Progress towards the participation indicators
The LPMF sets forth the aspiration of achieving a “fuller and more influential involvement of affected people in what relief is provided to them, and how” [37]. According to the framework, this can be accomplished by ensuring that CAP actively shape and participate in humanitarian response initiatives [37]. . The findings of this study indicate that despite digital health practitioners having a positive perception of participatory action and the benefits it can yield, participatory events were primarily limited to specific, pre-defined project milestones rather than spanning the entire project lifecycle or at the pre- or post-intervention points. In general, participation within the humanitarian digital health sphere manifested as focus groups, surveys, and interviews, and included assessments and testing. CAP influence within these events was curtailed and limited according to organisational boundaries. For the most part, CAP were not actively engaged in needs assessments, prioritisation decisions, or shaping humanitarian and health policies. As a result, CAP held limited influence or power over problem identification, goal definitions, strategy selection or policy shaping. However, notable exceptions were identified, where co-creation activities were enacted with CAP to gain insight into broader lifestyle and digital realities to inform project planning and decisions prior to design phases. , Despite these noteworthy instances, in the context of the LPMF, this study found the overall progress towards participation indicators remains far from a revolution.
Summary of emerging themes
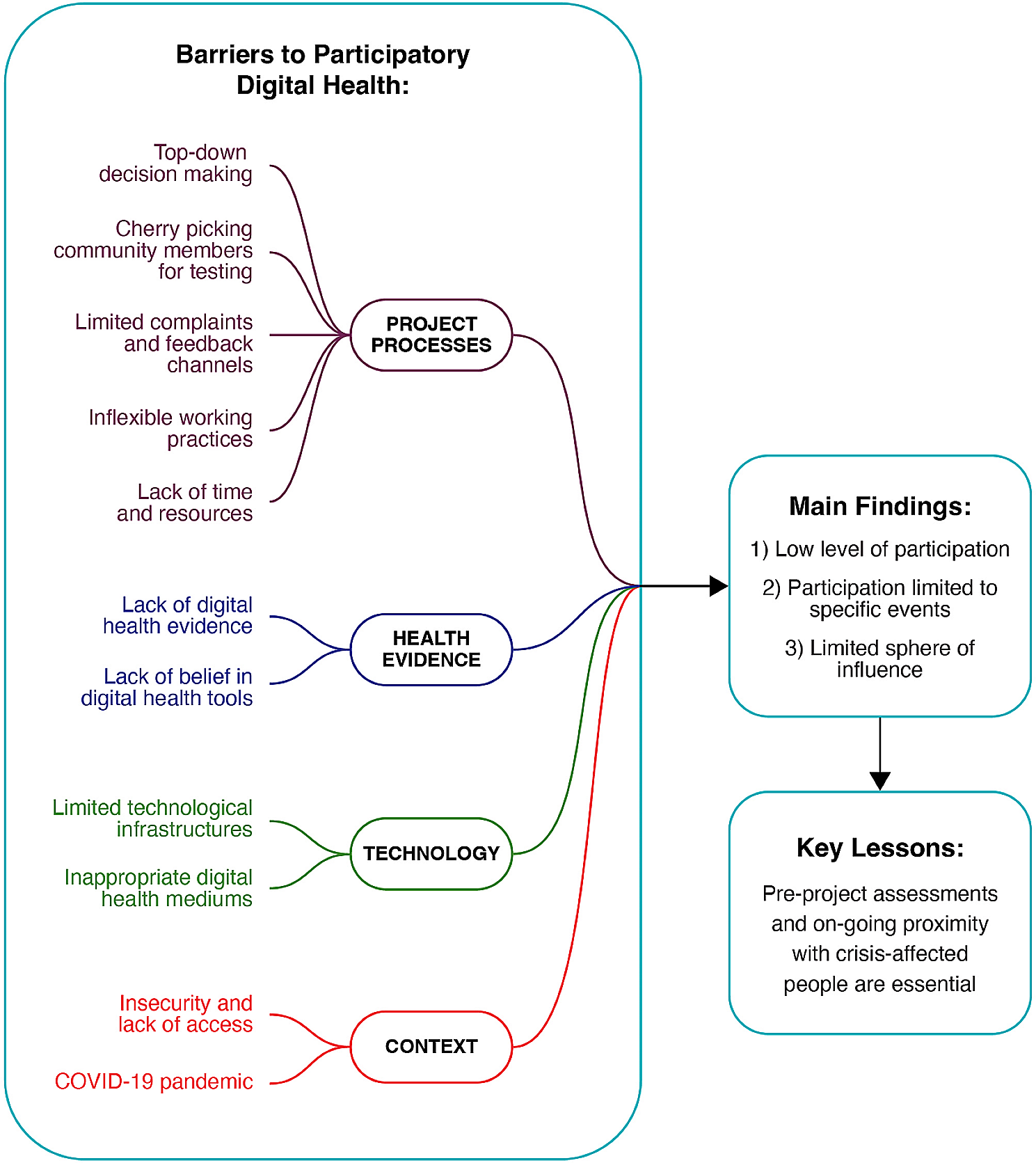
Participatory barriers emerged as major themes: Project processes, technological limitations, contextual issues, and a lack of health evidence all influenced the participatory reality of digital health projects in LMIC crisis contexts. Key participatory lessons for successful digital health interventions were acknowledging the importance of and acting on in-depth pre-intervention assessments, in conjunction with maintaining ongoing proximity and meaningful engagement with CAP during and after interventions to understand the intervention against evolving humanitarian needs. Our findings indicate that substantial disparities persist between these participatory best practices and the realities of digital health humanitarian action [46, 47].
