
記住我


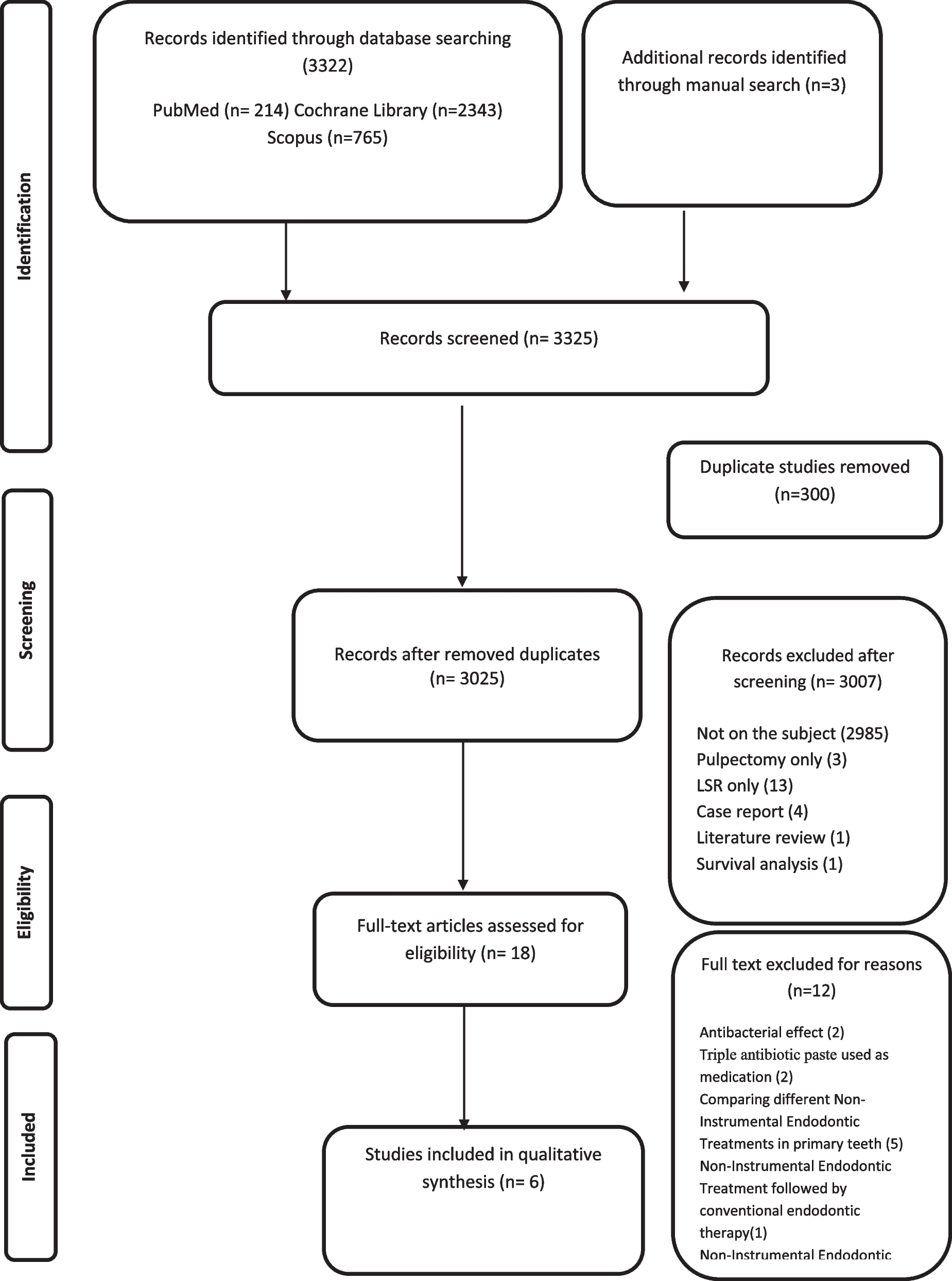

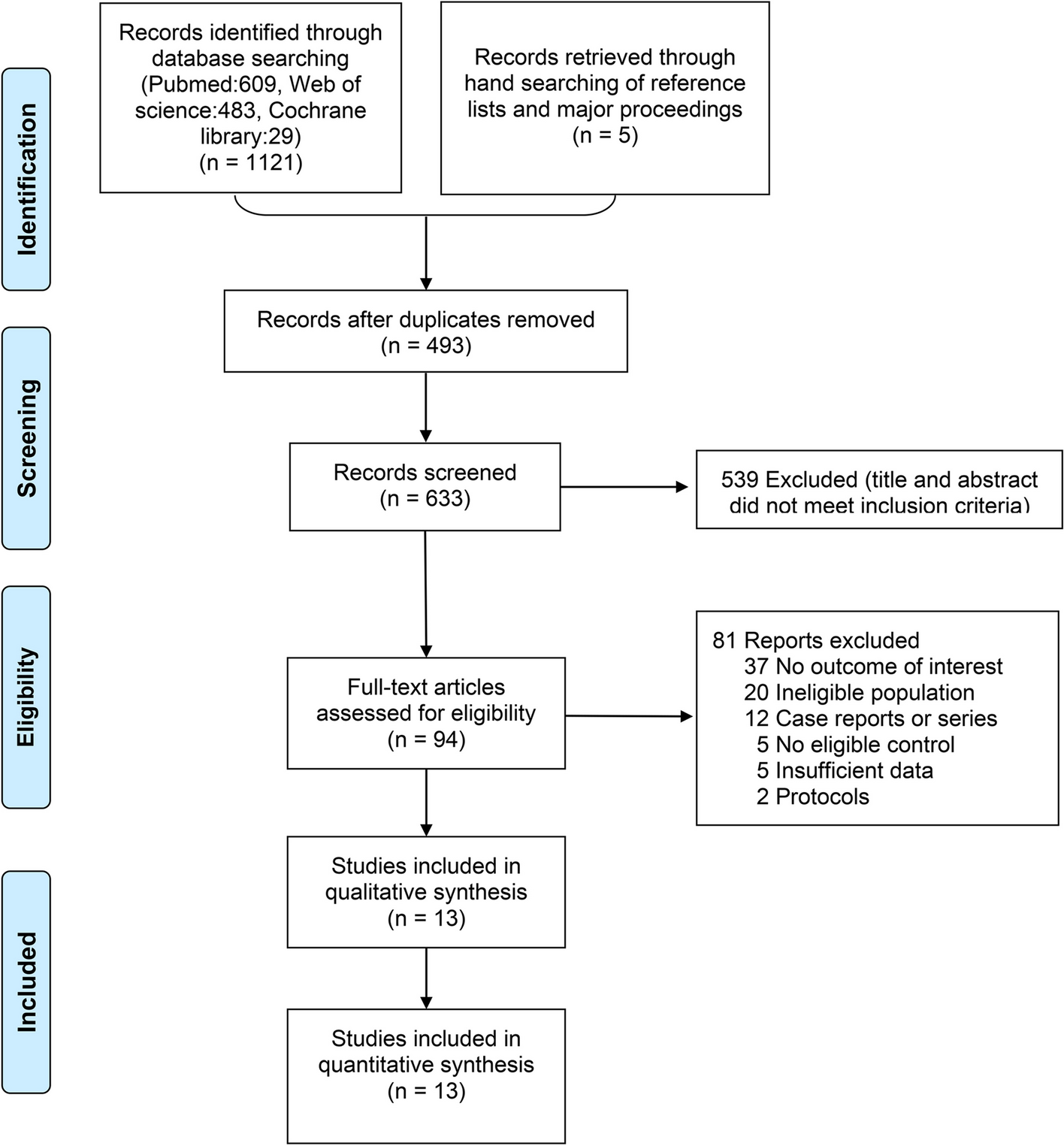

Details about the process of identification, inclusion, and exclusion of studies are summarized in Fig. 1, Table 2.
Fig. 1 Table 2 Overview of inclusion and evaluation criteria of the selected studies
Table 2 Overview of inclusion and evaluation criteria of the selected studiesAll 3322 articles retrieved from the electronic databases were screened by Mendeley Desktop software 1.19.4, which served as a facilitating tool in the organization of the references.
Of these 3322 initial references initially identified, 300 were duplicates and 3 were identified through other sourcing. About 3007 records were excluded by screening for title and abstract, ending with eighteen articles for full-text reading. Twelve records were excluded. Therefore, six studies were included in the present systematic review.
A standardized eligibility drawing sheet was used to register the reasons for exclusion at this stage.
The reasons for the exclusions are described in Fig. 1.
As the data were very heterogeneous, it was difficult to do the meta-analysis. All the studies were subject to qualitative analyses.
Study characteristicsTable 3 presents the characteristics of the six selected searches for the present systematic review.
Table 3 A summary of the descriptive characteristics of the included studies (N = 6)The six included searches were published during the last 10 years and were performed in four different countries: India [14, 19, 20], Thailand [15], Argentina [21], and Brazil [18].
The selected studies included 283 primary molars, of 213 children aged between 3 and 9 years, treated by NIET and conventional pulpectomy, and had follow-up periods ranging from 1 month to tooth exfoliation.
The inclusion and evaluation criteria of the selected studies are summarized in Table 2.
All the clinical procedures were performed under rubber dam isolation [14, 15, 18,19,20,21].
In each tooth, a cavity was prepared depending upon the extent of the lesion, and caries were removed with no overhanging tooth structure left in to provide good access to the coronal pulp.
Only the pulp chamber was removed and no root canal treatment was performed on the included teeth receiving NIET [14, 15, 18,19,20,21].
For teeth receiving conventional endodontic treatment, the radicular pulp was removed using K-files in four studies [15, 18, 20, 21], and H-files in two studies [14, 19].
