
記住我


Patient 1 is a White male, born to non-consanguineous parents, who had an abnormal newborn screen (NBS) for SCID. Initial flow cytometry at 9 days of life showed 1 CD3+ cell/µL, 5 CD19+ cells/µL, and 50 CD16/56+ NK-cells/µL. Lymphocyte proliferation in response to phytohemagglutinin (PHA) stimulation was unsuccessful prior to starting ERT due to profound lymphopenia. However, after 4 weeks of ERT the proliferation was detectable, but low, at 22,313 counts/minute (cpm) (< 5% normal). Engraftment of maternal T-cells was not detected. Erythrocyte ADA activity was 0.2 nmol/h/mg protein (normal range 63.0 ± 41.4) and dAXP was markedly elevated at 0.62 µmol/mL of packed red blood cells (pRBCs), or 61.7% of total adenine nucleotides (normal range < 0.002, < 0.2%). Genetic testing confirmed ADA deficiency with a homozygous pathogenic variant in ADA1 [c.956_960del (p.Glu319Glyfs*3)]. Subcutaneous immunoglobulin replacement (SCIG) and antimicrobial prophylaxis with trimethoprim-sulfamethoxazole and fluconazole were started. At 30 days of life, Revcovi was started with an initial dose of 0.2 mg/kg twice weekly, as per manufacturer’s instructions.
The patient developed immune reconstitution of T-cells, B-cells and NK-cells and was able to discontinue antimicrobial prophylaxis and SCIG at around 17 and 37 weeks of ERT, respectively. Revcovi dosing was consolidated to once weekly and the initial total dose remained unchanged as he gained weight. Plasma ADA activity and dAXP levels in pRBCs were measured regularly to ensure appropriate dosing. Between weeks 61 and 67 of therapy, lymphocyte counts and function had fallen despite adequate ADA activity (> 30µmol/h/mL) and detoxification (dAXP undetectable). Due to progressive lymphopenia, declining T-cell function and hypogammaglobulinemia, both SCIG and antimicrobial prophylaxis were restarted. Additionally, the weight-based dose of Revcovi had fallen to 0.16 mg/kg once weekly, so the dose was increased to 0.125 mg/kg twice weekly during week 63. The adjustment of Revcovi dose and frequency re-established normal T-cell function prompting discontinuation of SCIG and antimicrobial prophylaxis. His T- cell counts have remained low, which has previously been noted among patients treated with ERT (ADAGEN) after a peak around 1–3 years [7]. Despite low T-cell counts the patient remained free of significant infections throughout his clinical course. He developed IgE-mediated food allergy to egg. He is currently at the 67th percentile for length and 19th percentile for weight, with a weight-for-length ratio of ~ 3rd percentile that has been consistent over time. He has speech delay with no evidence of hearing loss.
Clinical Presentation: Case 2Patient 2 is a Black male, born to non-consanguineous parents, who had an abnormal NBS for SCID. Immune evaluation showed 159 CD3+ cells/µL, 27 CD19+ cells/µL, 207 CD16/56+ NK-cells/µL, and 11 naïve CD4+ cells/µL. Lymphocyte proliferation in response to PHA stimulation was detectable, but low, at 17,018 cpm (< 5% normal). Engraftment of maternal T-cells was not detected. Erythrocyte ADA activity was undetectable and dAXP was markedly elevated at 0.61 µmol/mL of pRBCs, or 34.8% of total adenine nucleotides. Genetic testing showed 2 pathogenic heterozygous variants in ADA1 [c.632G > A (p.Arg211His) and c.845G > A (p.Arg282Gln)] consistent with ADA deficiency. SCIG and antimicrobial prophylaxis were started. He was hospitalized for pneumonia at 5 weeks of life, with suspicion for pulmonary alveolar proteinosis. He had subsequent resolution of symptoms following initiation of Revcovi (at 7 weeks of life) using 0.2 mg/kg twice weekly [8].
