [27]. Therefore, the patients of the current study required surgical treatment after patients failed medical management of their LUTS. In our study, at 1-month follow-up, only one (5.9%) patient complained of SUI in 17 patients with asymptomatic posterior urethral stricture after posterior urethral stricture surgery, and there was no case of SUI at 6 months, which confirms that preservation of bladder neck is a critical factor for maintaining the internal sphincter mechanism.
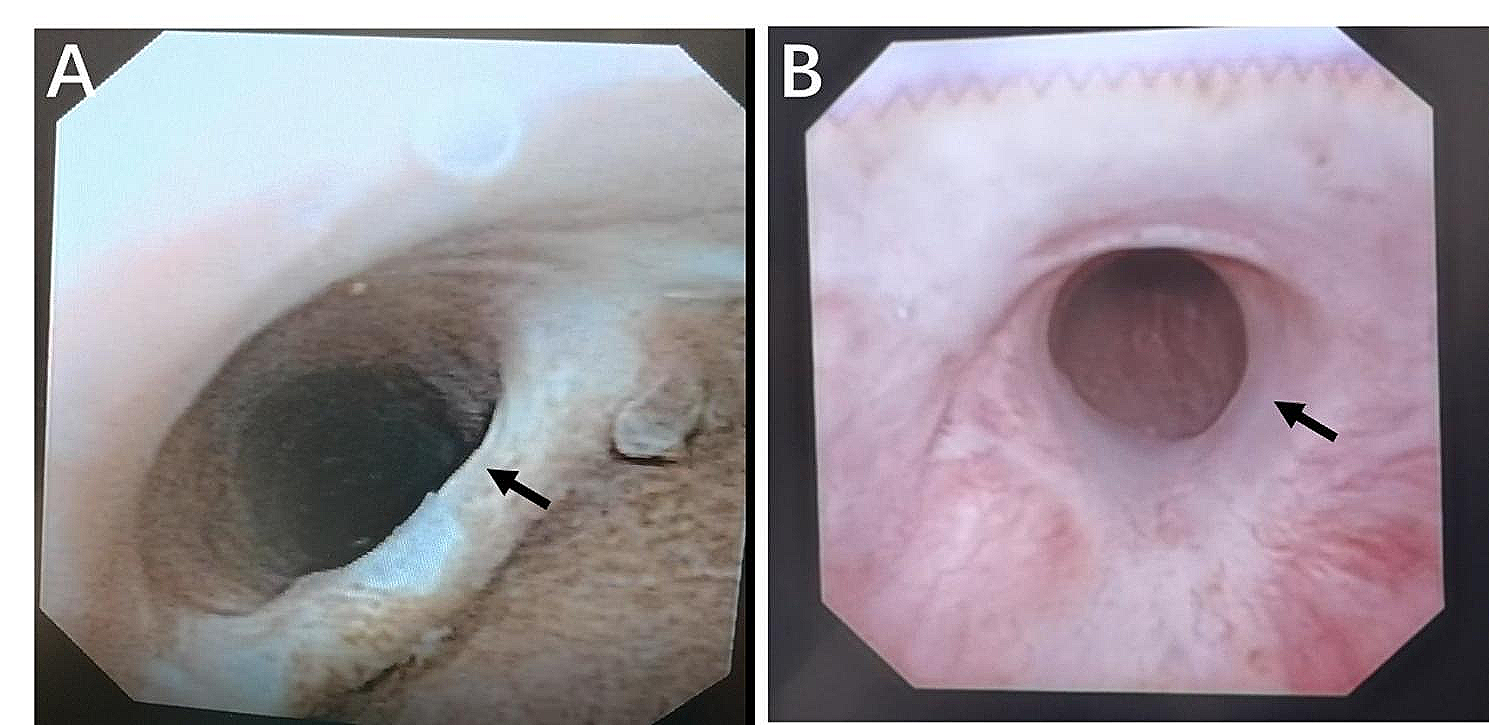
In the current study, 16Fr flexible cystoscopy evaluation confirmed that calibre of the urethral lumen was greater than 16Fr, and the diagnosis of BPH was established after excluding neurogenic dysfunction according to EAU guidelines on urethral strictures [2]. Thus, patients with asymptomatic urethral stricture after urethral stricture surgery did not require repeat urethral surgery but needed BPH surgical treatment because of significant BPH-related LUTS. Our results showed that US-LSP presented significant improvements when compared to baseline in terms of IPSS, QoL, Qmax, and PVR during follow-up, which further confirmed that significant LUTS of patients should be contributed to BPH, not asymptomatic urethral stricture.
Our study has some limitations. Firstly, the limited number of patients is major limitation. Secondly, the relatively short follow-up period for BPH patients with asymptomatic urethral stricture is also a limitation. At last, all surgeries in this study were performed by highly experienced laparoscopic surgeons, so the results cannot be generalized to all clinical centers.




留言 (0)