For NIET technique, the mixture of metronidazole, ciprofloxacin, and minocycline (1:1:1) was used in two studies [15, 21], the mixture of metronidazole, ciprofloxacine, and minocycline (1:3:3) in one study [20], the mixture of metronidazole, ciprofloxacin, and Cefixime (1:1:1) in one study [14], the mixture of ornidazole, ciprofloxacin, and Cefaclor in one study [19], and CTZ paste which is a mixture of chloramphenicol, tetracycline and zinc oxide eugenol (1:1:2) in one study [18].
In all the included studies [15, 17,18,19,20,21] using 3 Mix, carriers: macrogol and propylene glycol were added to the different antibiotics powder mixtures until a consistent non-friable paste was obtained. For conventional endodontic therapy, several canals filling pastes were used: Vitapex, Zinc oxide eugenol cement, Maistro-Cappuro paste, Calcium hydroxide paste, Zinc oxide-ozonated oil (ZnO-OO), Propolis liquid-mixed Endoflas powder [15, 17,18,19,20,21].
Before placement of the 3 Mix-MP in teeth receiving NIET, irrigation was done with 1% sodium hypochlorite [19], 2.5% sodium hypochlorite [15, 21], 3% sodium hypochlorite [20], and normal saline [19].
In conventional endodontic therapy, the following irrigants were used: 5% sodium hypochlorite [14], 3% sodium hypochlorite [20], 2.5% sodium hypochlorite [15], 1% sodium hypochlorite [18, 21], and 1% sodium hypochlorite with normal saline [19].
Final teeth restorations were done using stainless steel crowns in five studies [15, 17, 19,20,21] and with composite restoration in only one study [18].
Teeth were sealed with glass ionomer cement and then restored with stainless steel crowns in one visit in two studies [15, 20], sealed with glass ionomer cement at the same visit then restored with stainless steel crowns after 24 h in one study [17], sealed with glass ionomer cement at the same visit then restored with stainless steel crowns after 15 days in one study [19], filled with a temporary dressing (zinc oxide eugenol) and then restored with stainless steel crowns after 7 days in one study [21], restored only with composite restoration in one study [18].
Main outcomesThree studies showed that the radiographical success rate of conventional pulpectomy was higher than the NIET [14, 18, 19].
No significant difference was found between NIET and conventional pulpectomy technique in the two included studies [20, 21] whereas one study showed a significant difference between both techniques with better results for endodontic therapy [15].
At 6 months follow-up, the clinical success rate of conventional pulpectomy ranged from 89.4 to 100%, while for NIET, the clinical success rate ranged from 38.8 to 100%.
At 12 months follow-up, the clinical success rate of conventional pulpectomy ranged from 89.4 to 100%, and for NIET, it ranged from 33.33 to 96%.
Concerning the radiographical success rate, at 6 months observation period, the radiographical success rate of conventional pulpectomy ranged from 80 to 100% and for NIET technique from 20 to 84%. At 12 months follow-up, the radiographical success rate of conventional pulpectomy ranged from 80 to 100% and for NIET technique from 20 to 84%.
Risk of bias appraisalThe risk-of-bias assessment summarized in Fig. 2 was generated by the robvis (visualization tool) which is a web application designed for visualizing risk-of-bias assessment [16]. All studies stated acceptable reasons for missing data, with no major missing outcome data.
Fig. 2
The overall quality of the randomized clinical trials included in the present review was moderate.
Three studies; Daher et al. 2015 [18], Doneria et al. 2015 [19], and Zacharczuk et al. 2019 [21], were considered as “high risk of bias”.
In these studies, a lack of information about the random sequence generation and allocation was reported and no blinded clinical evaluations were noted in these studies.
The study of Agrawal et al. 2011 [17], and the study of Divyia et al. 2019 [20] were classified as having “unclear risk of bias” due to some concerns reported in the randomization process and the outcomes measurement.
Only one study, Nakornchai et al. 2010 [16], was classified as having a low risk of bias.
Meta-analysisOf the 6 included studies in the present systematic review, only 4 were included in the meta-analysis (Fig. 3).
Fig. 3
Forest plot of treatments clinical and radiographic parameters at 6 and 12 months
At 6-month follow-up, there was no significant difference in the clinical and radiographical success rates between the non-instrumentation endodontic treatment and the conventional endodontic therapy in primary molars.
The clinical results at 6 months showed; a relative risk (RR) = 0.99, with a 95% CI 0.94, 1.04, and a P value = 0.64 with I2 = 0%.
The radiographical results at 6 months showed; a relative risk (RR) = 0.91, with a 95% CI 0.78, 1.06 and a P value = 0.23 with I2 = 9%.
At 12-month follow-up, no significant difference in the clinical and radiographical success rates between the non-instrumentation endodontic treatment and the conventional endodontic therapy were reported.
The clinical results at 12 months showed; a relative risk (RR) = 0.97, with a 95% CI 0.90, 1.04, and a P value = 0.34 with I2 = 0%.
The radiographical results at 12 months showed; a relative risk (RR) = 0.87, with a 95% CI 0.65, 1.18 and a P value = 0.38 with I2 = 64%.
A meta-regression was not performed as it is not recommended when the number of the included studies is small [22].
留言 (0)