The patient showed progressive increase in lymphocyte counts after starting ERT. Antimicrobial prophylaxis was discontinued at around 18 weeks of therapy after normalization of T-cell function and development of newly formed naïve T-cells in the circulation. SCIG was stopped after 39 weeks of ERT. The dose of Revcovi was increased after 11 weeks of ERT, and the total dose remained unchanged while gaining weight as he continued to show adequate ADA activity and near undetectable dAXP. Now, two years old, he continues to be free of infections while on a Revcovi dose, unadjusted for weight gain due to adequate clinical and biochemical response, of 0.1 mg/kg twice weekly. He is developing normally with most recent growth at the 13th percentile for weight and 32nd percentile for length.
Clinical Presentation: Case 3Patient 3 is a White female, born to non-consanguineous parents, who had two borderline NBSs for SCID. Flow cytometry at 50 days of life showed lymphopenia with 192 CD3+ cells/µL, 9 CD19+ cells/µL, and 22 CD16/56+ cells/µL. CD3+ count had decreased to 169 cells/µL by the time of referral to our institution at 71 days of life. Lymphocyte proliferation in response to PHA stimulation was detectable, but low, at 10,242 cpm (< 5% normal). Engraftment of maternal T-cells was not detected. Erythrocyte ADA activity was absent with increased dAXP concentration at 0.923 µmol/mL of pRBCs, or 40.3% of total adenine nucleotides. Genetic testing revealed two heterozygous variants in ADA1 [c.445 C > T (p.Arg149Trp) and c.956_960del (p.Glu319Glyfs*3)] consistent with ADA deficiency. Antimicrobial prophylaxis with trimethoprim-sulfamethoxazole and fluconazole were started. At 84 days of life Revcovi was started at 0.2 mg/kg twice weekly, as well as SCIG. At 7 months of ERT, the dose and frequency of Revcovi was consolidated to 0.3 mg/kg once weekly.
The patient demonstrated earlier than expected immune reconstitution after 3 weeks of ERT with normalization of T-cell, B-cell, and NK-cell counts and normal proliferation to PHA. Plasma ADA activity at this time was 109.4 µmol/h/mL with 0.214 µmol/mL dAXP concentration in pRBCs (9.7% of total adenine nucleotides). Immunoglobulin replacement was stopped after 8 weeks of ERT and antimicrobial prophylaxis was stopped around 4 months of ERT.
The patient had mild transient transaminitis prior to starting ERT that resolved. She is 17 months old and has been on ERT for 15 months at the time of this report. She is doing well with no infections. She is growing and developing normally with current weight at the 79th percentile and length at the 19th percentile.