Systemic issues
Many of our thematic findings stem from systemic issues. This is symptomatic of the challenges with the current response ecosystem [16, 17] and, thus, distracts us from the human dimension that should be at its core. As a result, incorporating the fundamental right of CAP to participate in decisions that affect them meaningfully has become deprioritised. Consequently, this study emphasises the necessity to move away from a systemic master, and instead towards a person-centred approach. Enhancing collaboration between humanitarian health actors and CAP could surmount identified obstacles and harness the potential offered by digital health tools in addressing humanitarian crises. As an alternative focus, integrating the participation of CAP through the key benchmarks laid out in the Core Humanitarian Standard [48] unlocks a number of ethical gains, such as respect for cultural and contextual norms, equitable representation and diversity inclusion, as well as accountability, non-maleficence, beneficence and mutual reciprocity, informed consent and decision-making powers.
Overcoming participatory barriers
Barriers to CAP participation caused by project processes include limited time and resources, inflexible working practices, top-down decision-making, and cherry-picking community involvement. Drawing upon the experiences documented by Fitz-Gerald and others [16, 17], our study underscores the persistent challenges of the paternalistic humanitarian system acting in its own interests and restricting the quality and quantity of participatory events [49]. This highlights the tensions between the dominant system approach, and how neglecting contextual and human dimensions undermines adherence to humanitarian principles of humanity, impartiality, neutrality, and independence [50] and impedes progress towards meaningful transformation.
Our research echoes the concerns raised by Ehrenzeller [51] and others [52,53,54] regarding the intersectionality of localisation required to effect change. To overcome these barriers, digital health projects should embrace all dimensions of the Localisation Agenda, centred by the Participation Revolution, including decentralising funding, visibility, relationship and capacity building [53]. Enacting these dimensions simultaneously can support the development of a more human-centric approach at all stages and overcome existing constraints.
A lack of digital health evidence posed a barrier for both digital health providers and CAP. This limitation led providers to establish parallel data collection and reporting systems. In turn, this was said to be responsible for community scepticism and lack of trust rather than acceptance of and participation in digital health tool interventions. This contrasts with findings from other feasibility studies [55,56,57] that showed positive community assessments of digital health tools, highlighting the need for further exploration.
To address this lack of health evidence, digital health projects could actively engage healthcare providers and CAP in recognising the potential impacts of digital tools on health outcomes. Implementing co-production initiatives presents an opportunity for this and can foster interest and trust by reporting outcomes and interpreting results collaboratively. This approach can promote a learning culture that strengthens support for digital health initiatives and ensures their alignment with real-world challenges.
In settings with considerable technological limitations, as observed in several studies [35, 58], barriers such as poor connectivity pose a considerable challenge to both digital health interventions and digital participatory action. When technology and infrastructures do align, digital health tools become powerful facilitators in addressing specific health issues, particularly for stigmatised problems such as mental health, offering privacy and discretion [59]. This represents a considerable strength for digital health tools, considering the high burden of mental health issues found within crisis contexts [60, 61].
However, as our exploration highlights, the reality of aligning tools within limited techno-ecosystems is not always feasible and underscores the importance of designing interventions according to local contexts. Incompatible digital tools that are not tailored to the hosting environment are indicative of hierarchical provider-led decision-making rather than user-led approaches prioritising the needs and desires of CAP [62, 63]. As WHO outlines, digital tools are only a platform, not a means to an end [42]. A greater understanding of existing digital behaviours in relation to socio-economic aspects, such as gender, ownership, and literacy can inform appropriate digital platform selections and local hosting capabilities [61]. An important consideration here is that certain contexts may not be viable for digital health tools, and traditional methods may be more appropriate. This decision should be locally led.