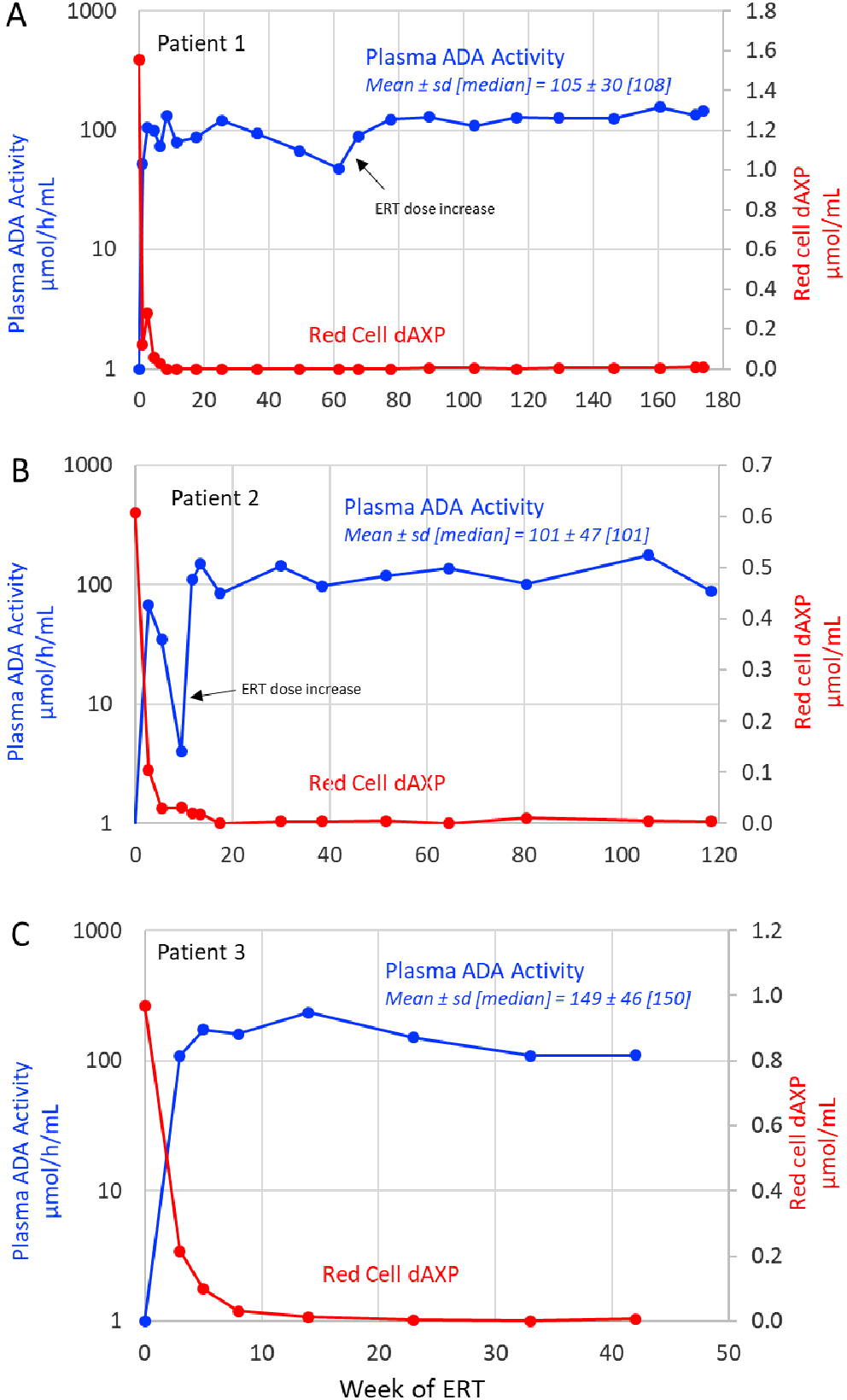
Biochemical StudiesPrior to initiating ERT, all three patients had near absent ADA activity in pRBCs and markedly elevated levels of erythrocyte dAXP, accounting for 40–60% of total deoxyadenosine nucleotides (dAXP are normally undetectable in mature red cells). A trough plasma ADA activity above 30 µmol/h/mL (normally < 0.5 µmol/h/ml in healthy individuals) is recommended by the manufacturer in order to reduce pRBC dAXP to less than 0.01 µmol/ml [9]. The plasma ADA threshold was rapidly achieved in all three patients, with median levels exceeding 3–5 fold the suggested trough while on Revcovi (Fig. 1A-C). In patient 2, plasma ADA activity declined transiently to 4 µmol/h/ml at week 9 owing to suspected incorrect home administration, but returned to effective levels after the recommended dose of Revcovi was restored at week 11 (Fig. 1B). In patients 1 and 3, red cell dAXP declined steadily, becoming negligible by week 8 of treatment in patient 1 and between weeks 8 and 14 in patient 3 (Fig. 1A & C). Elimination of dAXP in patient 2 was delayed until week 17 owing to the transient decline in plasma ADA activity (Fig. 1B).
Fig. 1
Biochemical Studies. The plasma ADA activity and pRBC dAXP concentration for patient 1 A, patient 2 B and patient 3 C. All patients had a high dAXP concentration prior to initiating therapy and achieved rapid detoxification and maintained a dAXP concentration below 0.01 µmol/mL throughout treatment. All patients maintained ADA activity well above the goal of 30 µmol/h/mL. Patient 1’s ADA activity gradually fell from 120 to 48 µmol/h/mL, but it increased again following Revcovi dose escalation. Patient 2 had a brief drop below goal at week 9 likely related to home-dosing error, but remained above goal thereafter
Immune ReconstitutionAfter initiating ERT, lymphocyte counts rapidly improved in all patients. An increase was seen first in NK-cell and B-cell subsets, followed by T-cells in the first 2 patients. Unexpectedly, patient 3 had normalization of T-cells (including naïve) by the third week of ERT, while it took longer to achieve T-cell reconstitution in patients 1 and 2 (Fig. 2A-C). NK-cell numbers normalized within 3–5 weeks of therapy for all patients. B-cells normalized by 3 weeks in patients 1 and 3. In patient 2, B-cells increased steadily after starting therapy, and are now in the normal range.
Fig. 2
Immunophenotyping. Lymphocyte counts for patient 1 A, patient 2 B, and patient 3 C. Patients 1 & 2 showed improvement with reconstitution at around 2 months of ERT, whereas patient 3 developed full immune reconstitution at 3 weeks. T-cells: CD3+, B-cells: CD19+, NK-cells: CD16/56+
Naïve T-cells (CD4/CD45RA/CD62L+) first appeared at week 8 of therapy in patient 1, week 9 in patient 2 and week 3 in patient 3. T-cell function, as measured by proliferation in response to PHA, normalized by week 11 in patient 1, week 13 in patient 2 and by week 5 in patient 3. T-cell reconstitution was evident 11 weeks into ERT for patient 1, with progressive improvement over time, however, by week 67 all subsets subsequently declined. T-cells had decreased to 262 cells/µL, and T-cell function was also depressed, despite adequate ADA activity and undetectable pRBC dAXP. The Revcovi dose was increased at this time from 0.16 mg/kg weekly to 0.13 mg/kg, twice weekly. He demonstrated a favorable response to this dose increase, with normalization of T-cell function. After 2 years of Revcovi his T-cell count was 699 cells/µL while receiving 0.20 mg/kg divided twice weekly. However, recently T-cell counts have begun to decline (218 CD3+ cells/µL) despite appropriate ADA plasma activity and undetectable dAXP levels. Reassuringly, T-cell function remains normal. In patient 2, the lymphocyte subsets remain sufficient with normal T-cell function. In patient 3, all lymphocyte subsets remain completely normal and T-cell function remains intact (Fig. 3 C). Lymphocyte subsets for all patients by weeks of ERT can be found in Table 1.
Fig. 3
T-cell Subsets and Mitogen Proliferation. A Patient 1’s T-cell numbers and mitogen proliferation. T-cell function declined over the first year, but then increased again after an increase in dose of ERT. B Patient 2’s T-cells numbers and mitogen proliferation have improved since starting ERT and are now normal. C Patient 3’s T-cell function and counts have normalized since week 3 of ERT. Naïve T-cells: CD4/CD45RA/CD62L+
Table 1 Lymphocyte subsets by week of ERT for all patients. Refer reader to Shearer et. al. for lymphocyte reference ranges [17]Humoral immune function normalized with Revcovi. All patients showed evidence of endogenous immunoglobulin production (rising IgM) and B-cell class switching (rising IgA levels) (Fig. 4). IgG levels measured more than 6 months from the most recent SCIG infusion were 276 mg/dL, 703 mg/dL, and 300 mg/dL for patients 1, 2 and 3, respectively. No patient has developed antibodies to Revcovi. All patients received age appropriate non-live pediatric vaccines and demonstrated normal humoral immune responses.
Fig. 4
Humoral Immunity. All patients show evidence of endogenous immunoglobulin production and B-cell class switching with rising IgM and IgA levels
ThrombocytosisPatients 1 and 2 experienced significant, but transient thrombocytosis soon after starting Revcovi (Fig. 5). Patient 1’s platelet count peaked 2.5 weeks into ERT at 1,165,000/µL. Patient 2’s platelet count peaked 3 weeks into ERT at 1,573,000/µL. Patient 3 had thrombocytosis prior to starting ERT. The platelet counts in all patients decreased over the course of ERT and have nearly normalized with most recent values being around 400,000/µL. The patients experienced no thromboembolic events. ERT was not altered due to the thrombocytosis, and no anticoagulation treatment was given.
Fig. 5
Thrombocytosis. Patients 1 & 2 experienced transient profound thrombocytosis in the first few weeks of therapy. Thrombocytosis quickly resolved, and platelet counts continue to be at the upper limit of normal
留言 (0)