As outlined by other studies [64, 65], in regions with ongoing conflicts, accessibility challenges between responders and CAP can hinder access to services [66] as well as traditional participatory activities [67,68,69]. In such contexts, greater community engagement and improved participation can provide protection and access to humanitarian responders. This must go hand-in-hand with principled action but can act as a mechanism in which assistance can continue to be delivered to communities within these areas.
However, given the shrinking humanitarian space, increasing human rights violations, and attacks on responders [67], proximity with CAP may not always be possible. In these cases, digitalised health services offer the potential to transcend some of these barriers virtually, as demonstrated during the emergence of the COVID-19 pandemic. The pandemic served as a catalyst for digitalising health and humanitarian sector services, and as a result, digital interventions may have extended the reach of health services and fostered greater inclusion of CAP in humanitarian response efforts [70]. This is a notable achievement and may become increasingly important in the future. Establishing best practices and effective digital health platforms that also incorporate digitalised participatory engagement opportunities would be highly advantageous in this evolving landscape.
It is crucial to acknowledge that while increased digitalisation may have broadened inclusion for some communities in accessing services, it risks excluding others [71, 72]. As outlined by Boza-Kiss et al. [73], the lack of access to digital technology in low-income crisis contexts disproportionately affects socio-economically disadvantaged communities. Consequently, balancing the benefits of digital health solutions with addressing disparities is crucial to ensure equitable and effective support for all CAP during crises.
Implications
Insufficient CAP participation in digital health projects has several critical implications. Firstly, poor participation with CAP can result in unrepresentative local information lacking cultural and contextual nuances, limiting project design and development. Secondly, the lack of engagement may limit the targeted users’ adoption of digital health tools. Thirdly, without the meaningful involvement of CAP, digital health tools may not be fit for purpose, technologically, economically, ethically, or socially. This may mean that intended groups are not reached with humanitarian response efforts or that ethical lines are crossed, which could result in adverse outcomes.
This study’s findings align with existing literature and best practices in health and humanitarian endeavours [74, 75] in highlighting two critical lessons learned for the success of digital health projects: Firstly, conducting comprehensive population and context assessments with CAP before project initiation is crucial for ensuring appropriate design and implementation: Building on the lessons learned from the West African Ebola outbreak [76, 77] and COVID-19 Pandemic [78, 79], we emphasis this as an ethical approach for deeper, more holistic understanding of community needs. In this way, CAP participation can help to reduce power imbalances and systemic paternalism whilst bridging the divide between global resources and local solutions [80].
Secondly, maintaining close proximity and ongoing interaction with CAP throughout and after humanitarian actions is essential [66, 81,82,83]. Previous studies have shown that it is not enough to simply develop and implement a digital health tool [84]. Instead, ongoing engagement is required to facilitate trust and legitimacy whilst enabling continuous adaptation and improvement, maximising the potential benefits of digital health interventions within evolving and dynamic environments. Incorporating these lessons into digital health projects can uphold a rights-based approach that increases accountability to CAP whilst contributing to more effective and impactful response efforts.
Strengths and limitations of the study
In seeking to understand the organisational perspective of the Participation Revolution, this study engaged with digital health and humanitarian organisations, recognising their pivotal role and access to resources required for an accountable and effective response. As highlighted in much literature, the interest of CAP to participate is high [85], and whilst our study offers a valuable organisational perspective, the limitations of not including CAP in this study are acknowledged. Participatory rights are the cornerstone for the realisation of numerous fundamental ethical and human rights, including, but not limited to, the right to non-discrimination, the right to healthcare and the right to freedom of expression. Further research in this field should explore this topic from the CAP perspective, exploring CAP’s awareness of their rights in relation to health, digital and humanitarian response efforts. Investigating participatory evaluation mechanisms as indicators of success, measured by CAP, for humanitarian and digital health interventions could contribute towards the evolving discourse on inclusive and rights-based humanitarian and digital health interventions. Furthermore, given the diversity of health issues addressed by technology, additional analysis of these and their crisis contexts to understand their potential participatory opportunities could enhance this research field.
We recognise this study’s small sample size as a limitation for generalisability and as such cannot tease out differences between technology types, health issues, and crisis contexts. However, considering this against the diversity of CAP and crisis contexts globally, we consider this study a baseline for greater exploration in this sphere. Considering the complexity of the topic, this study’s strength lies in the rich diversity of perspectives from several humanitarian crises, crisis context types, types of digital health tools and health issues.
The lack of health evidence from digital health tools within humanitarian contexts challenges the very notion that they benefit health outcomes. Further research to demonstrate their ability to affect positive health change could garner greater traction as well as highlight opportunities for further CAP participation in response efforts.









留言 (0)